1871
5D reconstruction exploiting spatial-motion-echo sparsity for accelerated free-breathing liver R2*/QSM1Department of Medical Physics, Memorial Sloan Kettering Cancer Center, New York, NY, United States, 2Department of Radiology, Memorial Sloan Kettering Cancer Center, New York, NY, United States
Synopsis
Keywords: Image Reconstruction, Image Reconstruction, QSM
Motivation: Conventional compressed sensing-based 4D respiratory motion-resolved image reconstruction techniques are limited in their ability to utilize correlations between echoes for free-breathing 3D multi-echo liver MRI, which is inherently a 5D imaging problem.
Goal(s): Develop a 5D reconstruction algorithm to jointly exploit correlations between echoes and motion states.
Approach: 5D reconstruction with sparsity constraints along the motion and echo dimensions was developed to reconstruct retrospectively undersampled k-space data and compared with the 4D reconstruction on one volunteer and one patient.
Results: Compared to the 4D reconstruction, the proposed reconstruction showed comparable image quality to the reference (undersampling factor=1) and more reliable liver R2*/QSM values.
Impact: Using the proposed 5D image reconstruction, the scan time of free-breathing 3D multi-echo liver MRI for R2*/QSM can be reduced while preserving image quality and providing reliable R2*/QSM values.
Introduction
Recent advancements in free-breathing 3D multi-echo liver MRI for R2*/QSM have been achieved through the application of compressed sensing (CS)-based 4D (3D image space+1D motion state) image reconstruction1-3. However, these methods treat each individual echo independently, restricting the ability to leverage correlations between echoes. Here, we propose CS-based 5D (3D image space+1D motion state+1D echo) image reconstruction to demonstrate the feasibility of accelerated, motion-robust, and free-breathing 3D multi-echo liver MRI for R2*/QSM. The proposed reconstruction was compared with the conventional echo-by-echo 4D reconstruction method on one healthy volunteer and one patient with liver iron overload across a wide range of undersampling factors.Methods
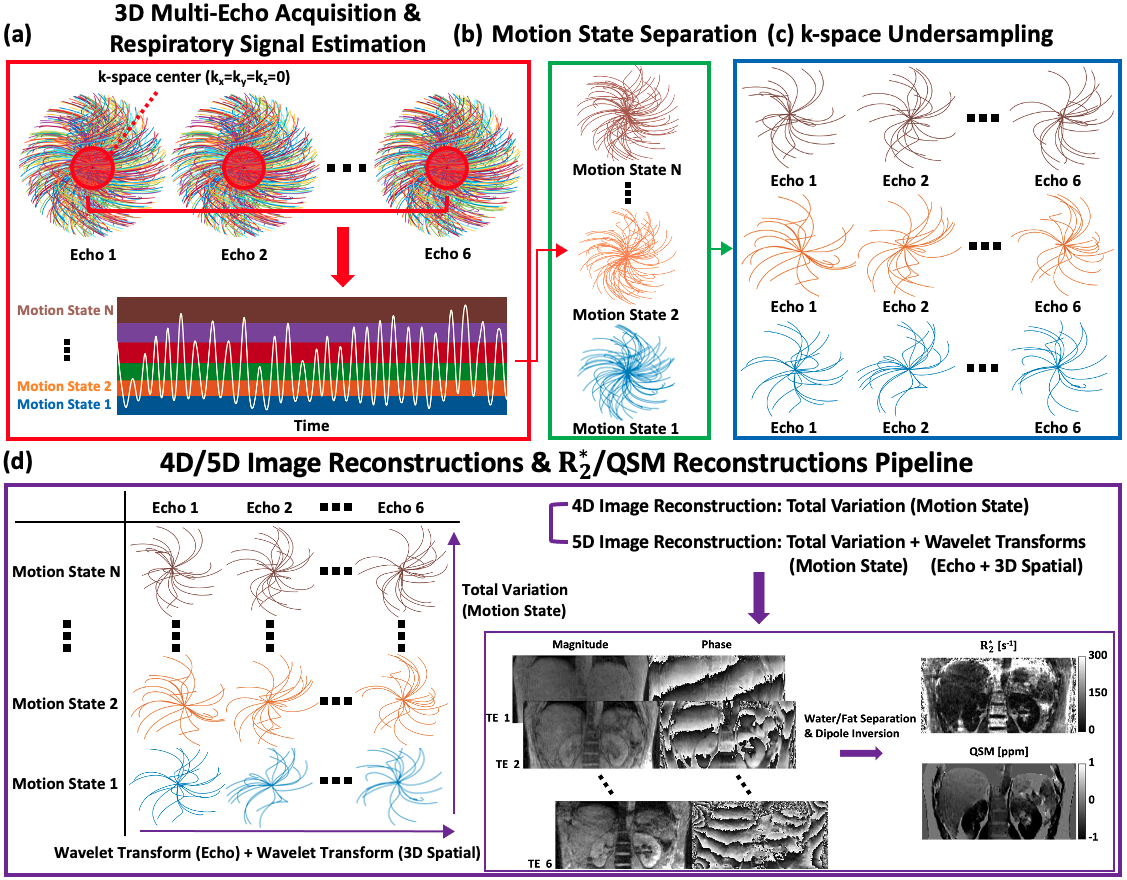
