1870
Improved Reconstruction Speed for 5D Free Running Motion Resolved Using a Variable Projection Augmented Lagrangian (VPAL) Method1Biomedical Engineering, Georgia Institute of Technology and Emory University, Atlanta, GA, United States, 2Mathematics, Emory University, Atlanta, GA, United States, 3Radiology and Imaging Science, Emory University School of Medicine, Atlanta, GA, United States, 4Radiology, Lausanne University Hospital (CHUV)), Lausanne, Switzerland, 5Advanced Clinical Imaging Technology, Siemens Healthineers International AG, Lausanne, Switzerland
Synopsis
Keywords: Image Reconstruction, Image Reconstruction
Motivation: 5D free-running whole heart CMR offers CT-quality images but requires hours-long reconstruction time, preventing clinical usage. Therefore, a more efficient reconstruction algorithm is needed.
Goal(s): We propose to use the advanced numerical algorithm to reduce the reconstruction time while preserving image quality.
Approach: A variable projection augmented Lagrangian (VPAL) method for 5D motion-resolved image reconstruction was developed and compared with the state-of-the-art alternating direction method of multipliers (ADMM) on 15 5D free-running raw data sets.
Results: When compared to the ADMM method, VPAL reduced the reconstruction time by 60%, preserved image similarity, had equivalent ejection fraction measurements, and had superior radiologist ratings.
Impact: This study shows that using an advanced numerical algorithm for highly under-sampled MR reconstruction both reduces computational time and results in better image quality for diagnostics, bringing 5D free-running imaging closer to clinical usage.
Background
5D free-running CMR imaging is a free-breathing CMR method that produces high spatial (1mm3) and temporal resolution (50ms) images by utilizing an image-based self-navigation signal for retrospective cardiac and respiratory gating [1]. 5D free-running CMR uses compressed sensing-based reconstruction to recover the underlying image data from highly under-sampled k-space in the cardiac and respiratory dimensions. However, using the state-of-the-art alternating direction method of multipliers (ADMM) [2], the iterative reconstruction method still requires several hours on a multi-GPU cluster, which is not viable for clinical usage. Therefore, we need an efficient method to improve the speed for 5D free-running CMR reconstruction. We propose to use an efficient numerical algorithm, called the variable projection augmented Lagrangian (VPAL) method which was shown to converge faster with less computational cost [3]. We hypothesize that the VPAL method is less computationally expensive and thus reconstructs faster than the ADMM method and preserves the image quality for functional analysis and diagnostics.Method
