1889
Detection of Type 2 Diabetic Peripheral Neuropathy using Lumbosacral Nerve Root Diffusion Tensor Imaging1China-Japan Friendship Hospital, Beijing, China, 2Philips Healthcare, Beijing, China
Synopsis
Keywords: Peripheral Nerves, Diabetes, DTI
Motivation: Electrophysiology is the gold-standard tool to diagnose diabetic peripheral neuropathy (DPN), but it is invasive. We try to find a convenient and reliable technique for diagnosing DPN.
Goal(s): The study aimed to reveal whether DTI of the lumbosacral nerve roots could be used to detect DPN.
Approach: Using a 3T MRI scanner to get the DTI parameters of lumbosacral nerve roots from 2 diabetic patients with and without DPN, respectively, and analyze data using statistical methods.
Results: DTI of lumbosacral nerve roots can detect whether peripheral nerve injury occurs in diabetic patients.
Impact: DTI of lumbosacral nerve roots can not only detect whether peripheral nerve injury occurs in diabetic patients but also quantitatively describe the degree of peripheral nerve injury and has the potential to evaluate the nerve changes after treatment in DPN patients.
Introduction
Electrophysiology is recommended as the gold-standard tool to diagnose diabetic peripheral neuropathy (DPN). However, electrophysiology is not able to detect focal neuropathy at an early and subclinical stage and is time-consuming, invasive, and might be affected by many factors such as the proficiency and subjectivity of the operator. Therefore, there is a need to find a convenient, reliable technique for the diagnosis of DPN.Objective
To evaluate the lumbosacral nerve roots of patients with type 2 diabetic peripheral neuropathy by MRI, clarify whether MRI of the lumbosacral nerve roots can be used to detect DPN and explore the value of lumbosacral nerve root MRI in the diagnosis of DPN.Method
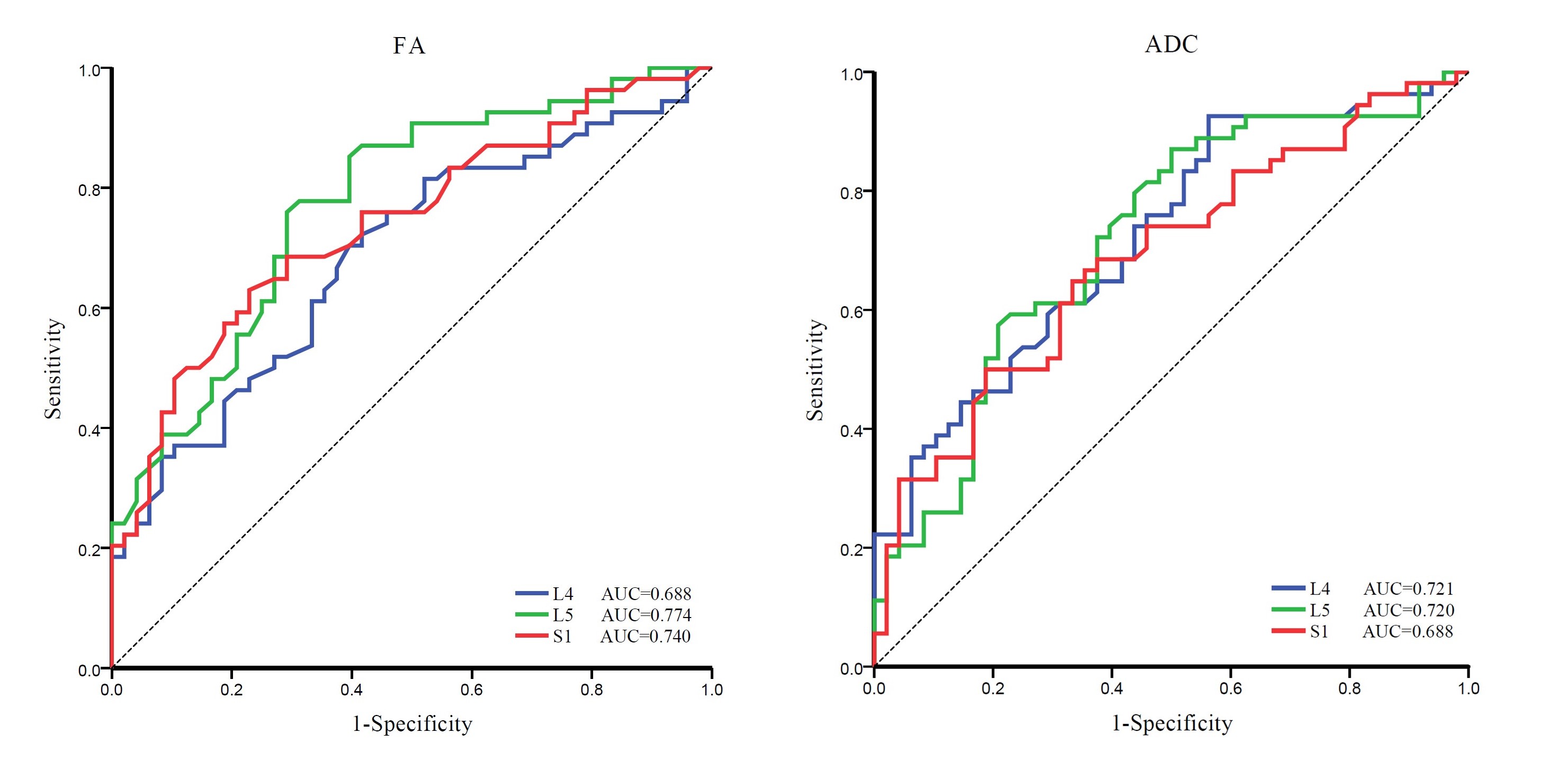
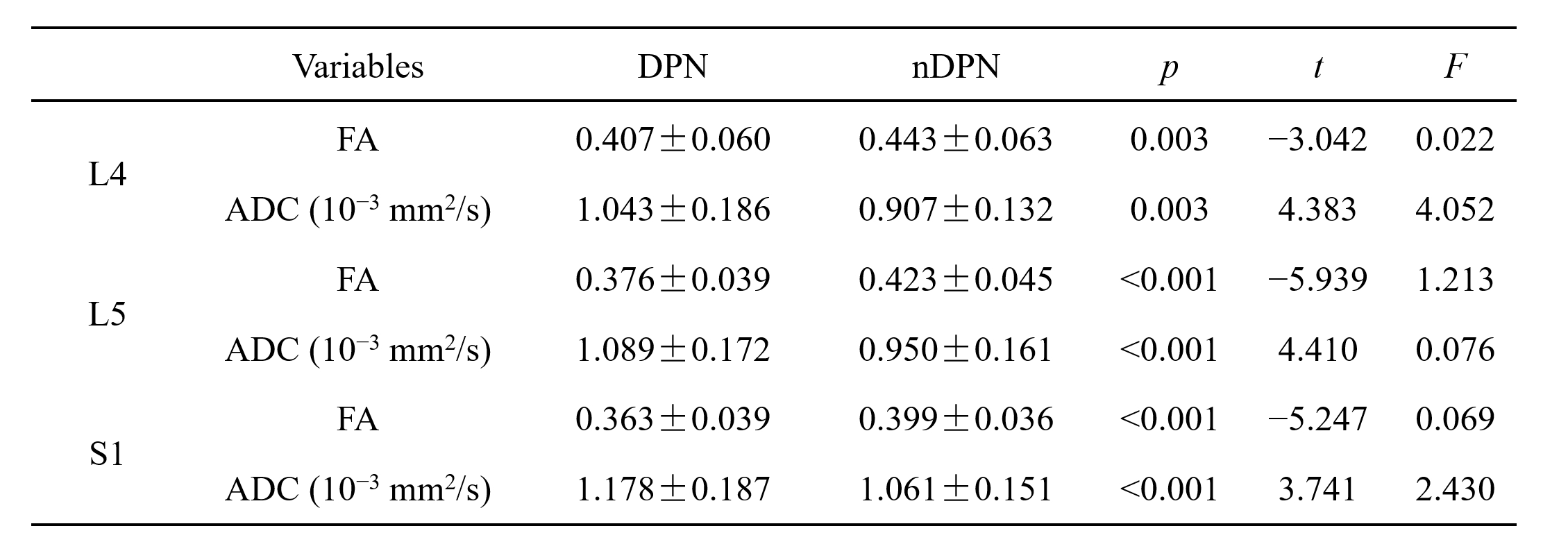
Thirty-two type 2 diabetic patients with DPN and twenty-eight type 2 diabetic patients without DPN were investigated with a 3T MRI scanner (Ingenia, Philips Healthcare, Best, Netherlands). DTI with L4, L5, and S1 nerve root tractography was performed. Fractional anisotropy (FA) and apparent diffusion coefficient (ADC) values were measured from tractography images and compared between groups. Diagnostic value was assessed using receiver operating characteristic (ROC) analysis. The Pearson