1882
Extended Capabilities for multi-dimensional MR for Abdominal Radiation Therapy Planning1University of Southern California, Los Angeles, CA, United States, 2UT Southwestern Medical Cnter, Dallas, TX, United States, 3University of California, San Francisco, San Francisco, CA, United States, 4Cedars-Sinai Medical Center, Los Angeles, CA, United States, 5University of California, Los Angeles, Los Angeles, CA, United States
Synopsis
Keywords: Image Reconstruction, Radiotherapy
Motivation: Motion resolution of the original Multitasking 4D RTP MR sequence is not robust enough.
Goal(s): To enhance motion robustness and introduce T1/T2 mappings of 4D abdominal RTP MR protocol.
Approach: Estimation of explicit motion deformable vector fields to correct.
Results: The proposed approach dramatically enhance motion robustness of MR multitasking in 4D MRI.
Impact: The straight-forward explicit motion vector field estimation and application provides effective and robust motion correction .
Introduction
In the ever-evolving realm of medical imaging, magnetic resonance (MR) simulation has emerged as a pivotal technology in the precise planning of radiation therapy. As clinicians seek to maximize the efficacy of treatments while minimizing exposure to healthy tissues, the ability to accurately visualize and track the target area is paramount. However, the dynamic nature of the abdomen presents unique challenges for MR, notably in motion management and image co-registration across varying contrasts. Many groups, including us1-3have proposed 4D MR techniques that can resolve the respiratory motion. Our previous studies in this area introduced a multi-dimensional (volumetric, motion-resolved, multi-contrast) technique based on MR-Multitasking4 that can benefit radiation treatment planning and potentially the subsequent MR-guided radiation therapy. This abstract is to introduce our new developments that include an explicit motion model for more robust motion resolution, an additional capability to perform DCE scan at the same time and the ability to perform T1/T2 mapping. The developments expand existing capabilities that can further improve tumor and target delineation as well as open new doors for post-treatment evaluation.Method
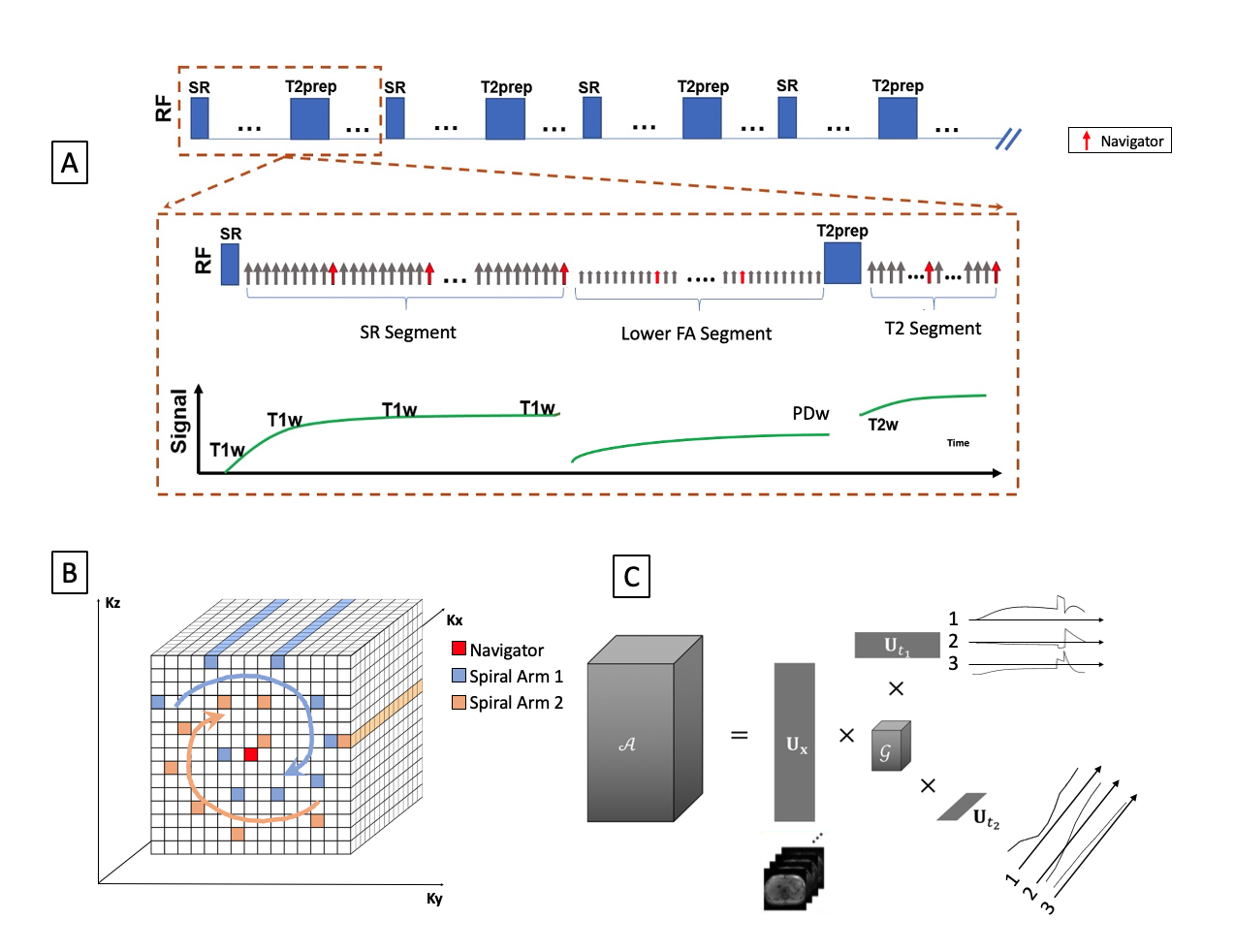