4D vs 5D image reconstructionSuppose that we have acquired 3D multi-echo liver k-space data using an incoherent k-space sampling trajectory, such as radial4 or cones1-3 under free-breathing conditions. For respiratory motion-resolved image reconstruction, information from the kz-line or the k-space center can be utilized to estimate respiratory motion. Subsequently, the k-space data can be binned into specified motion states3-5. Let M be a vectorized multi-echo image with all motion states stacked column-wise, and let Y be a vectorized multi-echo k-space raw data with all sorted motion states stacked column-wise. Then, the 4D image reconstruction solves the following problem3,5:
$$$\hat{M}=argmin_{M}\frac{1}{2}\parallel FSM-Y\parallel_D^2+\lambda_{m}TV_{m}(M),$$$
where S is the estimated coil sensitivity map using JSENSE6, F is the nonuniform fast Fourier transform (NUFFT) operator, the weighted least-squares fidelity term is associated with the density compensation factor D, and TVm is total variation along the motion state dimension.
The proposed 5D image reconstruction solves the following problem:
$$$\hat{M}=argmin_{M}\frac{1}{2}\parallel FSM-Y\parallel_D^2+\lambda_{m}TV_{m}(M)+\lambda_{e}\parallel W_{e}M\parallel_1+\lambda_{s}\parallel W_{s}M\parallel_1,$$$
where We and Ws are the wavelet transform operators along the echo and 3D image space dimensions, respectively. λm, λe, and λs are regularization parameters. The primal-dual hybrid gradient method was applied to solve both problems.
In-vivo study
With local IRB approval, one healthy volunteer and one patient with liver iron overload were scanned. All images were acquired using a 3T clinical MRI scanner (SignaPremierXT, GE Healthcare, Waukesha, WI). 3D multi-echo UTE cones acquisitions were performed following parameters: initial TE/ΔTE/TR=0.032(0.032)/1.5(1.4)/11.5(11.4)ms, #TEs=6, FA=3°, matrix size=226×(200)×226(200)×100(100), in-plane resolution=2×2mm2, slice thickness=2mm, rBW=1250 Hz/Px, and scan time= 5(5)min 56(28)s.
To perform 4D and 5D image reconstructions with retrospective undersampling, we prepared the k-space data as illustrated in Figure 1(a and b). Specifically, to enforce incoherency along the echo dimension, cone trajectories were randomly undersampled for each echo (Figure 1(c)). Using the undersampled k-space data, the 4D image reconstruction and the proposed 5D image reconstruction were separately performed. Then, R2*/QSM reconstructions were performed (Figure 1(d))3,7-10.