This study utilized data from a prototype ungated 5D free-running whole-heart CMR images acquired in 15 pediatric patients infused with ferumoxytol (4mg/kg). Cardiac and respiratory motions are extracted from the raw k-space data of the 5D free-running acquisition and were used to retrospectively bin the raw data into a set of four respiratory and a variable number of cardiac positions with a temporal resolution of 50ms [1]. The objective function of the reconstruction consists of a data consistency term, an L1- regularized spatial finite difference, and L2- regularized temporal finite differences in the cardiac and respiratory direction,$$$f(x,z)=\frac{1}{2} \|\|Ax-b\|\|_2^2+λ_1 \|\|z\|\|_1+\frac{λ_2}{2} \|\|D_t x\|\|_2^2+\frac{λ_3}{2} \|\|D_r x\|\|_2^2+\frac{ρ}{2} \|\|D_s x-z+u\|\|_2^2$$$ Here, A contains the non-uniform Fourier transform operator and coil sensitivity operator, $$$x$$$ is the target 5D image, variable $$$z$$$ computes the finite difference of the image in the spatial dimension. $$$D_t$$$ and $$$D_r$$$ are the finite difference operators in the cardiac and respiratory dimensions respectively, and $$$u$$$ is the augmented scaled Lagrange multiplier. The ADMM reference reconstruction algorithm has 10 outer and 4 inner CG iterations for the quadratic part of the problem. Our proposed VPAL approach allows reducing the computational cost for the quadratic problem using a single variable projection step per iteration, such that $$$x_{k+1}=x_k - α_k \cdot g_{x_k}$$$ where $$$g_{x_k}$$$ is the gradient of $$$x_k$$$ at f(x,z) and $$$α_k$$$ is a minimizer of $$$f(x_k-α_k \cdot g_{x_k},z_k)$$$ with a closed form solution as $$$α_k=\frac{g_k^T g_k}{(Ag_k )^T (Ag_k )+λ_2 (D_t g_k )^T (D_t g_k )+λ_3 (D_r g_k )^T (D_r g_k )+ρ(D_s g_k )^T (D_s g_k ) }$$$. The following parameters: $$$λ_1 = 0.0001$$$, $$$λ_2=λ_3=0.5$$$ and $$$ρ = 0.06$$$ were empirically determined and used for both reconstructions. Both ADMM and VPAL were implemented in MATLAB. The reconstruction time, structural similarity index measure (SSIM), and ejection fraction (EF%) of the reconstructed 5D images of the VPAL method were compared with the reference ADMM reconstruction. Additionally, radiologist ratings of ADMM and VPAL were done; images were ordered randomly for a blind review from an experienced CMR radiologist with the following 0-4 scoring criteria: 4 is excellent diagnostic value and 0 is non-diagnostic. The student-paired t-test with alpha = 0.95 is used for significance testing.Results
