1833
Detection of Elevated Succinate in Brain During Circulatory Arrest: A 3T 1H MR Spectroscopy Study1Radiology, Stanford University, Stanford, CA, United States
Synopsis
Keywords: Spectroscopy, Spectroscopy, Succinate
Motivation: To measure succinate in brain during circulatory arrest in a piglet model of cardiac bypass.
Goal(s): Dynamic measurement of succinate using 3T MR spectroscopy
Approach: Spectral fits of the archived data were used to create dynamic plots of succinate, to provide statistics, and to generate simulated spectra for validation.
Results: Elevation of succinate during circulatory arrest was observed and validated. Fitting bias was evaluated over the linewidths and signal-to-noise S/Ns of the archived data. Succinate increase did not appear to be dependent on bypass temperature. Succinate elevation was not observed with antegrade cerebral perfusion.
Impact: Elevated succinate during ischemia has been identified as a source of ischemic-reperfusion injury. The ability to measure increased succinate during ischemia plus the ability to intercede with succinate inhibitors may have important consequence prior to re-perfusion in bypass and stroke.
Introduction
Elevated succinate during ischemia has been identified as a source of ischemic-reperfusion IR injury1-7. IR injury occurs when the tissue blood supply is disrupted and then restored. While reperfusion is essential for survival, it also initiates oxidative damage, cell death