Results
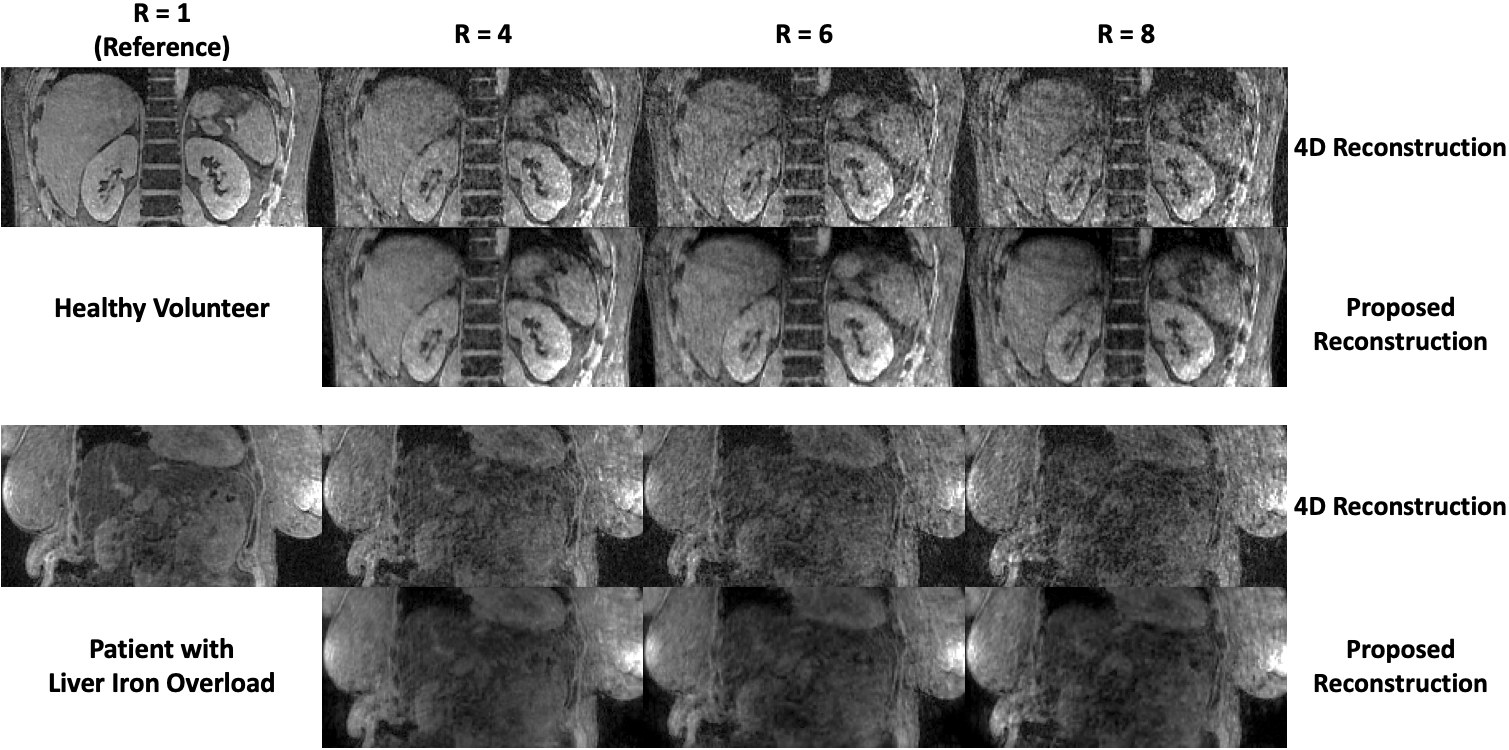
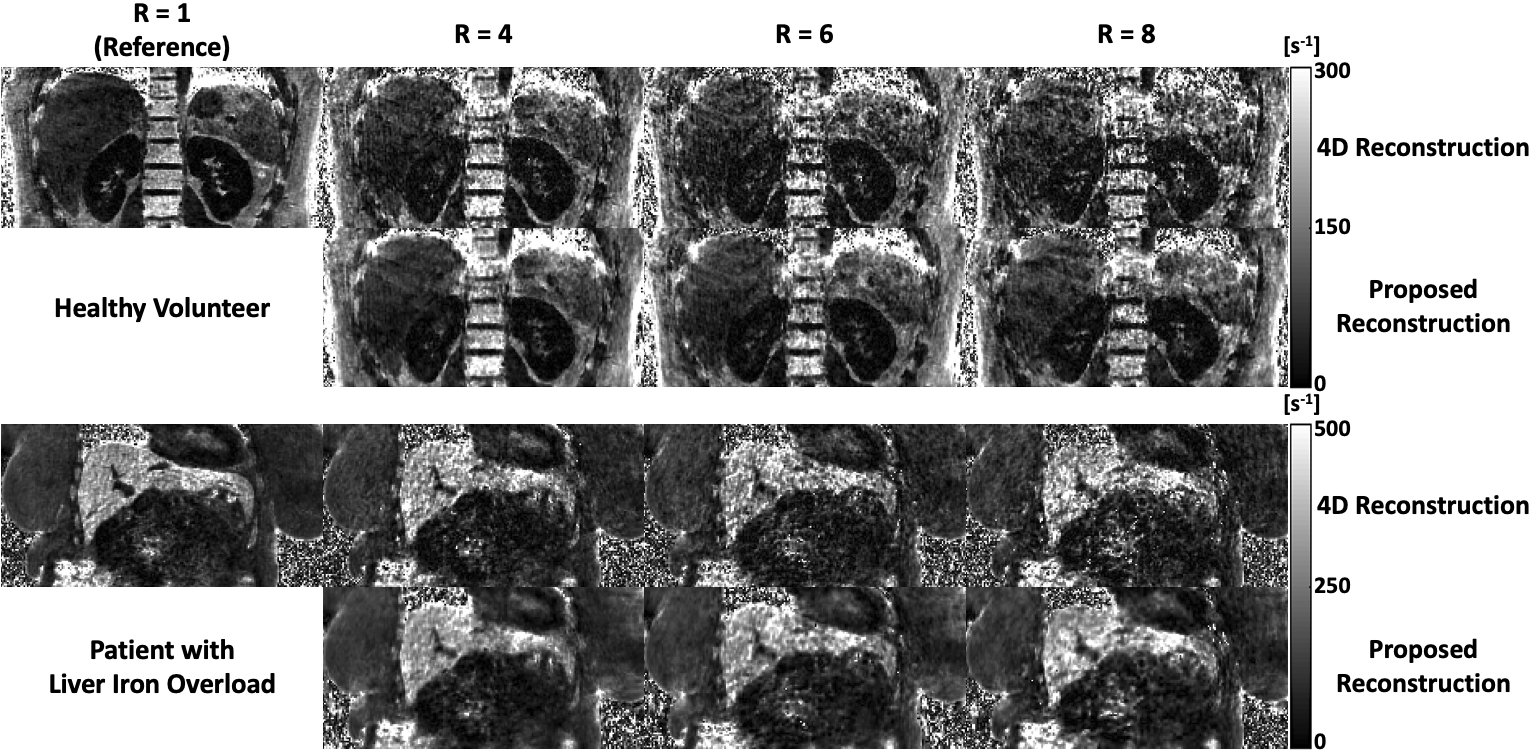
Image quality comparisonMagnitude images, R2*, and susceptibility maps from 4D and 5D image reconstructions from one healthy volunteer and one patient with liver iron overload are shown in Figures 2, 3, and 4, respectively. Across all undersampling factors, the proposed 5D image reconstruction demonstrated reduced undersampling artifacts and maintained image quality comparable to the reference (R=1 with 4D image reconstruction). Notably, the susceptibility maps in Figure 4 exhibit significant differences in image quality between the 4D and 5D image reconstructions.
