1818
Differentiating Myocardial Scar and Viable Myocardium without Gadolinium Contrast using Native Cardiac MRF Maps and Synthetic Images1Biomedical Engineering, University of Michigan, Ann Arbor, MI, United States, 2Radiology, University of Michigan, Ann Arbor, MI, United States, 3University Hospitals Cleveland Medical Center, Cleveland, OH, United States, 4School of Medicine, Case Western Reserve University, Cleveland, OH, United States
Synopsis
Keywords: Data Processing, Contrast Agent
Motivation: Late Gadolinium Enhancement (LGE) imaging is the gold-standard CMR imaging for distinguishing heart tissue viability. However, not all patients can receive gadolinium-based contrast agent. Native T1 have been proposed in place of LGE.
Goal(s): This study explores pre-contrast cardiac MRF T1 and T2 measurements as potential indicators of ischemic myocardial scar.
Approach: Native T1 and T2 values were measured using cMRF in eleven ischemic patients using ROIs in both scar and non-scar myocardial tissue identified through LGE imaging.
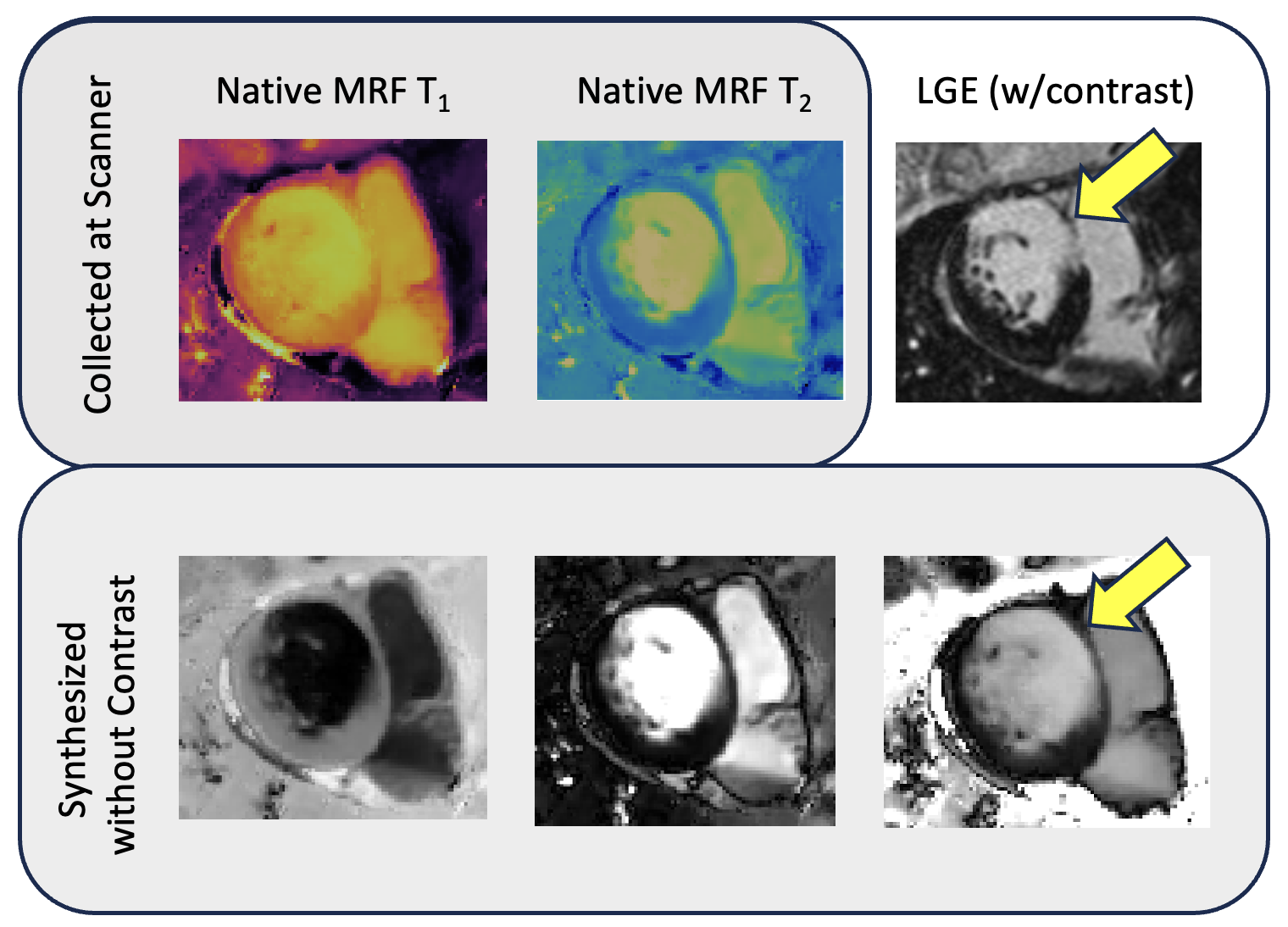
Results: Native cMRF measurements differ between scar and non-scar areas. Synthetic images from these maps highlight scar tissue, offering a potential LGE imaging alternative.
