1817
Simultaneous 3D whole-heart T2 mapping and coronary angiography (3D-T2A)1Kumamoto University, Kumamoto-shi, Japan, 2Philips Japan, Tokyo-to, Japan
Synopsis
Keywords: Myocardium, Myocardium, T2mapping
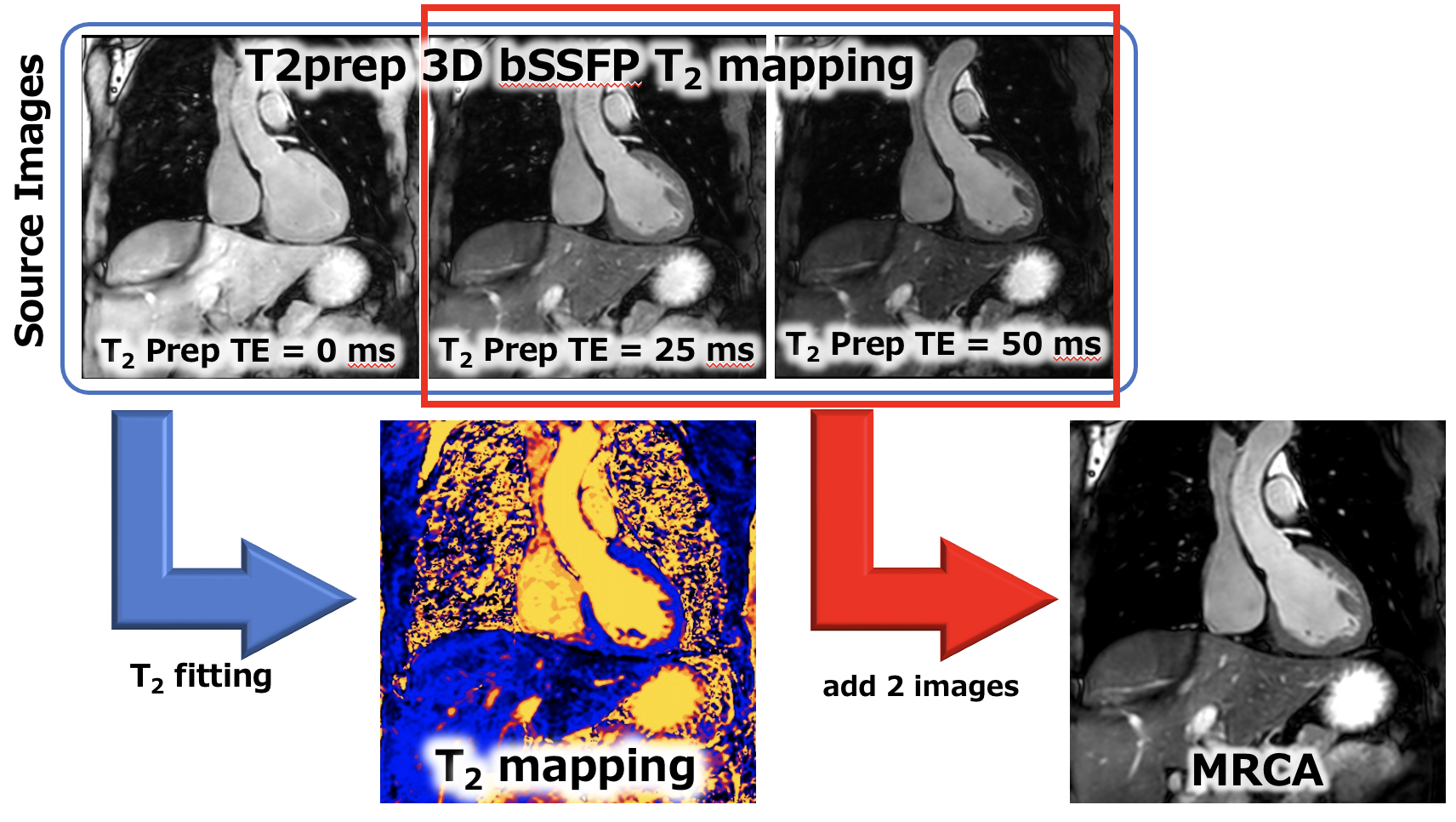
Motivation: We focused on the similarity between 3D T2prep T2 mapping and whole-heart MRCA and developed a new sequence for simultaneous T2 mapping and MRCA sequence.
Goal(s): Our goal of this study is to validate the simultaneous acquisition of 3D T2 mapping with whole heart MRCA.
Approach: We visually assessed the image quality of 3D T2 mapping and MRCA. T2 values were compared with 2D T2 mapping (2D-GRASE).
Results: This method, which enables simultaneous acquisition of 3D T2 mapping and MRCA, can provide stable image quality and T2 values.
Impact: Our method, which enables simultaneous acquisition of 3D T2 mapping and MRCA, can provide stable image quality and T2 values, and will be of great benefit in future imaging.