Quantitative comparison
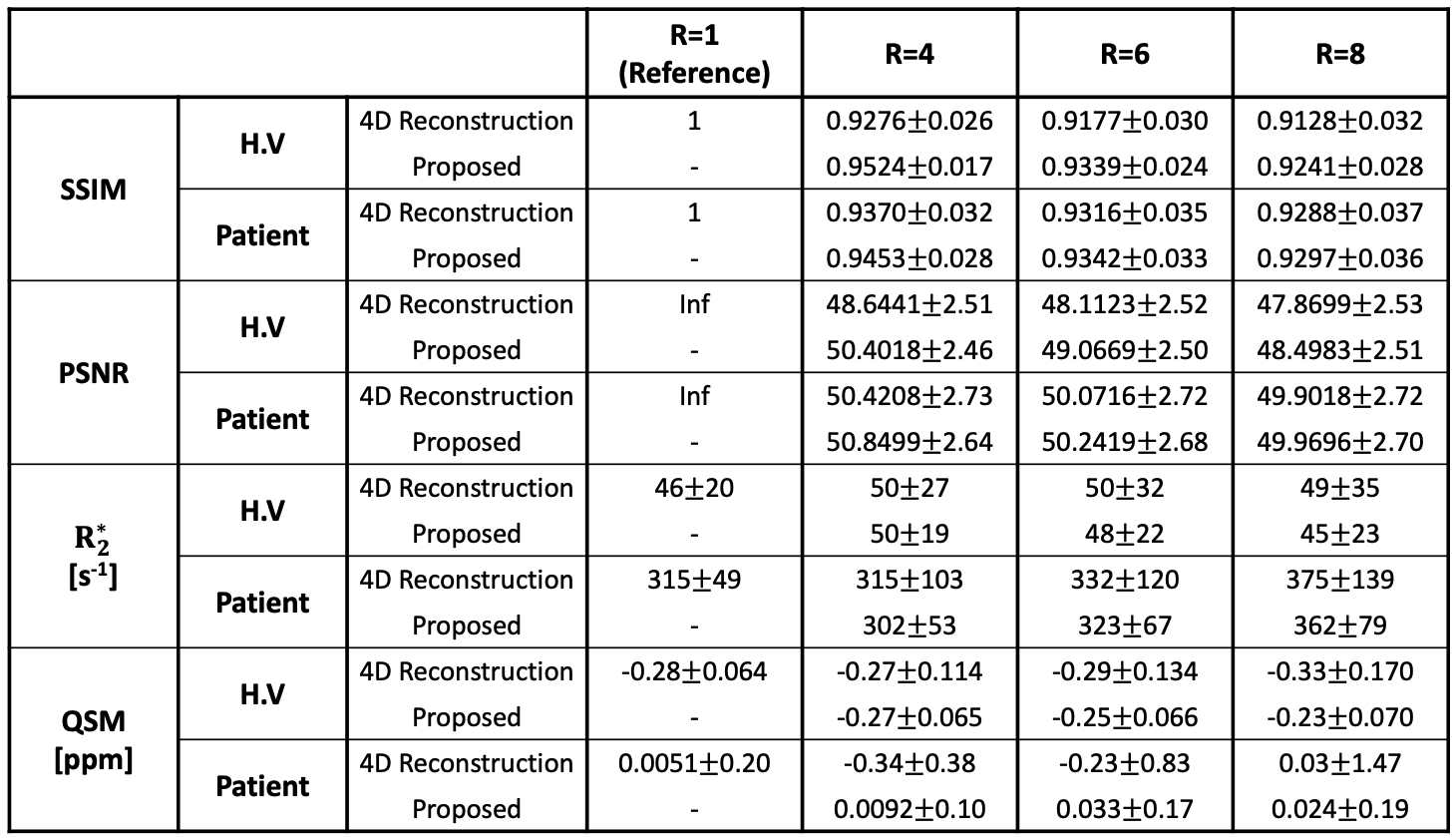
SSIM, PNSR, ROI-based mean±SD liver R2* and QSM values were evaluated as shown in Table 1. Across all undersampling factors, the proposed 5D reconstruction showed higher SSIM and PSNR values than the 4D image reconstruction in both subjects. This confirms our visual assessment of image quality. Furthermore, the 5D image reconstruction showed more consistent mean±SD liver R2* and QSM values than the 4D image reconstruction with respect to the reference, indicating an enhanced reliability in the measurements obtained from the proposed method.