Impact: Native cMRF T1 and T2 maps and synthetic images derived from these maps may enable differentiation of scar tissue from viable myocardium without the need for gadolinium-based contrast agents.
Introduction
Late gadolinium enhancement (LGE) cardiac magnetic resonance imaging (CMR) is considered the standard for the diagnosis of myocardial scar1. Many groups have sought alternative approaches that do not rely on gadolinium-based contrast agents to detect scar for specialized patient populations2. Among other quantitative metrics, native (non-contrast) T1 values have been suggested as a possible indicator of fibrosis2–7. Our group has explored cardiac Magnetic Resonance Fingerprinting (cMRF) for the efficient quantification of T1 and T2 values8. This study aims to evaluate whether native MRF T1 and T2 values are significantly different between viable myocardium and scar tissue in patients with ischemic cardiomyopathy, and conduct an initial exploration of synthetic imaging based on these native cMRF for the identification of scar tissue.Methods
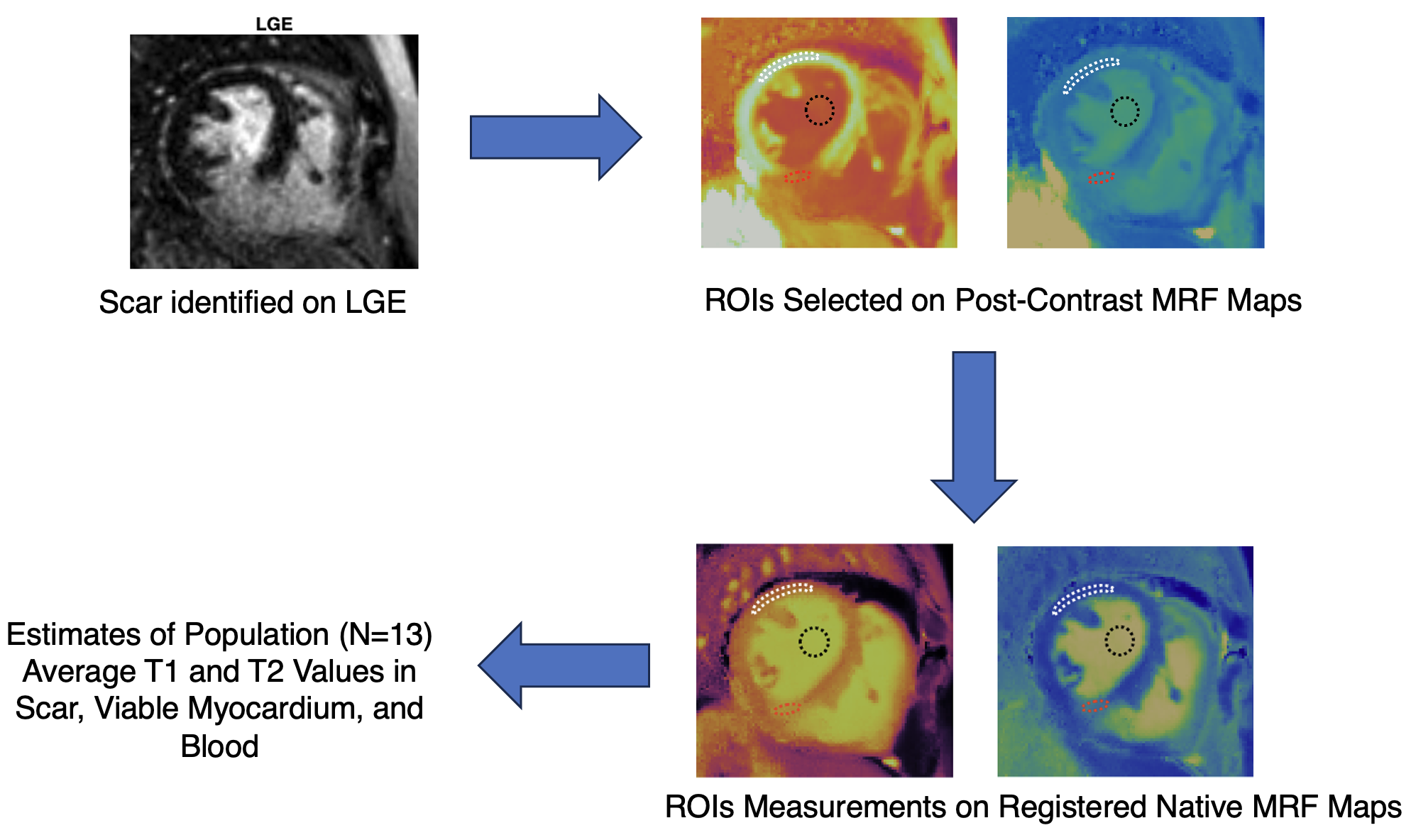
Thirteen cMRF scans acquired at 1.5T (MAGNETOM Aera, Siemens Healthineers, Erlangen, Germany) from eleven malepatients (ages: 38 - 80 years) with previous ischemic cardiomyopathy were analyzed. Short-axis cMRF scans using the sequence described in Hamilton, et al9 were acquired before and after injection of a gadolinium-based contrast agent. T1, T2, and M0 maps were estimated using a deep image prior10 reconstruction. LGE images were also collected in these slices.Areas of myocardial scar and viable myocardium, as well as LV blood pool, were visually identified on the LGE images, and manually segmented after affine registration of post-contrast to native cMRF maps, as depicted in Figure 1. Average values of native cMRF-based T1 and T2 from these three segmented regions were measured and compared using a Wilcoxon signed-rank test. These average values were then used to generate synthetic T1 and T2 weighted images, similar to the approach used in11. The following equations were used to generate scar-weighted images:
$$2 -(\frac{T_{1}}{T_{1}^{ROI}} + \frac{T_2}{T_{2}^{ROI}} )$$
Here T1 and T2 represent the values in the native cMRF maps of a given patient, T1ROI and T2ROI and denote the average values derived from the ROIs described above; as an example, setting T1ROI and T2ROI to the average values of T1 and T2 in blood is meant to null signal from blood. This formula was used to generate synthetic images from native cMRF maps in three patients with known scar. Note that the scans for one of these patients were not included in the ROI analysis in which average ROI values were derived.