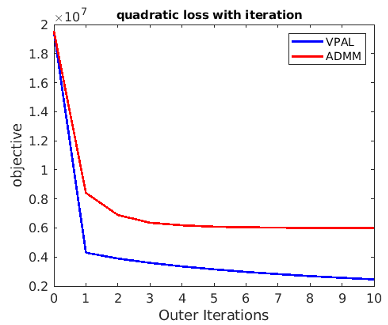
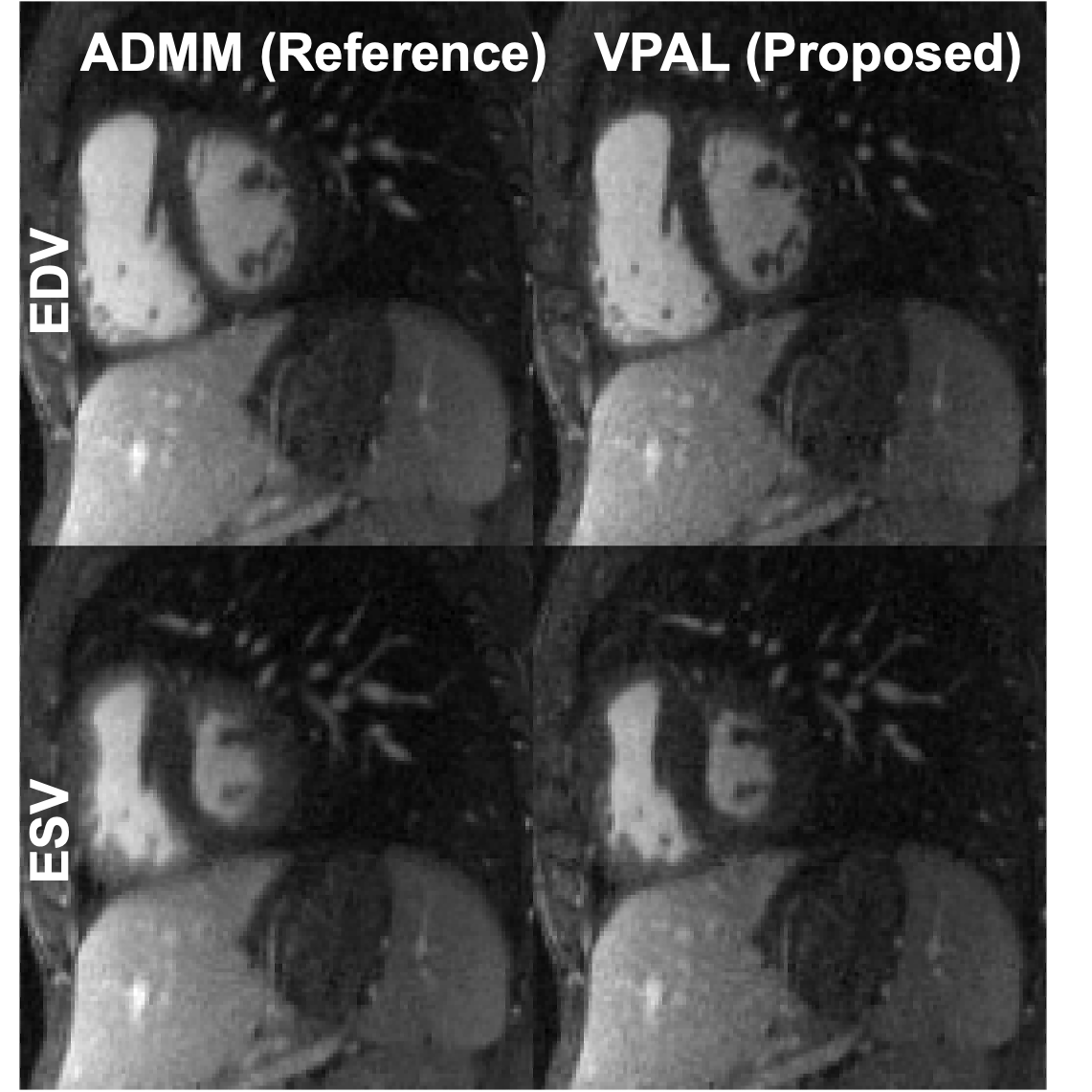
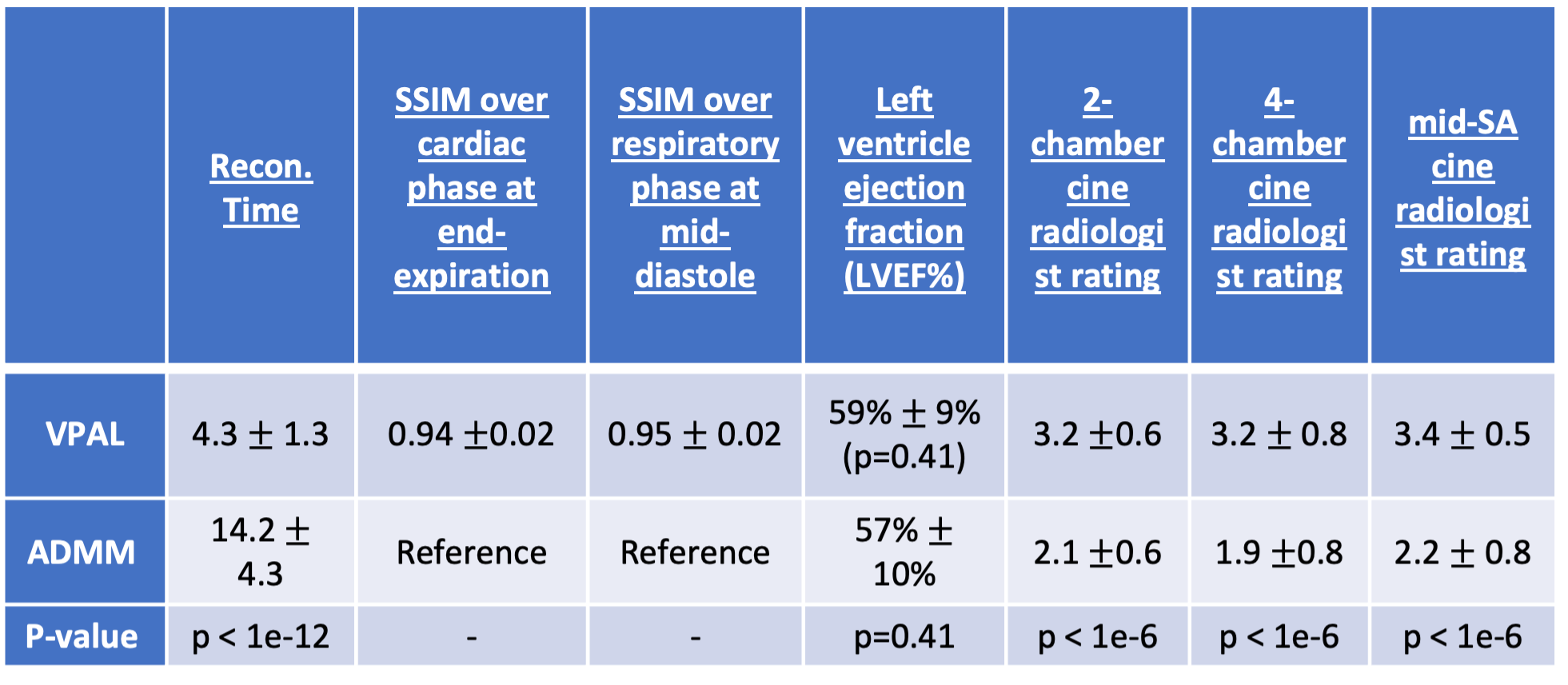
Reconstruction time, structural similarity, LVEF, and radiologist rating are summarized in Table 1. Using 10 outer iterations, VPAL converges faster than ADMM (Fig 1), and uses 60% less time to reconstruct the 5D motion-resolved images compared to ADMM method. Example reformatted mid-short-axis views of the heart at end-diastole and end-systole are shown the proposed VPAL method and the reference ADMM in Fig. 2. VPAL reconstructed images appear to be sharper than ADMM reconstructed images with high structural similarity across cardiac and respiratory phases and higher radiologist ratings, indicating higher diagnostic value. No significant difference was found between the left ventricular ejection fraction measured using VPAL and ADMM images.Discussion
This study demonstrates the efficiency of the variable projection method to reconstruct 5D motion-resolved images compared to the ADMM method. Using the same number of outer iterations, a single variable projection step in VPAL reduces the reconstruction time from 14.2±4.3 hours to 4.3±1.3 hours and achieves greater diagnostic quality 3D whole-heart motion resolved images possibly due to the sharper appearance of VPAL images versus ADMM images. Further development of the VPAL algorithm within the computer architecture will further the rate-limiting steps affecting reconstruction time and enable the adoption of the 5D free-running framework in the clinical domain.Conclusion
VPAL is a more time-efficient numerical algorithm to recover the highly under-sampled data in each retrospectively gated cardiac and respiratory position while preserving the quality of the reconstruction and potentially improving image quality.Acknowledgements
No acknowledgement found.References
[1] Di Sopra, L, Piccini, D, Coppo, S, Stuber, M, Yerly, J. An automated approach to fully self-gated free-running cardiac and respiratory motion-resolved 5D whole-heart MRI. Magn Reson Med. 2019; 82: 2118–2132. https://doi.org/10.1002/mrm.27898
[2] Stephen Boyd; Neal Parikh; Eric Chu; Borja Peleato; Jonathan Eckstein, Distributed Optimization and Statistical Learning via the Alternating Direction Method of Multipliers, 2011.
[3] Chung M, Renaut RA. A variable projection method for large-scale inverse problems with ℓ1 regularization. Appl Numer Math. 2023;192:297-318. doi:10.1016/j.apnum.2023.06.015
Figures