and aberrant immune responses through the generation of mitochondrial reactive oxygen species8. In this study, we examine MR spectra of brain collected during cardiac bypass CBP using a piglet model, to determine if succinate elevation can be observed and if any change depends on key CBP surgical parameters such as hypothermic temperature and cerebral blood flow.Methods
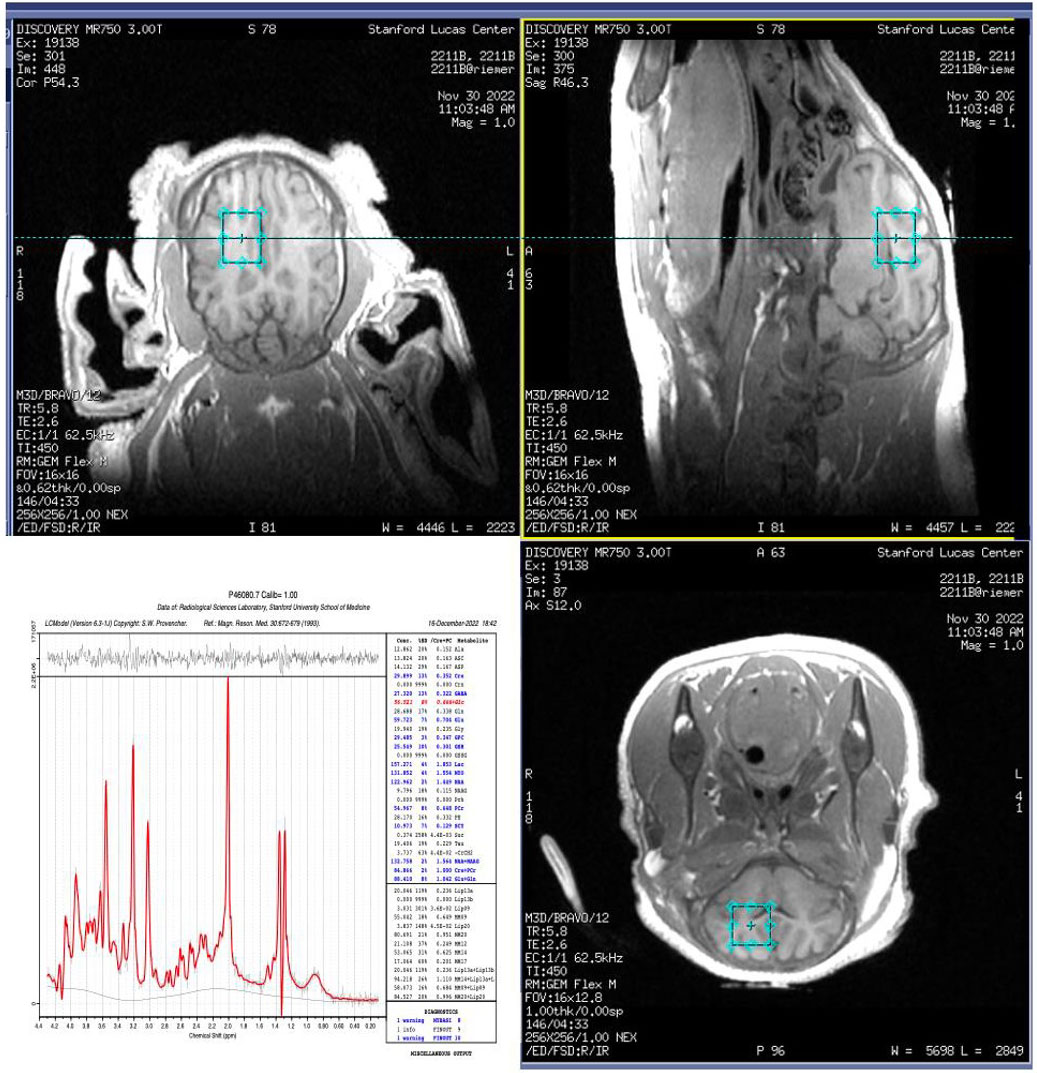
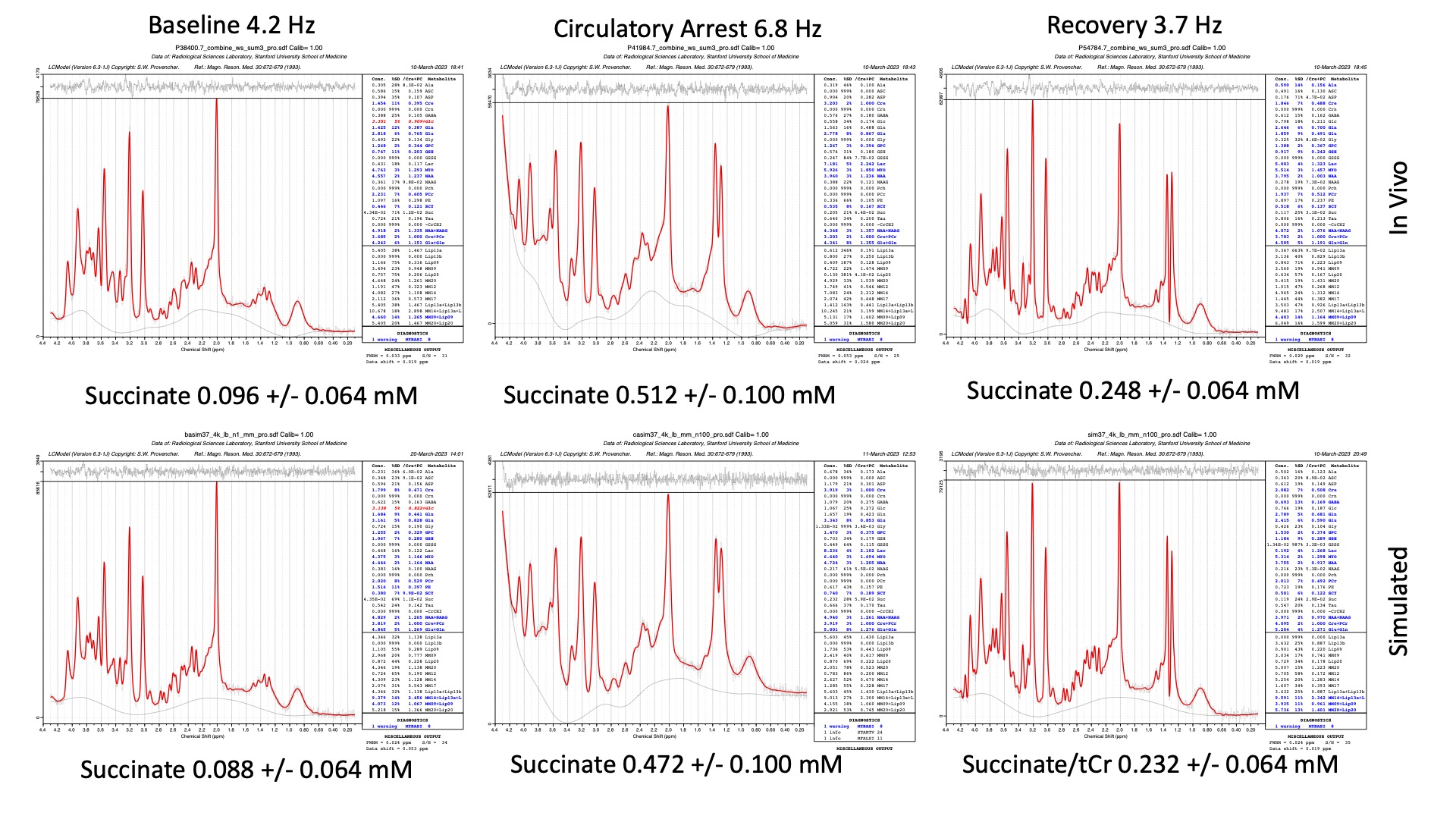
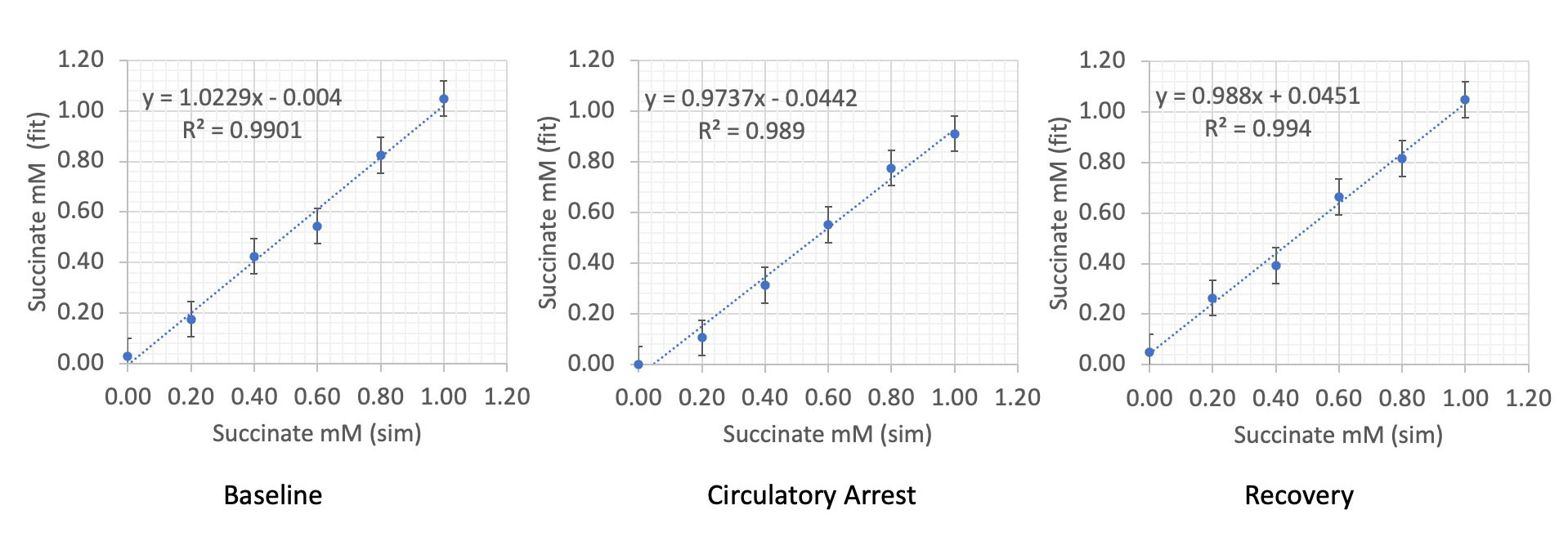
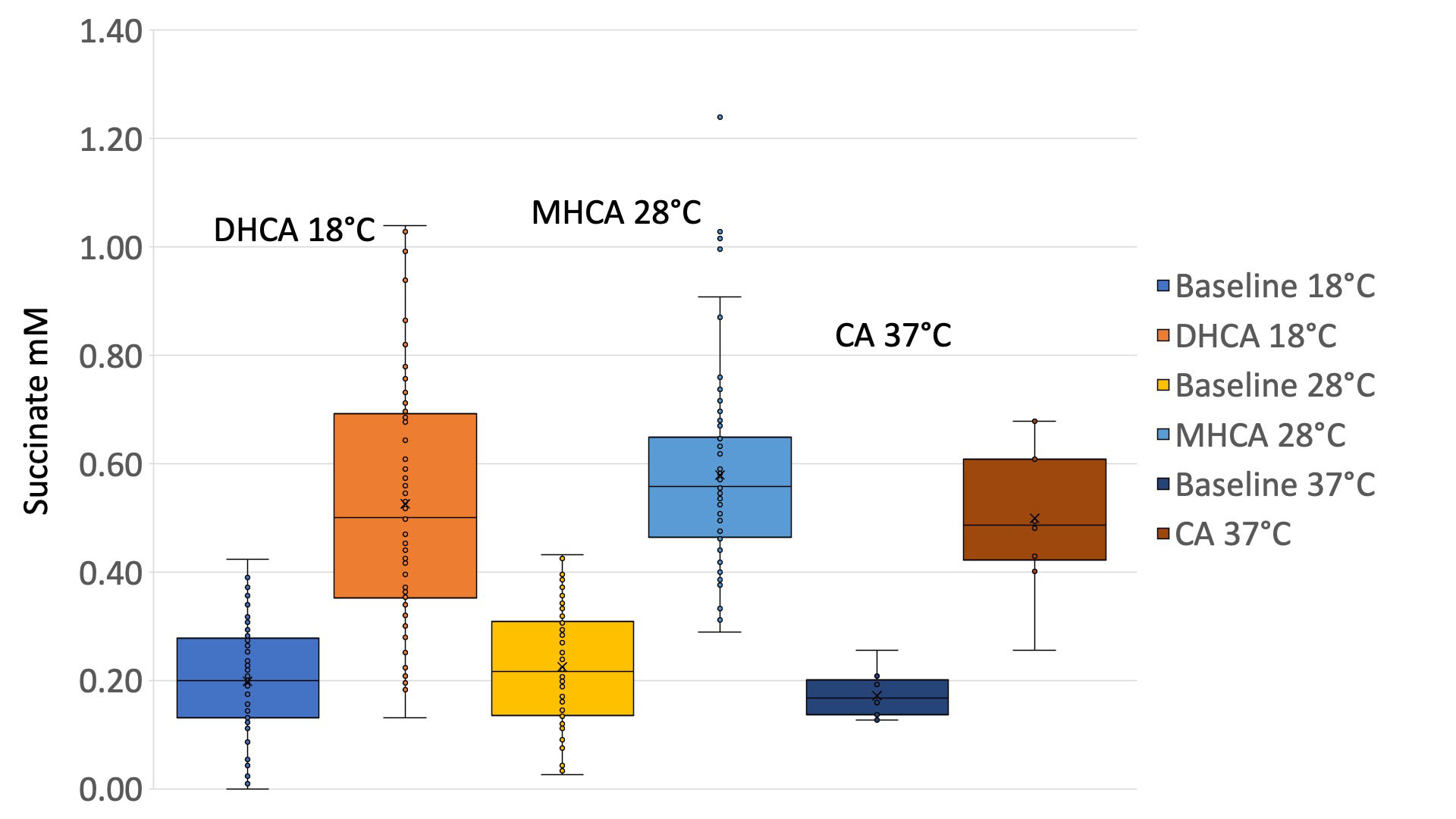
Data were taken from an archive of 23 in-magnet bypass studies. Animal prep and sLASER 2000/30 spectra (WIP GE Healthcare, Waukesha, WI) from a 12 x 12 x 15 mm3 voxel placed in the right midbrain is as previously described9,10. LCModel (version 6.3-1J)11 fits collected during baseline, circulatory arrest CA and recovery intervals are plotted versus time relative to the start of CA. Standard deviations of metabolites are taken from the LCModel estimation of %SD, and a 2-point running average was applied. Data were converted to mM, assuming an average total creatine concentration of 8 mM over the full experiment. To validate the LCModel estimates of succinate, simulated spectra with a known metabolite ground truth were constructed, adding line shape, macromolecules, baseline, and noise to match in vivo results. In vivo line shape, baseline and macromolecule contributions vary significantly with temperature, circulatory