Results
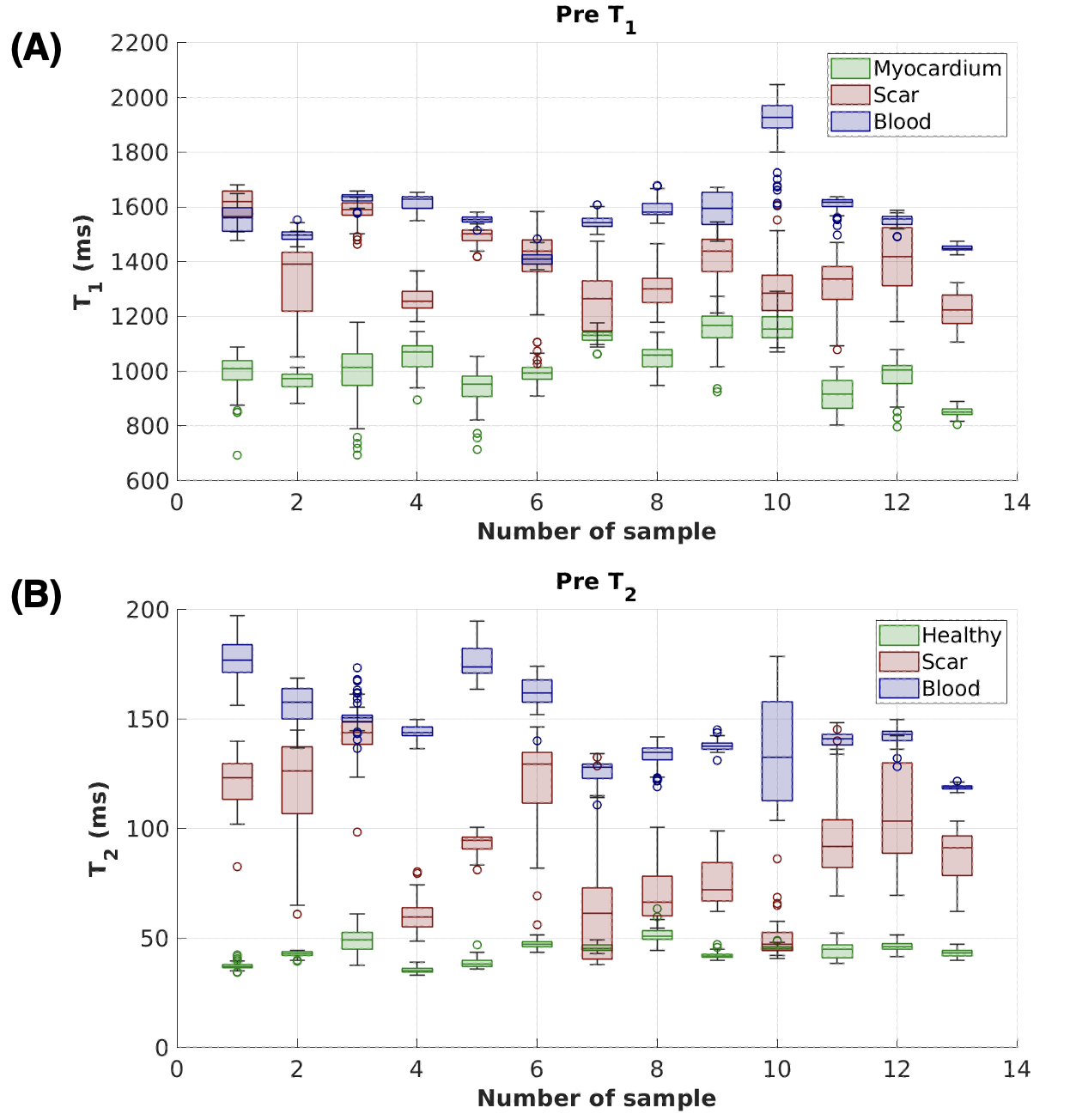
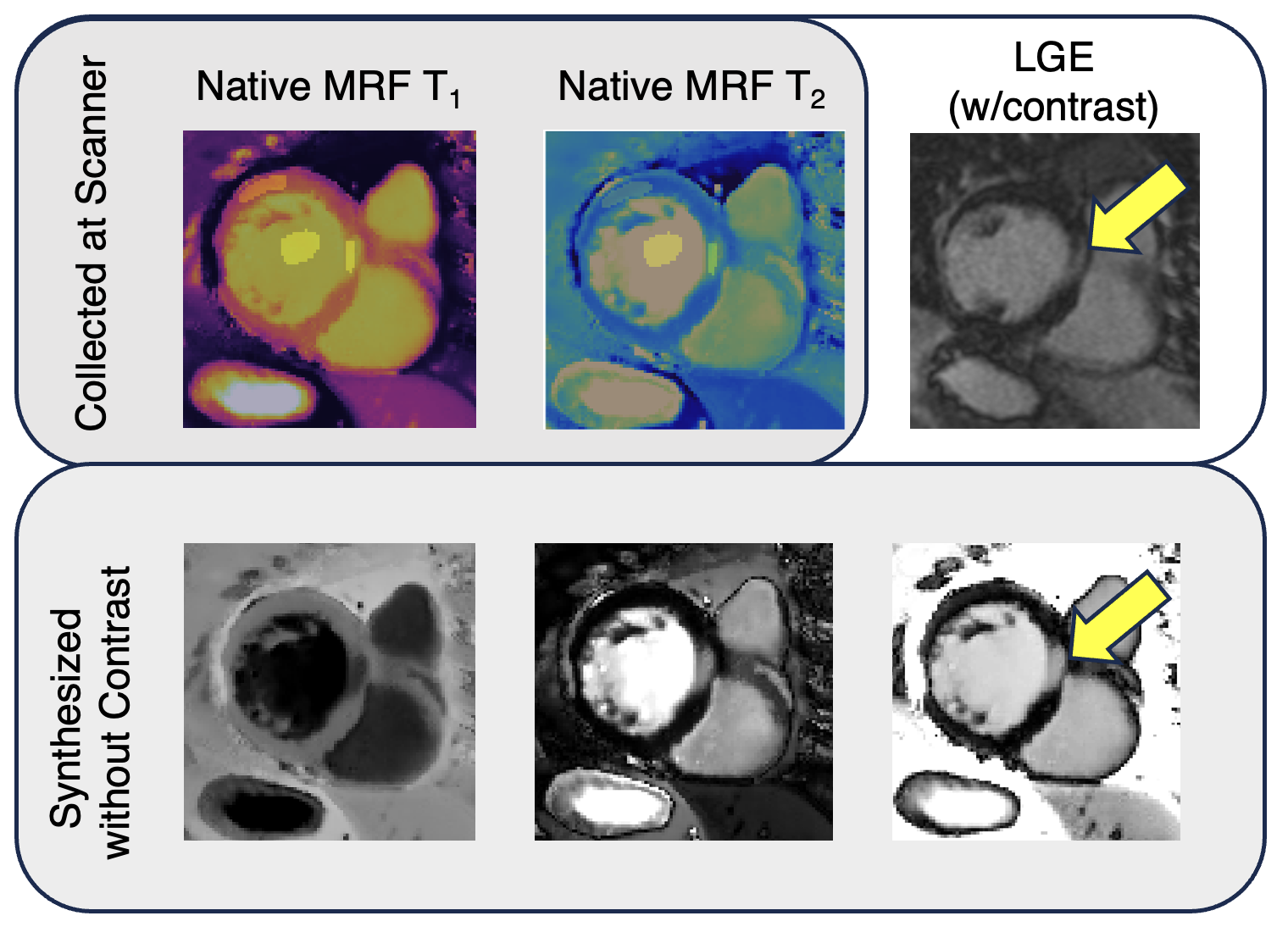
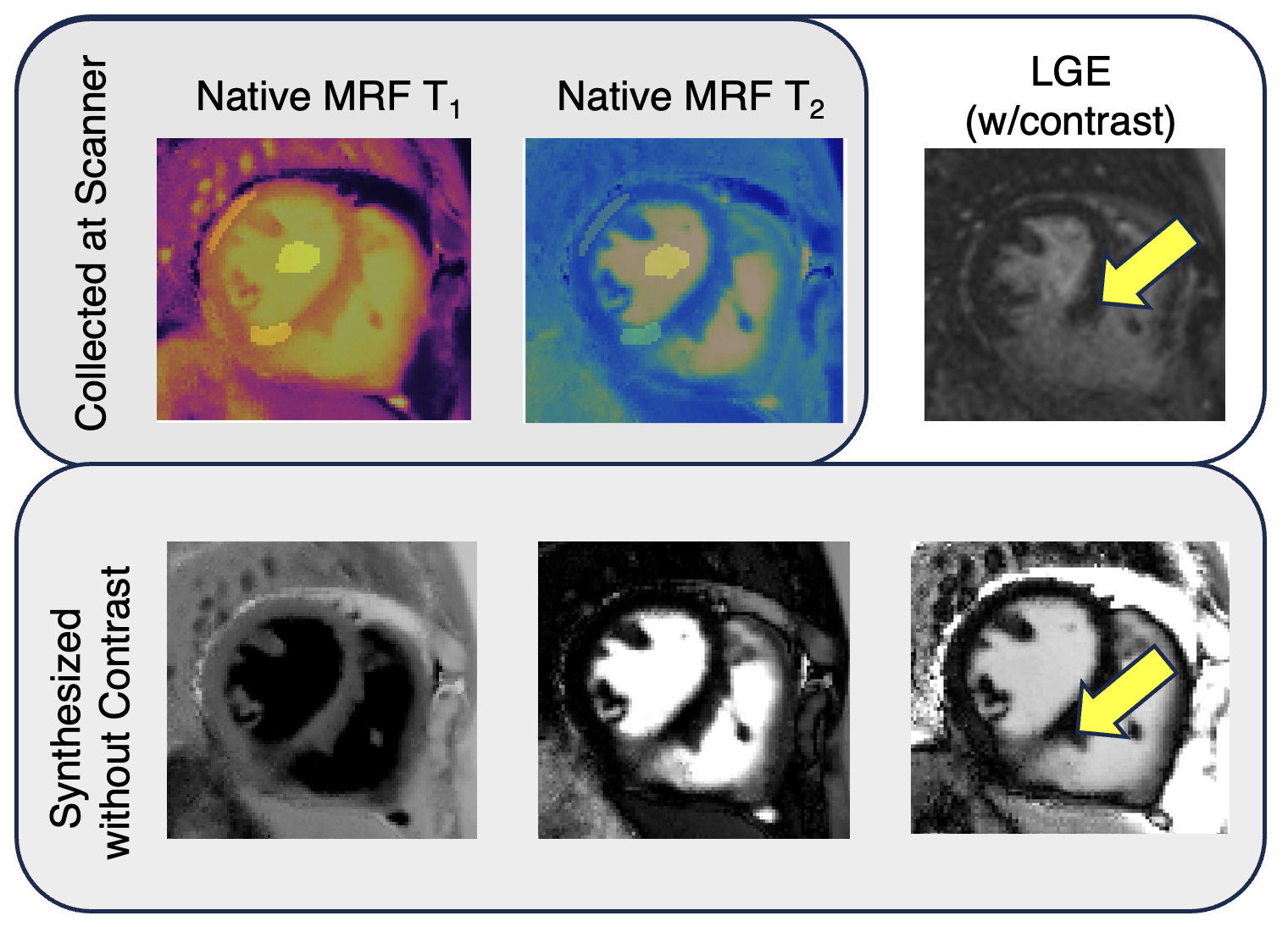
Average T1 and T2 values from viable and scarred myocardium across the thirteen scans with ischemic ROIs are plotted in Figure 2. The average native T1 and T2 values in viable myocardium were 1015.7±89.2 ms, and 43.4±4.5 ms, respectively, whereas average T1 and T2 values in scar were 1385.2±122.5 ms, and 94.8±27.9 ms. Significant differences between viable and nonviable myocardial T1 values (p<0.001,α=0.05), and T2 values (p<0.001, α=0.05) were found via a Wilcoxon signed-rank test; these average ROI values were used to generate the subsequent synthetic images. Native T1 and T2 maps, LGE, and three different scar-weighted images generated using only the native MRF data and average viable/scar/blood tissue T1 and T2 values are shown in Figures 3 through 5. The maps for the patients in Figures 3 and 4 were included in the ROI analysis; the maps for the patient depicted in Figure 5 were not included in the ROI analysis.Discussion
