1819
Evaluation of Local Microstructural Gradients in the Myocardium of Subjects with Severe Aortic Stenosis.1Cardiovascular Research Center, Mass General Hospital, Boston, MA, United States, 2A.A Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Charlestown, MA, United States, 3Institute of Medical Physics and Radiation Protection, TH Mittelhessen University of Applied Sciences, Geissen, Germany, 4Cardiovascular Innovation Research Center, Heart, Vascular, and Thoracic Institute, Cleveland Clinic, Cleveland, OH, United States, 5Health Sciences and Technology Program, Harvard - Massachusetts Institute of Technology, Cambridge, MA, United States
Synopsis
Keywords: Myocardium, Radiomics
Motivation: Diffusion tensor imaging of the heart can be performed with sub-mm resolution. However, established metrics do not fully take advantage of this improved resolution.
Goal(s): We aimed to determine whether local gradients in helix angle (HA) could be calculated and used to characterize the microstructural response of the heart to the load imposed by aortic stenosis.
Approach: Voxel-wise maps of radial, circumferential, minimum and maximum HA gradients were generated.
Results: The radial HA gradient was reduced in aortic stenosis, but microstructural coherence was well preserved in these patients despite a marked increase in the thickness of the myocardium.
Impact: DTI of the heart with sub-mm in-plane resolution allows maps of local HA gradients to be generated, providing novel insights into the microstructure of the heart.
Introduction
Diffusion tensor MRI (DTI) allows the microstructural properties of the myocardium to be measured non-invasively, but its resolution, typically 2.5x2.5mm in-plane, is limited. We recently presented an approach to perform DTI of the heart with submillimeter (0.85x0.85mm) in-plane resolution 1,2. Here, we leverage this enhanced resolution to measure local microstructural gradients in the myocardium in subjects with severe aortic stenosis (AS) and age-matched controls (CTL).Methods
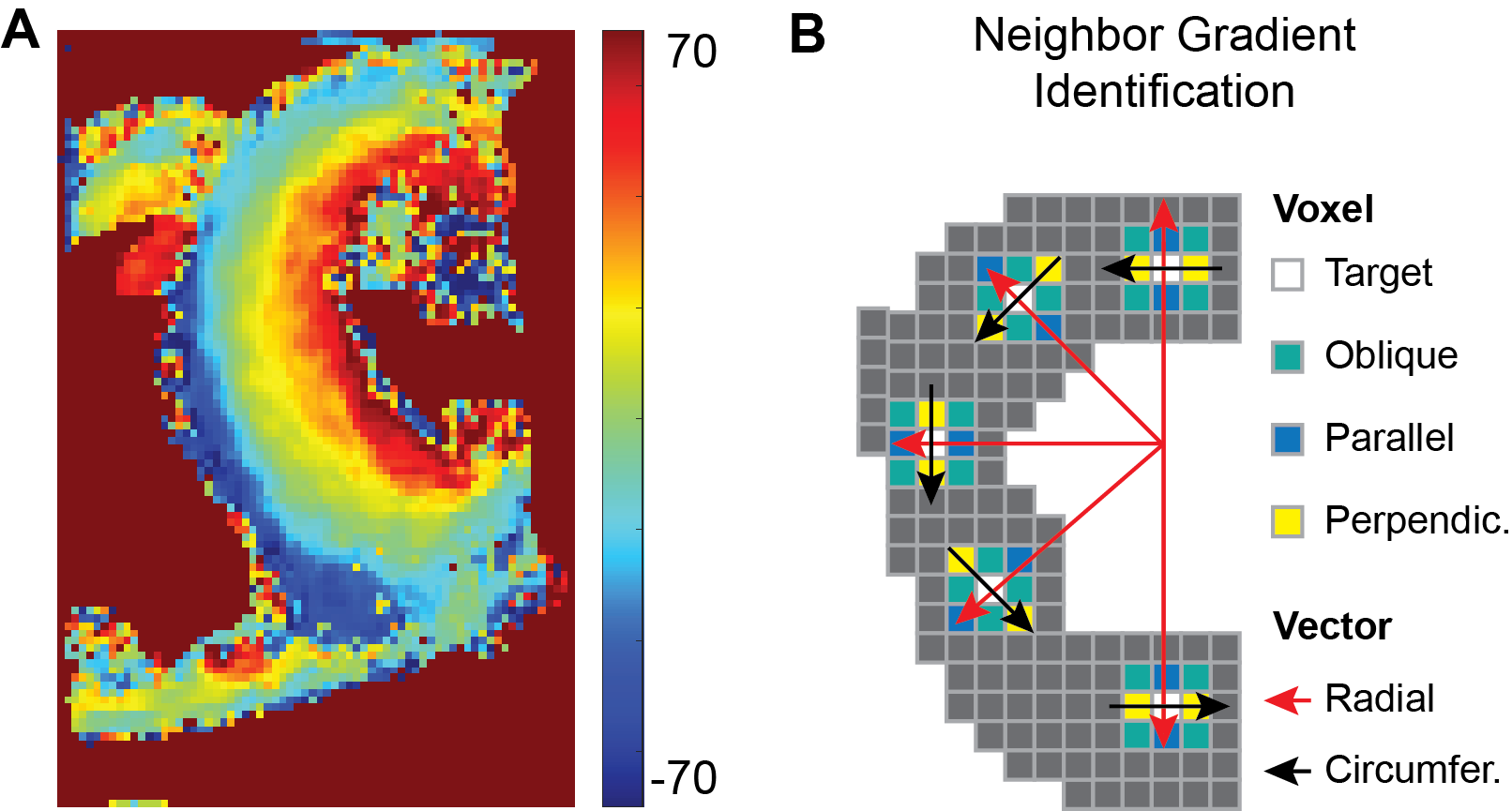