arrest, and recovery conditions. Circulatory arrest spectral-baseline can be dominated by increasing levels of deoxy-Hemoglobin deoxyHb which produces a powder pattern from the water in and near vasculature12,13. Succinate concentration was adjusted to provide a titration from 0.00 to 1.00 mM in 0.2 mM steps. Estimates of the succinate in each in vivo spectrum during CBP-baseline and during CA intervals were recorded and sorted by bypass temperature (18°C, 28°C and 37°C) and presented as a box-and-whisker plots.Results
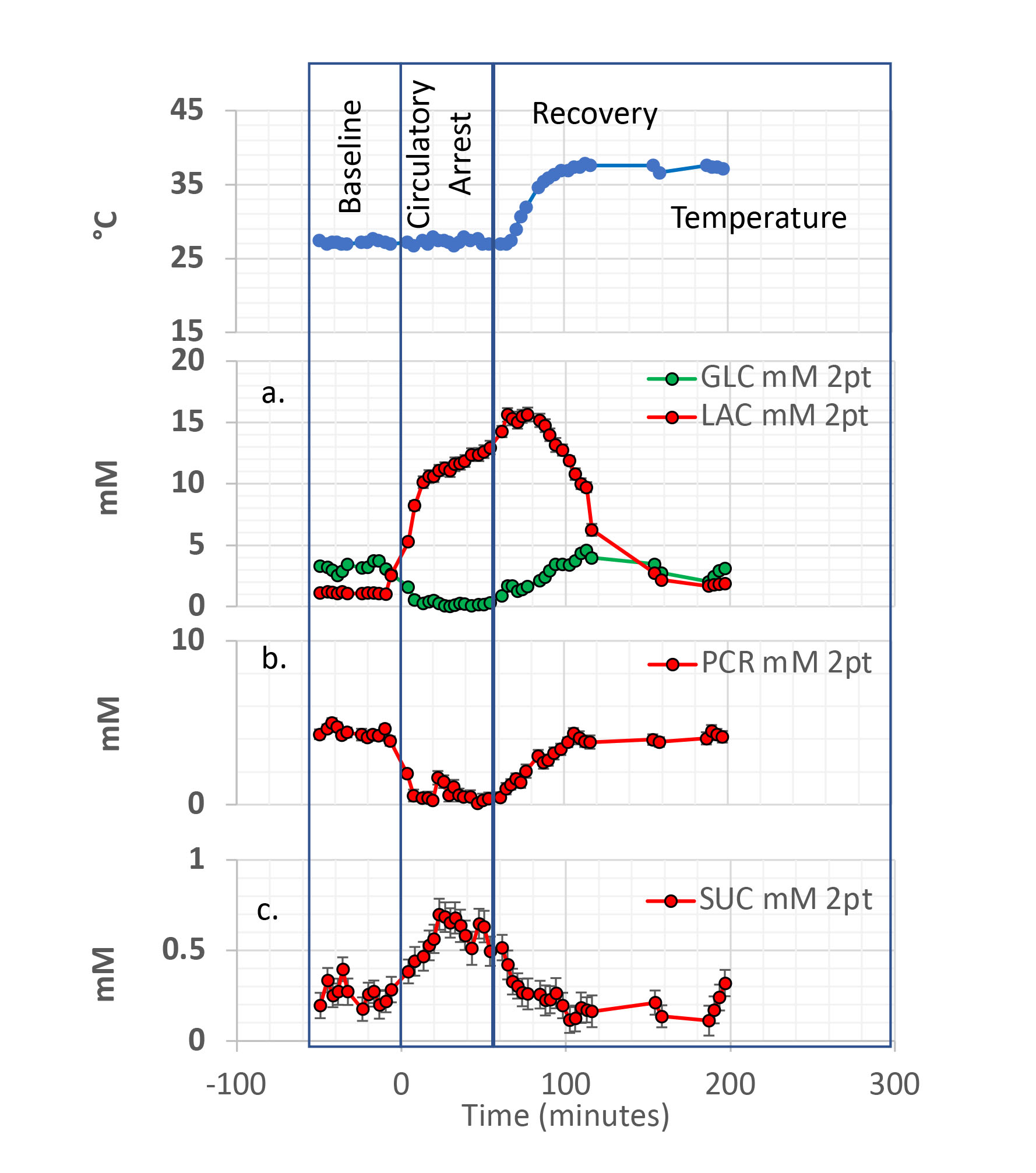
Figure 1 illustrates prescription, and Figure 2 shows dynamics of brain temperature, glucose GLC, lactate LAC, phosphocreatine PCR, and succinate SUC during a 28°C mild hypothermic circulatory arrest MHCA run. The decrease in GLC and the buildup and plateau of LAC during CA along with the depletion and recovery of PCR are observed at mM levels are as expected. Baseline succinate at around 0.2 mM is just detectable at the temporal resolution of the study but appears to rise during CA to over 0.6 mM and then recover back to near baseline on reperfusion. Figure 3 shows LCModel fits for in vivo and simulated data at baseline, circulatory arrest, and recovery periods in a 37°C bypass study. At S/N of >30 fits match the simulated input for all metabolites with minimal bias. Linewidths and S/N derived from the LCModel fits are indicated and the simulated spectra match the in vivo spectra