cMRF-derived native T1 and T2 values in scar were significantly higher than values in regions of viable myocardium. These results suggest that tissue properties measured with cMRF may enable differentiation between these tissue types, without the need for a gadolinium-based contrast agent. Additionally, synthetic images could be designed to highlight areas of scar using native cMRF maps, even in a patient who was not included in the ROI analysis, indicating that this approach may be generalizable when information about the specific scar native T1 and T2 values for a given patient are not available (as would be the case in a fully non-contrast protocol). This study has several limitations, including the use of only a small number of patients, a focus on patients with ischemic cardiomyopathy, manual segmentation of ROIs, unoptimized scar-weighted images, and lack of quantitative analysis of scar burden visible in these images. Future research will expand the patient populations studied, work towards an optimized scar-weighted sequence, and assess the area of scar apparent in LGE and native cMRF-based synthetic images.Conclusion
Native T1 and T2 mapping with MRF may enable differentiation between viable myocardium and scar. Synthetic images highlighting scar could be generated from native cMRF maps, which after optimization could potentially be used in place of LGE imaging for identifying myocardial scar tissue.Acknowledgements
No acknowledgement found.References
- Jenista ER, Wendell DC, Azevedo CF, et al. Revisiting how we perform late gadolinium enhancement CMR: insights gleaned over 25 years of clinical practice. J Cardiovasc Magn Reson. 2023;25(1):18. doi:10.1186/s12968-023-00925-0
- Graham-Brown MP, Singh AS, Gulsin GS, et al. Defining myocardial fibrosis in haemodialysis patients with non-contrast cardiac magnetic resonance. BMC Cardiovasc Disord. 2018;18(1):145. doi:10.1186/s12872-018-0885-2
- Gulani V, Calamante F, Shellock FG, Kanal E, Reeder SB. Gadolinium deposition in the brain: summary of evidence and recommendations. Lancet Neurol. 2017;16(7):564-570. doi:10.1016/S1474-4422(17)30158-8
- Yanagisawa F, Amano Y, Tachi M, Inui K, Asai K, Kumita S. Non-contrast-enhanced T1 Mapping of Dilated Cardiomyopathy: Comparison between Native T1 Values and Late Gadolinium Enhancement. Magn Reson Med Sci. 2019;18(1):12-18. doi:10.2463/mrms.mp.2017-0136
- Bull S, White SK, Piechnik SK, et al. Human non-contrast T1 values and correlation with histology in diffuse fibrosis. Heart. 2013;99(13):932-937. doi:10.1136/heartjnl-2012-303052
