1827
Investigating Cortical Neurochemical Concentrations in Painful Knee Osteoarthritis using Magnetic Resonance Spectroscopy1Department of Biomedical Engineering, Schulich School of Engineering, University of Calgary, Calgary, AB, Canada, 2McCaig Institute for Bone and Joint Health, Cumming School of Medicine, University of Calgary, Calgary, AB, Canada, 3Department of Radiology, Cumming School of Medicine, University of Calgary, Calgary, AB, Canada, 4Hotchkiss Brain Institute, Cumming School of Medicine, University of Calgary, Calgary, AB, Canada, 5Alberta Children’s Hospital Research Institute, University of Calgary, Calgary, AB, Canada, 6Section of Orthopaedic Surgery, Cumming School of Medicine, University of Calgary, Calgary, AB, Canada
Synopsis
Keywords: Spectroscopy, Osteoarthritis, Chronic Pain
Motivation: Alterations in the brain are suggested to contribute to chronic arthritis pain, however there is limited research on the specific neurochemicals and brain regions involved in this process.
Goal(s): We aimed to identify neurochemicals and brain regions associated with chronic pain in knee osteoarthritis to understand the brain’s contribution to this condition.
Approach: We used magnetic resonance spectroscopy to compare neurochemical levels in four pain-related brain regions between cohorts of patients with painful knee osteoarthritis and healthy controls.
Results: Significantly lower levels of GABA and myoinositol in the anterior cingulate cortex in the knee osteoarthritis group suggests potential disrupted inhibitory processes and neuroinflammation.
Impact: Patients with painful knee osteoarthritis exhibited significantly lower levels of GABA and myoinositol in the anterior cingulate cortex compared to healthy controls. These findings illuminate the anterior cingulate cortex as a potential therapeutic target for knee osteoarthritis pain management.
Introduction
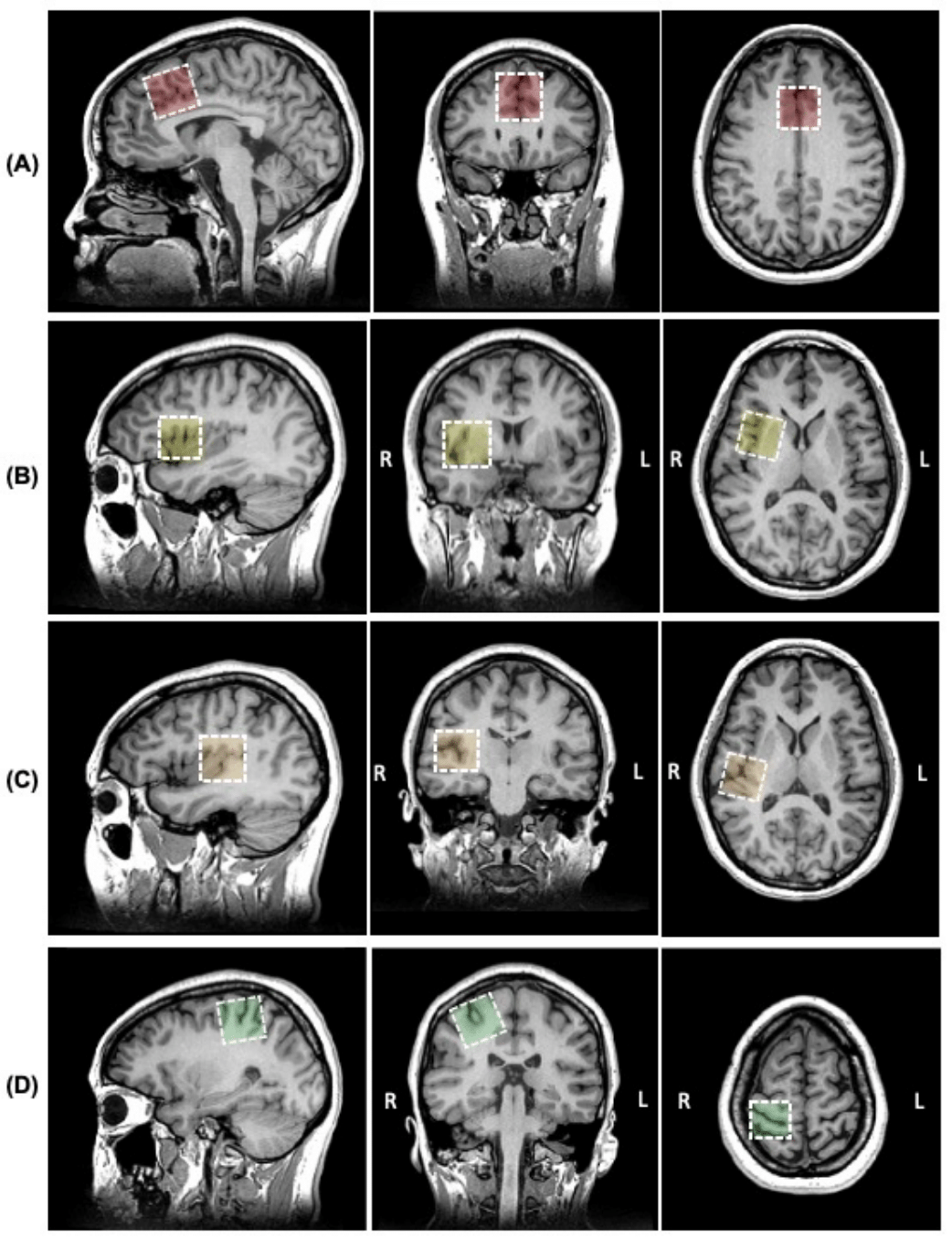
Knee osteoarthritis, a degenerative joint disease, is the most common cause of chronic pain worldwide.1 Structural knee damage (i.e., tissue damage shown on x-ray) is poorly associated with pain severity.3–5 Emerging evidence suggests that alterations within the brain may contribute to this dissociation between structural knee damage and pain severity.2 Magnetic resonance spectroscopy (MRS) offers a non-invasive means to investigate neurochemical alterations within pain-related brain regions, providing valuable insights into the brain’s contribution to pain perception. Specifically, understanding