Discussion
This work has demonstrated the feasibility of accelerated free-breathing liver R2*/QSM using 5D image reconstruction. The key difference between the 4D and 5D reconstruction models is that there is no coupling between echoes in the 4D model, so that the problem is separable such that each individual echo is independently updated. On the other hand, the 5D problem is inseparable so that all echoes are concurrently updated. Across all undersampling factors (R=4, 6, and 8), the proposed reconstruction exhibited comparable image quality and consistent ROI-based mean±SD liver R2*/QSM values with respect to the reference in both subjects compared to the 4D image reconstruction. Future studies will implement the proposed reconstruction on prospectively undersampled k-space datasets to explore potential reductions in scan time.Conclusion
5D reconstruction that exploits the sparsity of motion and echo improves the performance of 4D reconstruction that exploits only motion sparsity for accelerated free-breathing liver R2*/QSM.Acknowledgements
This work was supported by the NIH/NIBIB under Award Number R21EB033985.References
[1] Kang, M., Jafari, R., Behr, G. G., Otazo, R., & Kee, Y. Free-breathing liver QSM with high isotropic resolution using respiratory motion-resolved 3D multi-echo cones MRI. In Proceedings of the 2022 ISMRM & ISMRT Annual Meeting, London.
[2] Kang, M., Behr, G. G., Glezerman I. G., Otazo, R., & Kee, Y. Free-breathing renal R2*/QSM using 3D multi-echo UTE cones acquisition and respiratory motion-resolved image reconstruction with image-based self-navigator. In Proceedings of the 2023 ISMRM & ISMRT Annual Meeting, Toronto.
[3] Kang, M., Behr, G. G., Jafari, R., Gambarin, M., Otazo, R., & Kee, Y. (2023). Free‐breathing high isotropic resolution quantitative susceptibility mapping (QSM) of liver using 3D multi‐echo UTE cones acquisition and respiratory motion‐resolved image reconstruction. Magnetic Resonance in Medicine, 90(5), 1844-1858.
[4] Armstrong, T., Zhong, X., Shih, S. F., Felker, E., Lu, D. S., Dale, B. M., & Wu, H. H. (2022). Free-breathing 3D stack-of-radial MRI quantification of liver fat and R2* in adults with fatty liver disease. Magnetic Resonance Imaging, 85, 141-152.
[5] Feng, L., Axel, L., Chandarana, H., Block, K. T., Sodickson, D. K., & Otazo, R. (2016). XD‐GRASP: golden‐angle radial MRI with reconstruction of extra motion‐state dimensions using compressed sensing. Magnetic resonance in medicine, 75(2), 775-788.
[6] Ying, L., & Sheng, J. (2007). Joint image reconstruction and sensitivity estimation in SENSE (JSENSE). Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine, 57(6), 1196-1202.
[7] Yu, H., McKenzie, C. A., Shimakawa, A., Vu, A. T., Brau, A. C., Beatty, P. J., ... & Reeder, S. B. (2007). Multiecho reconstruction for simultaneous water‐fat decomposition and T2* estimation. Journal of Magnetic Resonance Imaging: An Official Journal of the International Society for Magnetic Resonance in Medicine, 26(4), 1153-1161.
[8] Dong, J., Liu, T., Chen, F., Zhou, D., Dimov, A., Raj, A., ... & Wang, Y. (2014). Simultaneous phase unwrapping and removal of chemical shift (SPURS) using graph cuts: application in quantitative susceptibility mapping. IEEE transactions on medical imaging, 34(2), 531-540.
[9] Liu, Z., Spincemaille, P., Yao, Y., Zhang, Y., & Wang, Y. (2018). MEDI+ 0: Morphology enabled dipole inversion with automatic uniform cerebrospinal fluid zero reference for quantitative susceptibility mapping. Magnetic resonance in medicine, 79(5), 2795-2803.
[10] Liu, J., Liu, T., de Rochefort, L., Ledoux, J., Khalidov, I., Chen, W., ... & Wang, Y. (2012). Morphology enabled dipole inversion for quantitative susceptibility mapping using structural consistency between the magnitude image and the susceptibility map. Neuroimage, 59(3), 2560-2568.
Figures