Sequence Design: As shown in Fig.1 The overall structure of our MR sequence remains unchanged from our previous works which includes a combination of GRE readouts, saturation recovery (SR) and T2-Preps. A Cartesian spiral-in sampling patterns make sures that the center of ky-kz (navigator) is sampled at a fixed interval. Image Representation: With MR-Multitasking, the multidimensional image $$$\mathcal{A}$$$ is encoded by $$\mathcal{A}=\mathbf{U}_{\mathbf{r}} \times \Phi$$With Ur being the spatial coefficient and The combined temporal factor $$$\Phi=\mathcal{G} \times_2 \mathbf{U}_{\mathrm{motion}} \times_3 \mathbf{U}_{\mathrm{contrast}}$$$ is determined from low-rank tensor completion and motion binning from the navigator data.
Explicit Motion Model:
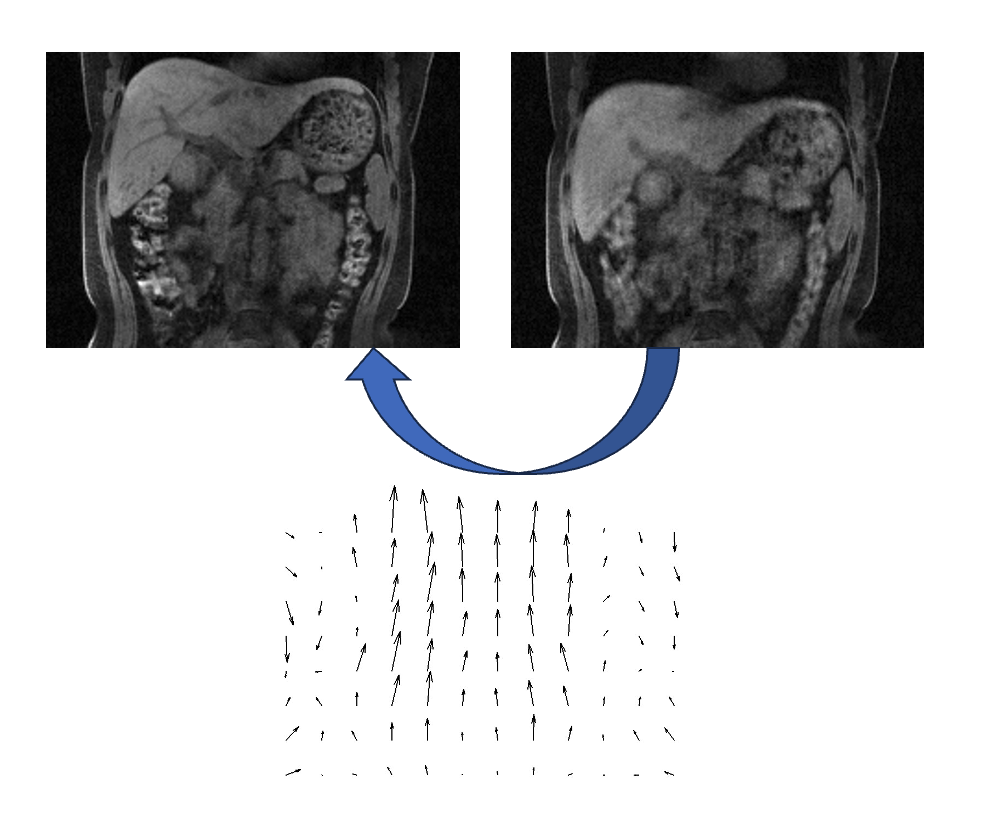
With this initial representation, the respiratory motion is encoded implicitly by values at difference indices across the motion dimension. However, explicit deformable vector fields (DVF) can be derived from final images at difference motion stages as demonstrated by figure 2. The fields can be used to directly deform an image or synthesize unacquired navigator data from acquired ones with
$$\Omega \mathbf{E} V \mathbf{U}_{\mathbf{r}} \times \Phi$$
where,$$$\Omega$$$ is the navigator sampling operator, and E is the multi-channel Fourier encoding operator.