neurochemical alterations associated with knee osteoarthritis-induced pain holds potential in identifying therapeutic targets for improved pain management in osteoarthritis.Thus, this cross-sectional study compared levels of six neurochemicals of interest in four brain regions between cohorts of patients with painful knee osteoarthritis and healthy controls. The neurochemicals of interest were gamma-aminobutyric acid (GABA), glutamate + glutamine (Glx), myoinositol, total creatine, total choline, and total N-acetylaspartate. These neurochemicals play key roles in inhibition, excitation, neurotransmission, and cellular functioning. Examining their concentrations in brain regions associated with pain; the anterior cingulate cortex, anterior insula, posterior insula, and the somatosensory cortex, may offer information about how the body processes and responds to pain signals.
Methods
This study was reviewed by the local ethics board and all participants provided informed consent. 20 female participants with end-stage knee osteoarthritis (i.e., scheduled for total knee replacement surgery) were recruited along with 19 healthy controls (40-75y). Participants underwent brain MRS at 3T to quantify GABA, Glx, myoinositol, total creatine, total choline, and total N-acetylaspartate levels in four key pain-processing regions of the brain – the anterior cingulate cortex, the anterior and posterior insular cortices, and the somatosensory cortex (Figure 1).Data were collected on a 3T GE 750W scanner. A T1-weighted structural image was acquired for voxel placement and tissue segmentation. GABA data were collected using macromolecule-suppressed GABA-edited MEGA-PRESS (TR/TE=1800ms/80ms, 20ms editing pulses at 1.5ppm and 1.9ppm, 30x30x30mm3 voxels, 256 averages) and analyzed using the Gannet 3.2 toolbox6 in MATLAB. Glx, myoinositol, total creatine, total choline, and total N-acetylaspartate data were acquired using short-echo single voxel PRESS (TR/TE= 1800ms/30ms, 30x30x30mm3 voxels, 64 averages). PRESS data were preprocessed in FID-A7, quantified in LCModel8, and subsequently tissue corrected9. Data were excluded if visual inspection indicated substantial movement artifacts, the signal-to-noise (SNR) ratio was less than 25, the full width at half maximum (FWHM) was greater than 0.07ppm, and/or the fit error (CRLB) was greater than 20%. Because the data was non-normally distributed, neurochemical concentration levels were compared between patients and controls using Mann Whitney U tests.