well. Cramer-Rao-lower-bounds CRLB of 0.064 mM was observed for baseline and recovery intervals, increasing to 0.100 mM for the broader spectra in the CA interval. Figure 4 shows titration of succinate from 0.0 to 1.0 mM for baseline, circulatory arrest, and recovery. Figure 5 shows a box and whisker plot comparing succinate increase during CA (without antegrade cerebral perfusion ACP) at 3 temperatures relative to baseline conditions. No evidence of temperature dependence was observed.Discussion
Detection of elevated brain succinate during CBP circulatory arrest using 3T MR spectroscopy is clearly demonstrated. As expected, no elevation of succinate was detected in the ACP studies where the brain is selectively perfused during the CA intervals. Sub mM changes with CRLBs as high as 0.140 mM in individual spectra are overcome by the large number of spectra acquired. Overlap of signal along with the possibility of bias, makes validation of results from partially obscured signals like succinate an absolute requirement. High succinate observed in this study, is still below mM level, and the 4-proton singlet at 2.4 ppm is overlapped in the GLU+GLN GLX spectral region. Dynamic data, statistics using the overall archive of CBP results, simulations with titration of the metabolite in question, and difference spectra are all support the LCModel SUC estimations. Elevated succinate in CBP circulatory arrest might be targeted as suggested for stroke. The apparent lack