correlation coefficient was used to explore the relationship between DTI parameters and clinical data and electrophysiology parameters. P<0.05 was considered statistically significant.Results
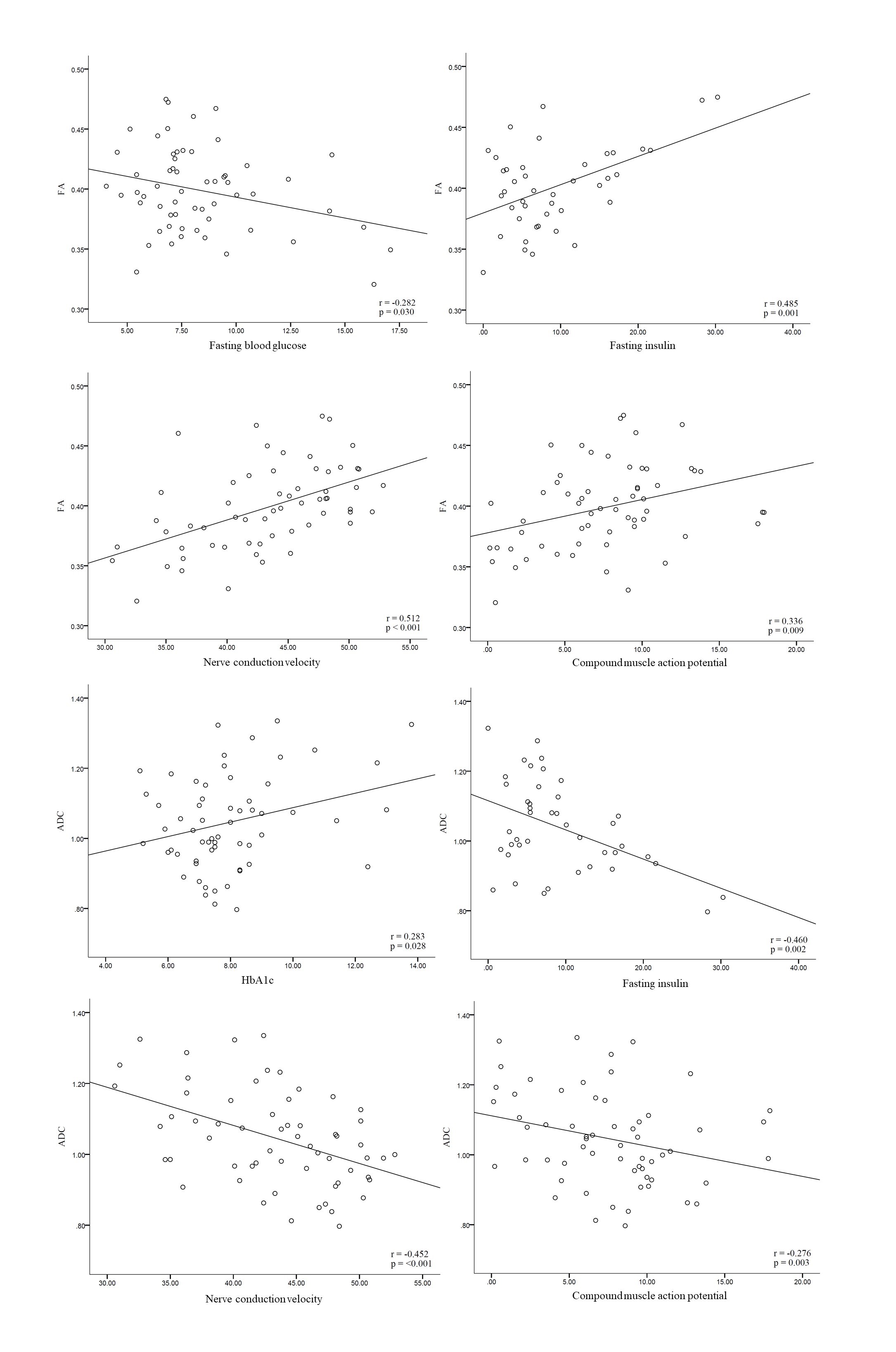
In the DPN patients, FA was decreased, and ADC was increased compared with the values of diabetic patients without DPN in L4~S1 levels (P<0.01). FA of the L5 nerve root displayed the best diagnostic accuracy in distinguishing the DPN from diabetic patients (AUC=0.774, sensitivity=75.9%, specificity=70.8%).Correlation analysis of clinical data revealed a strong positive relationship between the FA values and fasting insulin levels (r = 0.485, P = 0.001), while ADC values were inversely related (r = -0.460, P = 0.002). Furthermore, FA values were weakly inversely correlated with fasting blood glucose levels (r = -0.282, P = 0.030), and ADC values had a weak positive correlation with glycosylated hemoglobin levels (r = 0.283, P = 0.028).
From electrophysiological assessments, both FA and ADC values exhibited significant correlations with the results (P < 0.05). The strongest association was found between FA values and nerve conduction velocity (r = 0.512, P < 0.001).