Experiment Designs: Experiments were done on Siemens 3T and 1.5T scanners. All MR-Multitasking images were acquired with FOV = 256(SI) x 358(LR) x 256(AP) mm3, resolution = 1.6 x 1.6 x 3.2mm3 and water excitation RF pulses. Scan time are around 8 mins. Motion correction with the explicit motion model is demonstrated on healthy volunteers acquired at 3T. Contrast were injected 5 mins into the scan for those who received contrast at 3T. T1/T2 mapping capabilities were demonstrated from volunteers acquired at 1.5T with a slightly modified sequence structure where the SR pulses were replaced with T2-Inversion Recovery pulses. Additionally on 1.5T, reference 2D T1 maps with MOLLI (1.4x1.4x8.0 mm3) and 2D T2 maps with T2-prep FLASH (1.4x1.4x8.0 mm3) were acquired for comparison.
Results:
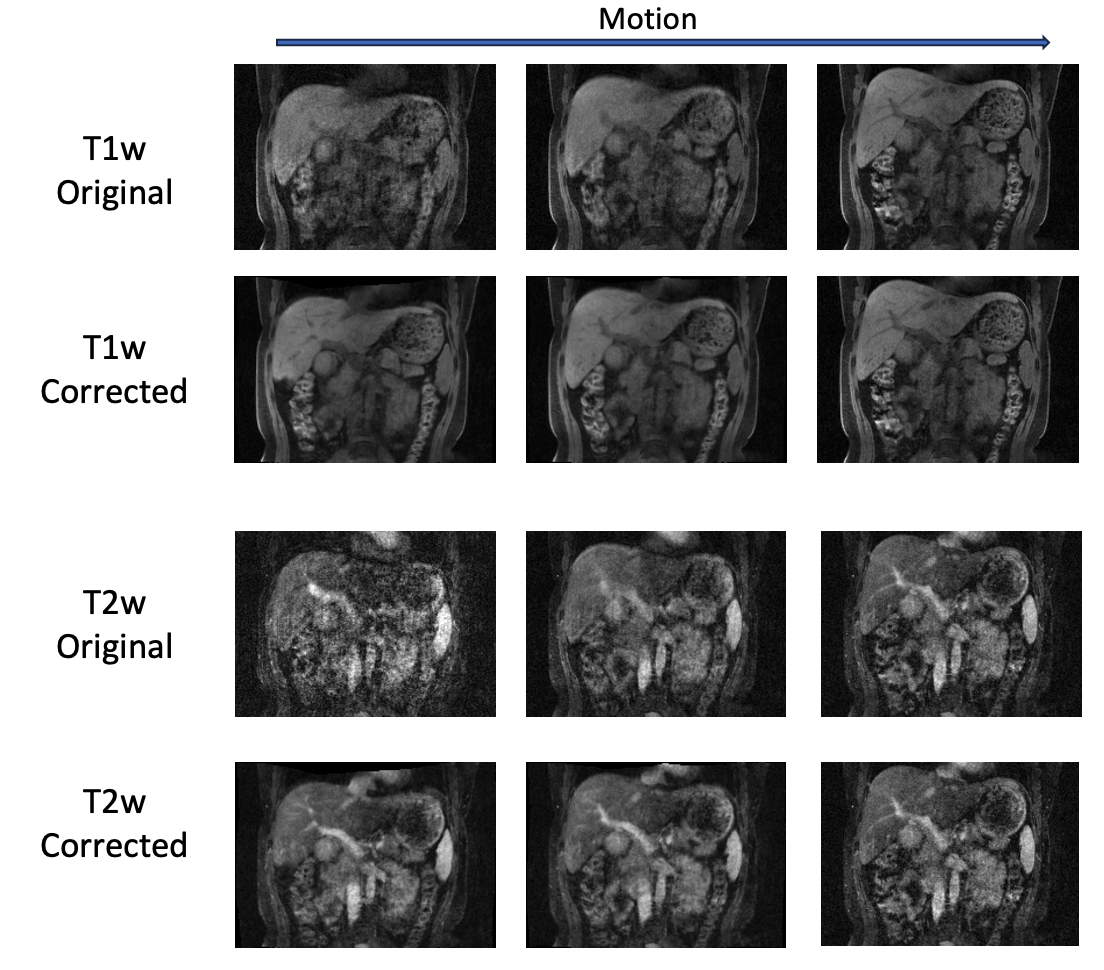
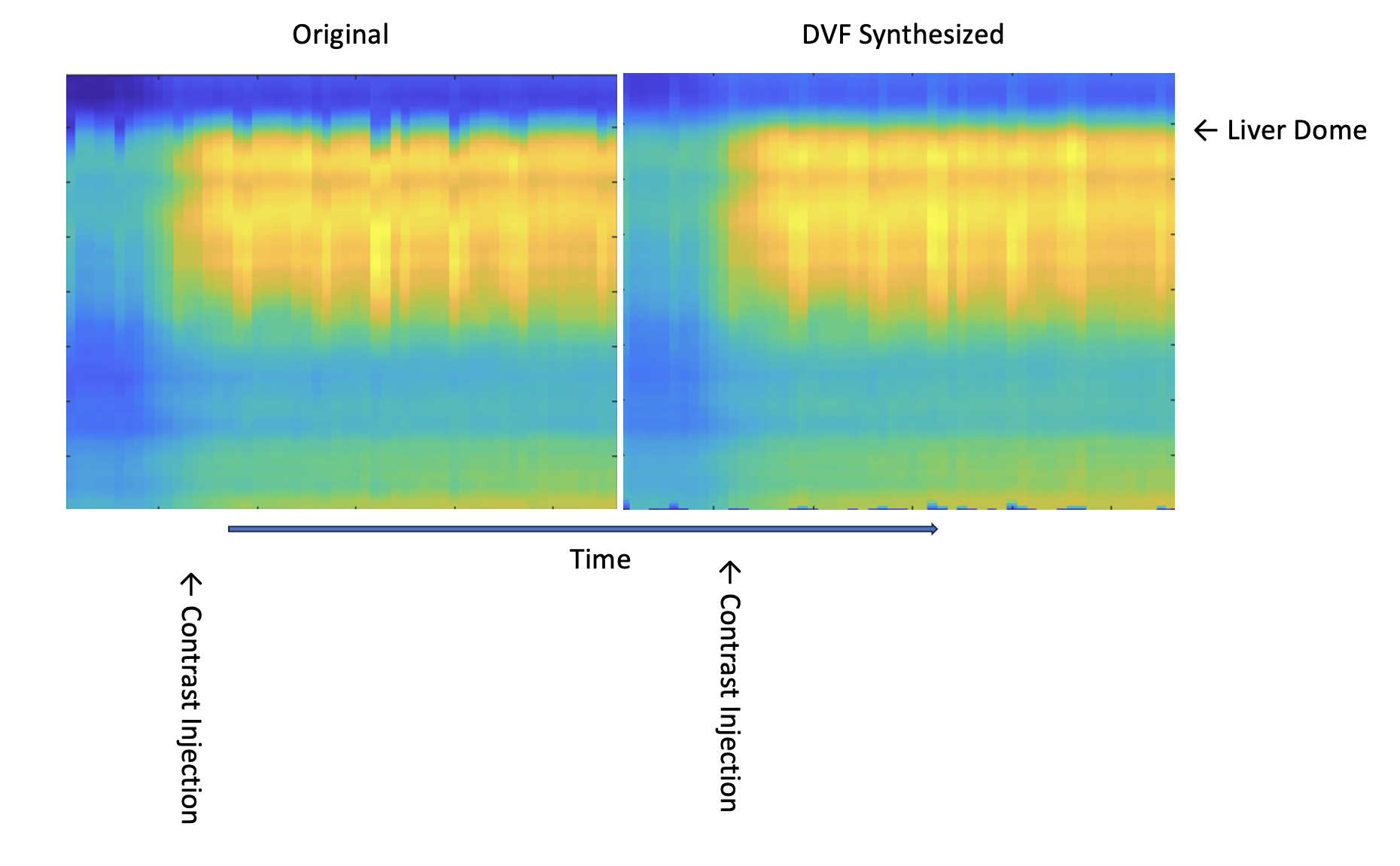
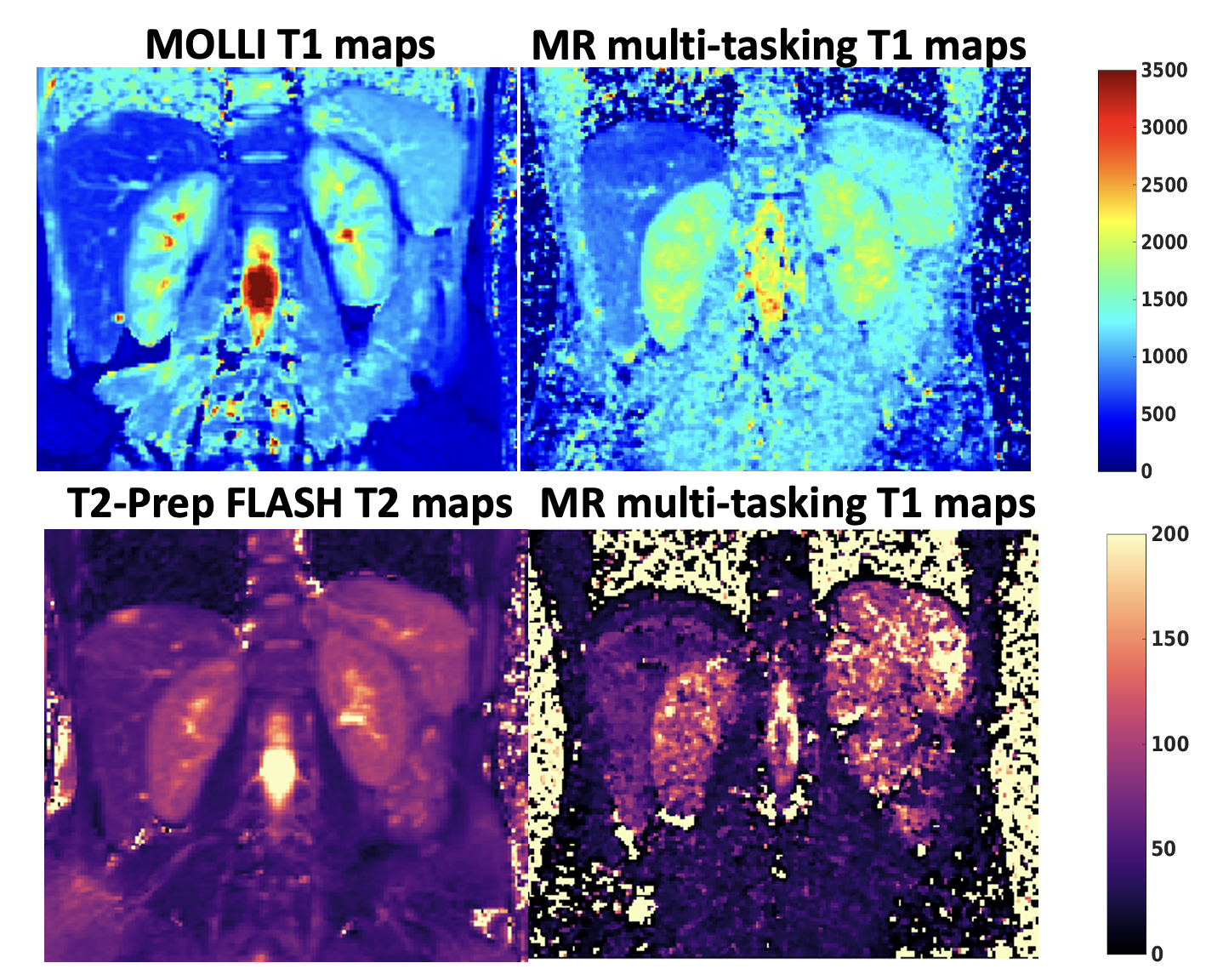
Figure 3 demonstrate the effect of using the deformable vector fields to infer different respiratory motion states for T1-w and T2-w contrasts. Motion states generated from the previous implicit model were used for comparison. Figure 4 demonstrate the DVF-synthesized navigators for across the dynamic contrast passage, the originally acquired