of temperature dependence of succinate elevation in our study is interesting and consistent with a previous cardiac study in which protection against cardiac IR injury by hypothermia and by inhibition of succinate accumulation was found to be additive14.Acknowledgements
NIH P41EB015891, R01MH110683 HL152757References
1. Mottahedin A, Prag HA, Dannhorn A, et al. Targeting succinate metabolism to decrease brain injury upon mechanical thrombectomy treatment of ischemic stroke. Redox Biol 2023;59:102600.
2. Mizuma A, You JS, Yenari MA. Targeting Reperfusion Injury in the Age of Mechanical Thrombectomy. Stroke 2018;49:1796-802.
3. Tretter L, Patocs A, Chinopoulos C. Succinate, an intermediate in metabolism, signal transduction, ROS, hypoxia, and tumorigenesis. Biochim Biophys Acta 2016;1857:1086-101.
4. Kamarauskaite J, Baniene R, Trumbeckas D, Strazdauskas A, Trumbeckaite S. Increased Succinate Accumulation Induces ROS Generation in In Vivo Ischemia/Reperfusion-Affected Rat Kidney Mitochondria. Biomed Res Int 2020;2020:8855585.
5. Tannahill GM, Curtis AM, Adamik J, et al. Succinate is an inflammatory signal that induces IL-1beta through HIF-1alpha. Nature 2013;496:238-42.
6. Chouchani ET, Pell VR, Gaude E, et al. Ischaemic accumulation of succinate controls reperfusion injury through mitochondrial ROS. Nature 2014;515:431-5.
7. Sahni PV, Zhang J, Sosunov S, et al. Krebs cycle metabolites and preferential succinate oxidation following neonatal hypoxic-ischemic brain injury in mice. Pediatr Res 2018;83:491-7.