Results
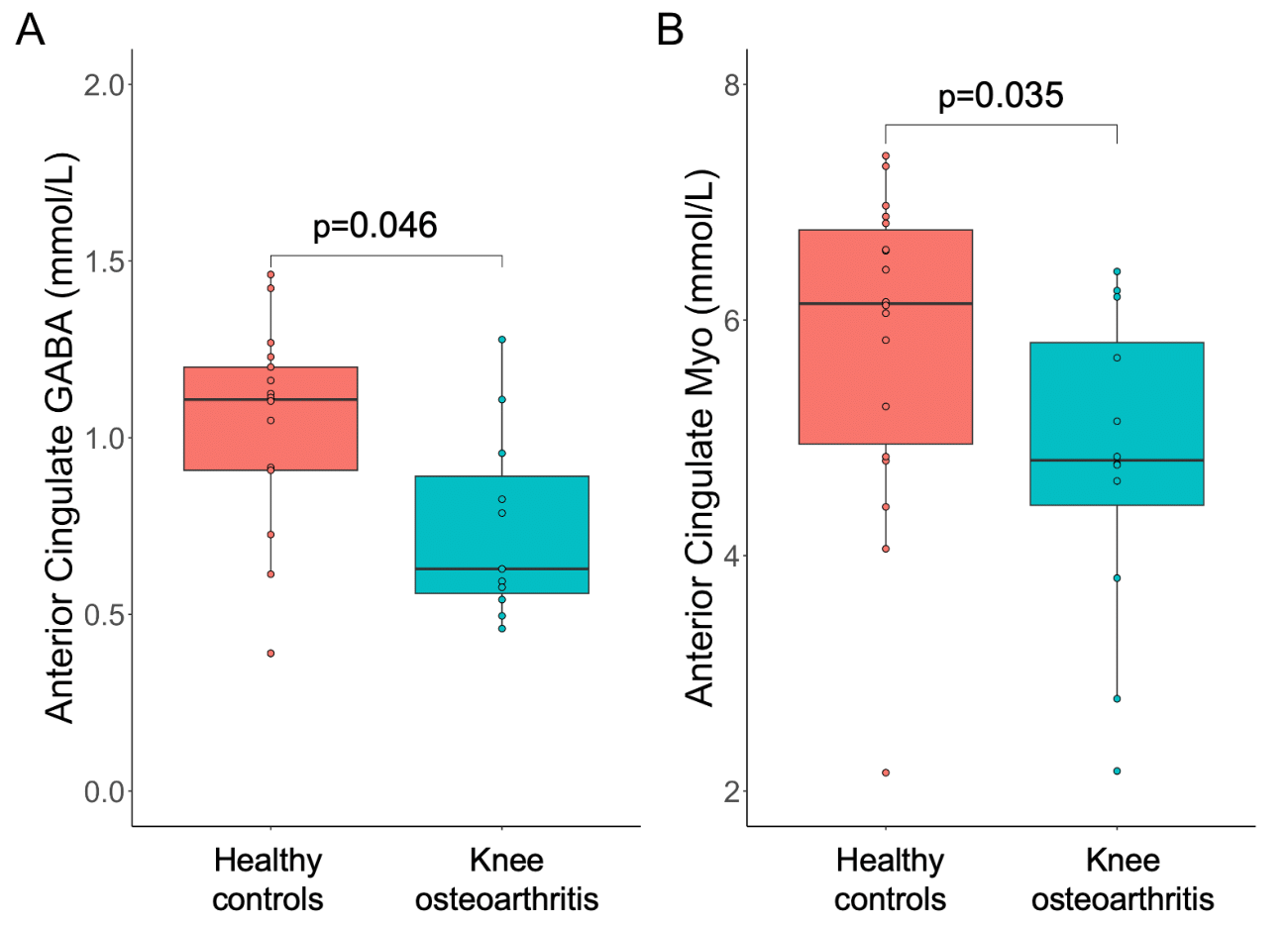
We found significantly lower levels of GABA (p=0.046) and Myo (p=0.035) in the anterior cingulate cortex in knee osteoarthritis patients compared to controls (Figure 2). There were no significant differences in Glx, total creatine, total choline, or total N-acetylaspartate concentrations between knee osteoarthritis patients and controls in any of the 4 regions of interest (all p>0.05).Discussion & Conclusion
Significantly lower levels of GABA and myoinositol were observed in the anterior cingulate cortex of patients with knee osteoarthritis. As GABA is a primary inhibitory neurotransmitter in the central nervous system, reduced concentrations may indicate altered inhibitory processes within the anterior cingulate cortex, potentially contributing to the heightened pain perception observed in individuals with knee osteoarthritis. This finding aligns with previous studies implicating GABAergic dysfunction in chronic pain conditions, emphasizing the importance of anterior cingulate cortex GABAergic modulation in the context of osteoarthritic pain.10 Myoinositol is a marker of glial cell activity, as well as being involved in cell signaling and membrane stability. Changes in myoinositol concentrations could be indicative of neuroinflammatory processes or disruptions in cellular regulation within the anterior cingulate cortex, both of which have been implicated in chronic pain states.11,12 Thus, this study suggests potential associations between the brain, particularly the anterior cingulate cortex, and the experience of pain in knee osteoarthritis. This may motivate further research to investigate the anterior cingulate cortex as a therapeutic target for pain management in knee osteoarthritis.Acknowledgements
This study was supported by the University of Calgary; the Hotchkiss Brain Institute, University of Calgary; the Arthritis Society Canada (PhD Salary Award 22-0000000127 to SAL and Stars Career Development Award STAR-18-0189 to SLM); the Canada Research Chair to ADH in MR Spectroscopy in Brain Injury; and the Natural Sciences Council of Canada (CGS-D to SAL).References