Discussion
In our research, we focused on the diffusion metrics of the lumbosacral nerve roots, diverging from the traditionally studied distal peripheral nerves as reported in prior literature [1-3]. The selection of lumbosacral nerve roots presents several technical benefits, such as superior image quality and the presence of larger diameters coupled with substantial peripheral fat, which facilitate more accurate measurements. In addition, some believe that diabetic damage first targets the neuron perikaryal that resides in the dorsal root ganglia and acts to support the axons instead of peripheral axons and their associated Schwann cells [4]. From this view, the detection of neural damage by measuring lumbosacral nerve roots, which include dorsal root ganglia, may be a better choice.The ROC analysis revealed that fractional anisotropy (FA) was the most precise DTI metric for diagnosing diabetic peripheral neuropathy (DPN), with the FA of the L5 nerve root presenting an AUC of 0.774. Corroborating experimental research suggests that FA is closely associated with axonal density [5,6], while changes in the apparent diffusion coefficient (ADC) are more reflective of variations in myelin density and thickness [7]. Given that DPN predominantly involves axonal loss rather than demyelination [8,9], our findings endorse the superiority of FA in distinguishing DPN patients.
Among all clinical data, DTI parameters correlate most with fasting insulin levels. This is mainly due to the neurotrophic effect of insulin [10].
Conclusion
DTI has been demonstrated to be a valuable tool not only for the detection of peripheral nerve injury in patients with diabetes but also for providing a quantitative assessment of the severity of such injury. It has the potential to evaluate the nerve changes after treatment in DPN patients.Acknowledgements
No acknowledgement found.References
[1] Vaeggemose, M.; Pham, M.; Ringgaard, S.; Tankisi, H.; Ejskjaer, N.; Heiland, S.; Poulsen, P.L.; Andersen, H. Magnetic Reso-nance Neurography Visualizes Abnormalities in Sciatic and Tibial Nerves in Patients with Type 1 Diabetes and Neuropathy. Diabetes 2017, 66, 1779–1788.
[2] Vaeggemose, M.; Pham, M.; Ringgaard, S.; Tankisi, H.; Ejskjaer, N.; Heiland, S.; Poulsen, P.L.; Andersen, H. Diffusion tensor imaging MR neurography for the detection of polyneuropathy in type 1 diabetes. J. Magn. Reson. Imaging 2016, 45, 1125–1134.
[3] Vaeggemose, M.; Haakma, W.; Pham, M.; Ringgaard, S.; Tankisi, H.; Ejskjaer, N.; Heiland, S.; Poulsen, P.; Andersen, H. Diffu-sion tensor imaging MR Neurography detects polyneuropathy in type 2 diabetes. J. Diabetes its Complicat. 2019, 34, 107439.
[4] Miyashita, A.; Kobayashi, M.; Yokota, T.; Zochodne, D.W. Diabetic Polyneuropathy: New Strategies to Target Sensory Neurons in Dorsal Root Ganglia. Int. J. Mol. Sci. 2023, 24, 5977.
[5] Wan, Q.; Wang, S.; Zhou, J.; Zou, Q.; Deng, Y.; Wang, S.; Zheng, X.; Li, X. Evaluation of radiation-induced peripheral nerve injury in rabbits with MR neurography using diffusion tensor imaging andT2measurements: Correlation with histological and functional changes. J. Magn. Reson. Imaging 2015, 43, 1492–1499.
[6] Lehmann, H.C.; Zhang, J.; Mori, S.; Sheikh, K.A. Diffusion tensor imaging to assess axonal regeneration in peripheral nerves. Exp. Neurol. 2010, 223, 238–244.
[7] Takagi, T.; Nakamura, M.; Yamada, M.; Hikishima, K.; Momoshima, S.; Fujiyoshi, K.; Shibata, S.; Okano, H.J.; Toyama, Y.; Okano, H. Visualization of peripheral nerve degeneration and regeneration: Monitoring with diffusion tensor tractography. Neuroimage 2009, 44, 884–892.
[8] Dyck, P.J.; Lais, A.; Karnes, J.L.; O’Brien, P.; Rizza, R. Fiber loss is primary and multifocal in sural nerves in diabetic polyneu-ropathy. Ann. Neurol. 1986, 19, 425–439.
[9] Neukomm, L.; Freeman, M.R. Diverse cellular and molecular modes of axon degeneration. Trends Cell Biol. 2014, 24, 515–523.
[10] Hobson-Webb LD, Walker FO. Traumatic neuroma diagnosed by ultrasonography. Arch Neurol. 2004;61(8):1322-1323.
Figures