8. Eltzschig HK, Eckle T. Ischemia and reperfusion--from mechanism to translation. Nat Med 2011;17:1391-401.
9. Hanley FL, Ito H, Gu M, Hurd R, Riemer RK, Spielman D. Comparison of dynamic brain metabolism during antegrade cerebral perfusion versus deep hypothermic circulatory arrest using proton magnetic resonance spectroscopy. J Thorac Cardiovasc Surg 2020;160:e225-e7.
10. Spielman DM, Gu M, Hurd RE, Riemer RK, Okamura K, Hanley FL. Proton magnetic resonance spectroscopy assessment of neonatal brain metabolism during cardiopulmonary bypass surgery. NMR Biomed 2022;35:e4752.
11. Provencher SW. Automatic quantitation of localized in vivo 1H spectra with LCModel. NMR Biomed 2001;14:260-4.
12. Springer CS, Patlack, C.S., Palyka, I, and Huang W. Principles of Susceptibility Contrast-Based Functional MRI: The Sign of the Functional MRI Response. In: Moonen CTW, and Bandettini, P.A, ed. Functional MRI. Berlin: Springer-Verlag; 1999:91-102.
13. Wilson GJ, Springer CS, Jr., Bastawrous S, Maki JH. Human whole blood (1) H2 O transverse relaxation with gadolinium-based contrast reagents: Magnetic susceptibility and transmembrane water exchange. Magn Reson Med 2017;77:2015-27.
14. Kohlhauer M, Pell VR, Burger N, et al. Protection against cardiac ischemia-reperfusion injury by hypothermia and by inhibition of succinate accumulation and oxidation is additive. Basic Res Cardiol 2019;114:18.
Figures