Sub-mm DTI scans were acquired on a 3T scanner with 80mT/m gradients (Prisma, Siemens) using a free-breathing M2-compensated spin echo sequence and a 64-channel radiofrequency coil, as previously described 1,2. Maps of mean diffusivity (MD), fractional anisotropy (FA), and helix angle (HA) were derived from the images. The HA maps (Fig. 1A) were further processed to derive local HA gradients in each voxel (Fig. 1B). Radial HA gradients were calculated between the target voxel and adjacent parallel voxels on a radial vector line (Fig. 1B, red line). Circumferential HA gradients were calculated between the target voxel and adjacent perpendicular voxels on a circumferential vector line (Fig. 1B, black line). Minimum and maximum HA gradients were calculated using the radial and circumferential vectors as well as oblique vectors between neighboring voxels (Fig. 1B). Little difference was seen between unidirectional and bidirectional calculations of the gradients, and unidirectional gradients (endo-to-epi for radial and counterclockwise for circumferential) were, therefore, used. HA gradients were calculated in degrees/mm and the angle between two voxels forming a gradient was classified as radial (angle of 0-30o), oblique (angle of 30-60o) or circumferential (angle of 60-90o) . Statistical comparisons between CTL and AS were done using unpaired t-tests with values expressed as mean ± standard deviation. DTI-tractography was performed in subjects with AS to evaluate the relationship between local HA gradients and tract coherence.Results
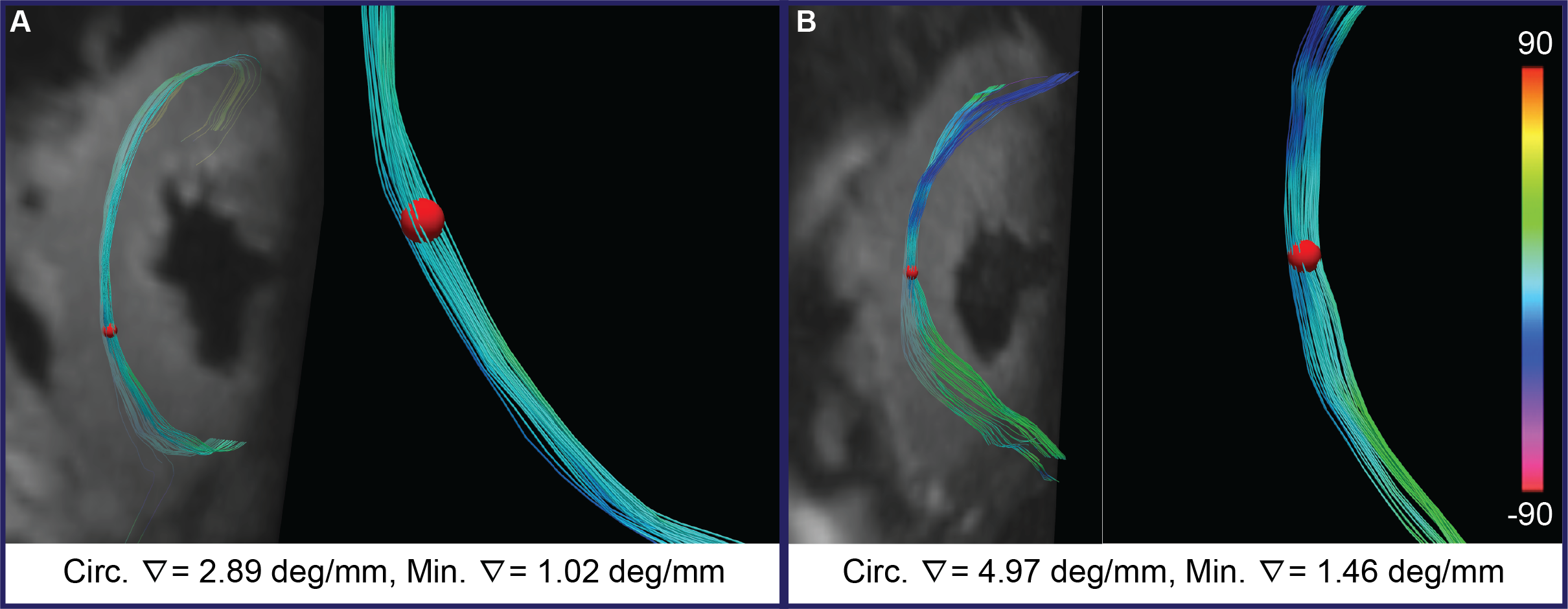
The myocardium in the midsystolic b50 images was significantly thicker in AS (15.4±1.4mm vs. 10.9±1.6mm, p<0.0001, Fig. 2I). No significant differences were observed in MD (1.41±0.11*10-3mm2/ms vs. 1.41±0.11*10-3mm2/ms, p=0.72, Fig. 2J) or FA (0.335±0.021. vs. 0.325±0.017, p=0.49, Fig. 2K). HA range was increased in AS subjects, but did not reach significance (110±8° vs. 106±6°, p=0.56, Fig. 2L). By contrast, radial gradient (Fig. 3-column 1) was significantly reduced in AS vs CTL (8.0±0.8°/mm vs. 10.2±1.8°/mm, p=0.001, Fig. 3M). There was no significant difference in circumferential HA gradient (3.78±1.1°/mm vs. 3.31±0.53°/mm, p=0.46, Fig 3-column 2). A strong trend towards a lower minimum HA gradient (Fig. 3-column 