- Małek ŁA, Werys K, Kłopotowski M, et al. Native T1-mapping for non-contrast assessment of myocardial fibrosis in patients with hypertrophic cardiomyopathy — comparison with late enhancement quantification. Magn Reson Imaging. 2015;33(6):718-724. doi:10.1016/j.mri.2015.04.001
- Toward Replacing Late Gadolinium Enhancement With Artificial Intelligence Virtual Native Enhancement for Gadolinium-Free Cardiovascular Magnetic Resonance Tissue Characterization in Hypertrophic Cardiomyopathy. doi:10.1161/CIRCULATIONAHA.121.054432
- Ma D, Gulani V, Seiberlich N, et al. Magnetic resonance fingerprinting. Nature. 2013;495(7440):187-192. doi:10.1038/nature11971
- Hamilton JI, Pahwa S, Adedigba J, et al. Simultaneous Mapping of T1 and T2 Using Cardiac Magnetic Resonance Fingerprinting in a Cohort of Healthy Subjects at 1.5T. J Magn Reson Imaging. 2020;52(4):1044-1052. doi:10.1002/jmri.27155
- Hamilton JI. A Self-Supervised Deep Learning Reconstruction for Shortening the Breathhold and Acquisition Window in Cardiac Magnetic Resonance Fingerprinting. Front Cardiovasc Med. 2022;9:928546. doi:10.3389/fcvm.2022.928546
- Rashid I, Al-Kindi S, Rajagopalan V, et al. Synthetic multi-contrast late gadolinium enhancement imaging using post-contrast magnetic resonance fingerprinting. NMR Biomed. n/a(n/a):e5043. doi:10.1002/nbm.5043
Figures