1. Neogi, T. The epidemiology and impact of pain in osteoarthritis. Osteoarthr. Cartil. 21, 1145–53 (2013).
2. Clauw, D. J. & Hassett, A. L. The role of centralised pain in osteoarthritis. Clin. Exp. Rheumatol. 35, S79–S84 (2017).
3. Cooper, C. et al. Risk factors for the incidence and progression of radiographic knee osteoarthritis. Arthritism & Rhreumatism 43, 995–1000 (2000).
4. Dieppe, P. A., Cushnaghan, J. & Shepstone, L. Progression of osteoarthritis (OA) over 3 years and the relationship between clinical and radiographic changes at the knee joint. Osteoarthr. Cartil. 5, 87–97 (1997).
5. Hannan, M. T., Felson, D. T. & Pincus, T. Analysis of the discordance between radiographic changes and knee pain in osteoarthritis of the knee. J. Rheumatol. 27, 1513–7 (2000).
6. Harris, A. D., Puts, N. A. J. & Edden, R. A. E. Tissue correction for GABA-edited MRS: Considerations of voxel composition, tissue segmentation, and tissue relaxations. J. Magn. Reson. Imaging 42, 1431–1440 (2015).
7. Simpson, R., Devenyi, G. A., Jezzard, P., Hennessy, T. J. & Near, J. Advanced processing and simulation of MRS data using the FID appliance (FID-A)—An open source, MATLAB-based toolkit. Magn. Reson. Med. 77, 23–33 (2017).
8. Provencher, S. W. Automatic quantitation of localized in vivo 1H spectra with LCModel. NMR Biomed. 14, 260–264 (2001).
9. Near, J. et al. Preprocessing, analysis and quantification in single‐voxel magnetic resonance spectroscopy: experts’ consensus recommendations. NMR Biomed. 34, 1–23 (2021).
10. Peek, A. L. et al. Brain GABA and glutamate levels across pain conditions: A systematic literature review and meta-analysis of 1H-MRS studies using the MRS-Q quality assessment tool. Neuroimage 210, 116532 (2020).
11. Jung, C. et al. Magnetic resonance imaging of neuroinflammation in chronic pain: a role for astrogliosis? Pain 161, 1555–1564 (2020).
12. Widerström-Noga, E. et al. Metabolite concentrations in the anterior cingulate cortex predict high neuropathic pain impact after spinal cord injury. Pain 154, 204–212 (2013).
Figures