3) was seen in AS (1.28±0.18°/mm vs. 1.50±0.27°/mm, p=0.064, Fig. 3O) but no significant differences were seen in maximum HA gradient (12.1±2.1°/mm vs. 13.2±2.1°/mm, p=0.43, Fig. 3-column 4). The angle between the voxels forming the minimum HA gradient (Fig. 3-column 5) was significantly less circumferential in AS vs CTL (64±6° vs. 73±4°, p=0.0013, Fig. 3P). Similarly, the direction of the maximum HA gradient (Fig. 3-column 6) was significantly less radial in AS (24.8±4.3° vs. 17.4±2.6°, p=0.0017, Fig. 3R). Tractography in subjects with AS revealed that high local HA gradients correlated with poor tract coherence (Fig. 4).Discussion
The approach we present evaluates the microstructure of the heart with unheralded (sub-mm) spatial resolution, but in a reduced field-of-view. Much like MR-spectroscopy or T2* mapping, which are frequently limited to the septum, our approach is suited to conditions that affect the heart globally. The myocardium in AS undergoes global (symmetric) hypertrophy but our data suggest that this is well tolerated without a loss of microstructural coherence. HA gradient mapping could provide novel insights into the microstructure of the heart in a broad range of cardiovascular conditions.Conclusions
DTI of the heart with sub-mm in-plane resolution facilities the calculation of local HA gradients and the generation of a family of HA gradient maps. We show, using these maps, that the myocardium in patients with severe, but well-compensated, AS maintains its microstructural coherence.Acknowledgements
No acknowledgement found.References
1. Nguyen CT, Christodoulou AG, Coll-Font J, Ma S, Xie Y, Reese TG, Mekkaoui C, Lewis GD, Bi X, Sosnovik DE and Li D. Free-breathing diffusion tensor MRI of the whole left ventricle using second-order motion compensation and multitasking respiratory motion correction. Magn Reson Med. 2021;85:2634-2648.
2. Rock CA, Chen IY, Philip AL, Keil B, Nguyen CT, David E. Sosnovik DE. Evaluation of Cardiac Microstructure in Patients with Severe Aortic Stenosis Using Diffusion Tensor MRI with Submillimeter Resolution. In: ISMRM & ISMRT Annual Meeting & Exhibition. 2023 June 03-08 June 2023; Toronto, ON, Canada. Abstract No 0170.