navigators is shown for comparison. Figure 5 demonstrate the fitted T1/T2 maps from 1.5T scanners and demonstrate feasibility of using our existing framework to produce quantitative maps.Discussion
MR-Multitasking is a powerful framework to produce multidimensional images with multiple contrast and motion states. However, with the original implicit signal model, the final image may suffer from artifacts due to transient contrast dynamics (e.g. T2-prep and Gd-contrast passage) and sub-optimal motion binning. In this work, we introduced estimation of an explicit motion model with DVFs which can correct these artifacts and therefore allow for more accurate target and tumor delineation. In addition, we demonstrate the feasibility of producing multiple quantitative maps which opens the possibility for post-treatment evaluations.Conclusion
The presented MR-Multitasking technique with an explicit motion model offers a promising tool for enhancing the precision of radiation therapy planning in the abdomen. The inclusion of an explicit motion model enables a more detailed and robust characterization of respiratory motion, while the ability to perform simultaneous DCE scans and T1/T2 mapping opens new avenues for comprehensive tissue characterization. Future studies should aim to validate these techniques in a larger cohort of patients, comparing the efficacy of treatment planning and outcomes using the proposed method against traditional approaches will be essential in establishing the clinical benefits.Acknowledgements
No acknowledgement found.References
1.Huttinga NRF, Berg CAT van den, Luijten PR, Sbrizzi A. MR-MOTUS: model-based non- rigid motion estimation for MR-guided radiotherapy using a reference image and minimal k- space data. Phys Medicine Biology. 2020;65(1):015004. doi:10.1088/1361-6560/ab554a
2. Rank CM, Heußer T, Buzan MTA, et al. 4D respiratory motion-compensated image reconstruction of free-breathing radial MR data with very high undersampling. Magnet Reson Med. 2017;77(3):1170-1183. doi:10.1002/mrm.26206
3.Chen J, Han P, Han F, Hu Z, Wang N, Yang W, Ling D, Palmer S, Christodoulou A, Li D, et al. BEST IN PHYSICS (MULTI-DISCIPLINARY): Multi-Task MR (MT-MR) for Free-Breathing Simulation in Abdominal Radiotherapy Treatment Planning. In: AAPM. 2021.
4. 1.Christodoulou, A. G. et al. Magnetic resonance multitasking for motion-resolved quantitative cardiovascular imaging. Nat Biomed Eng 2, 215–226 (2018).
Figures