Figures
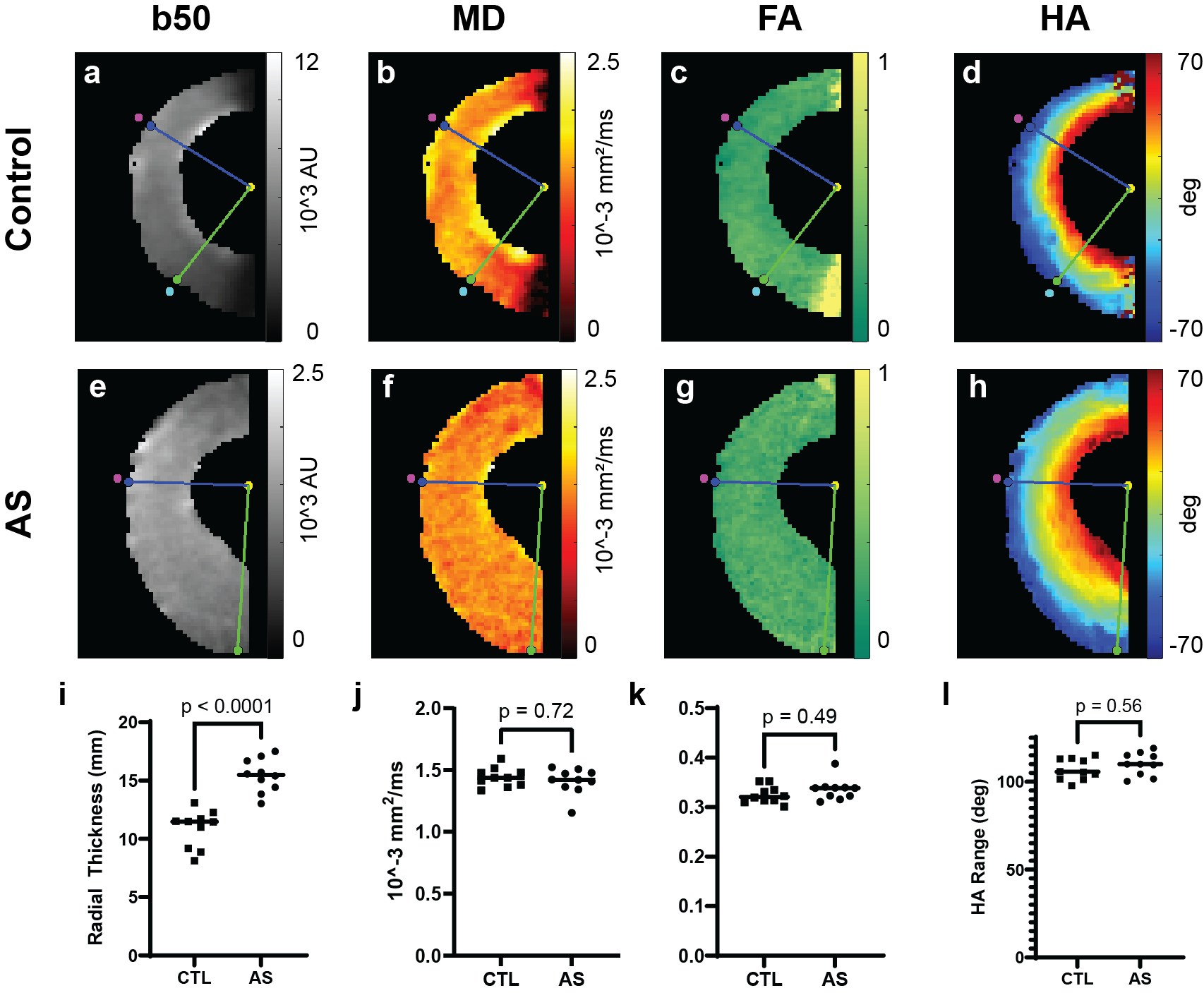
Comparison of conventional DTI-derived metrics in subjects with severe aortic stenosis (AS) and age-matched controls (CTL). (a-l) b50 images and maps of MD, FA and HA are shown. (i) Myocardial thickness in the b50 images, acquired in midsystole, was significantly increased in the AS subjects (15.4±1.4mm vs. 10.9±1.6mm, p = <0.001). No differences were seen in MD (j) and FA (k) between the AS subjects (n=10) and age-matched controls (n=10). HA range trended upwards in the AS subjects but did not reach significance (l).
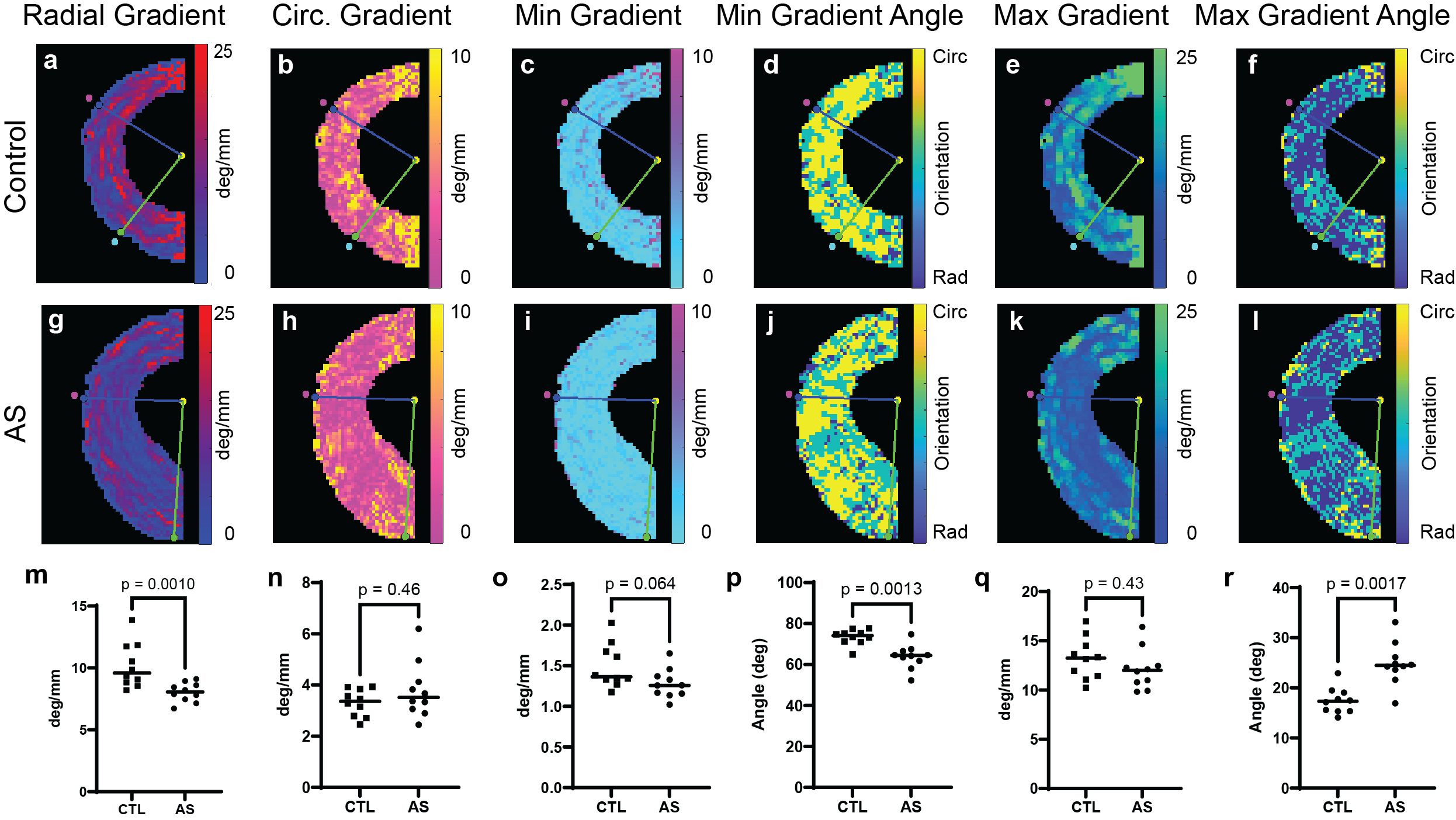
HA Gradient maps in aortic stenosis. (a-l) Maps of radial, circumferential (circ.), min and max HA gradient are shown with the orientation of min and max HA gradients. (m) Radial HA gradient was significantly reduced in aortic stenosis (AS) hearts. (n-o) No significant difference in circ. HA gradient were seen, however, a strong trend toward a lower min HA gradient in AS was present. (p) The min HA gradient in AS was significantly less circumferential. (q-r) No significant differences were seen in the max HA gradient magnitude, however, the orientation was significantly less radial in AS.