INTRODUCTION
The use of T2 mapping sequences to detect and quantify myocarditis and edema has been recommended. However, current T2 mapping sequence is performed in two dimensions, with limited volume coverage and multiple breath holds are needed to cover wider volume. T2 mapping has also been reported for noncardiac applications, evaluating right ventricular (RV) and left ventricular (LV) blood pool T1 and T2 values in patients with chronic thromboembolic pulmonary hypertension (CTEPH) and correlating them with pulmonary hemodynamics. Three-dimensional (3D) myocardial T2 mapping methods cover the whole heart and may allow better characterization of complex diffuse pathological findings, but require longer acquisition times (1,2). A free-breathing 3D whole heart T2 mapping framework with high isotropic resolution and clinically feasible scan time (approximately 8 minutes) has recently been proposed (3). This method was reported to be in good agreement with conventional 2D mapping in a small cohort of healthy patients with low T2 bias in the phantom.Magnetic resonance coronary angiography (MRCA), on the other hand, is also widely used for relatively gross imaging of the coronary arteries, and cardiac-gate and respiration-gate (free-breathing), T2 preparation, and 3D steady-state free-precession (SSFP) sequences are now widely used (4-6).In this study, we focused on the similarity between these two sequences (3D T2 mapping and MRCA). Our purpose of this study is to validate the simultaneous acquisition of 3D T2 mapping with whole heart MRCA.METHODS
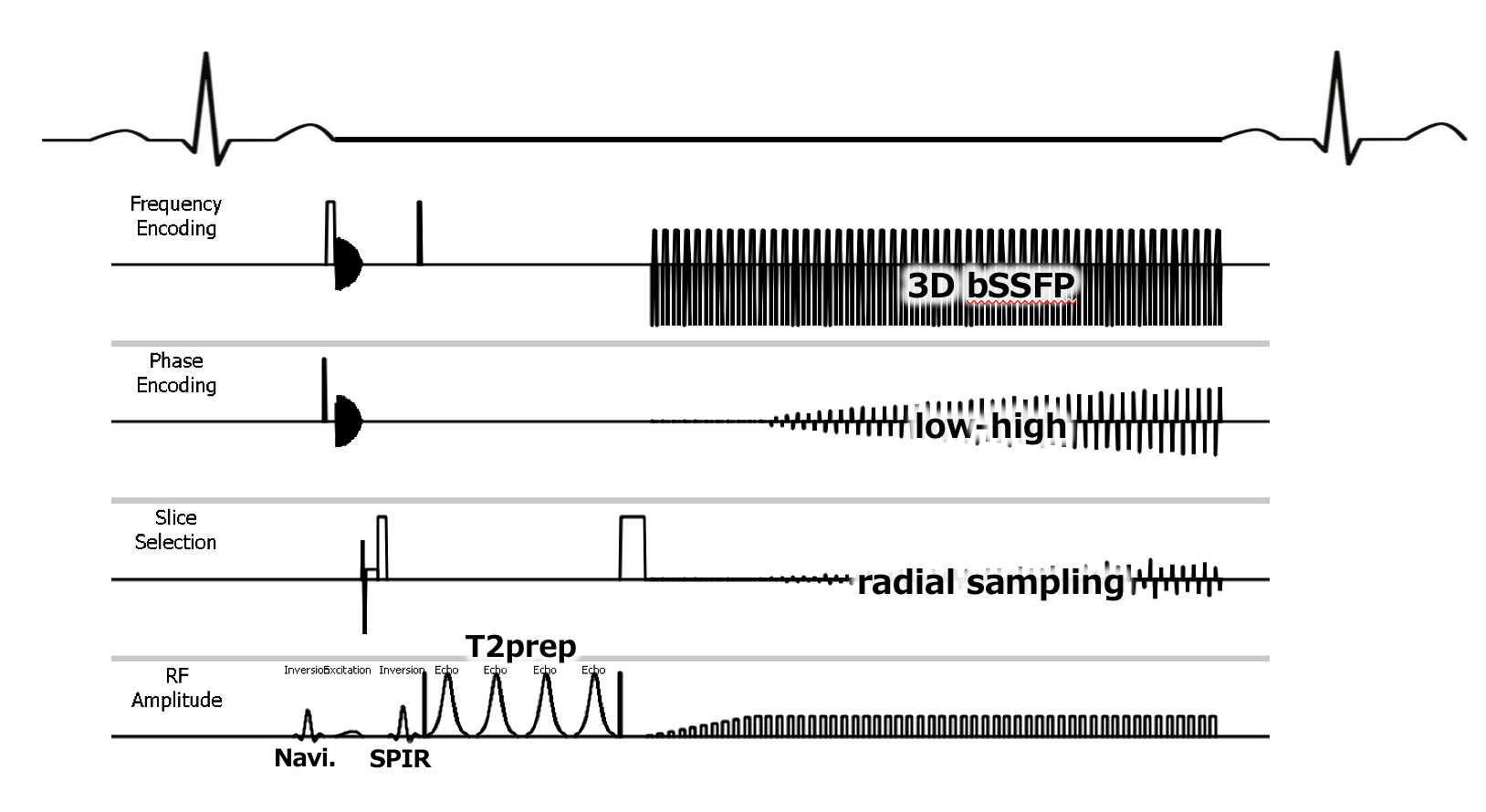
Cardiac MRI acquisitions were performed in the supine position with a 3-T MRI scanner (Ingenia 3.0T CX; Philips) with a spine coil and a body array coil.The investigated free-breathing 3D bSSFP whole-heart T2 mapping sequence (Fig. 1) was shown(6). The subjects were five healthy volunteers who consented to the study. Scan parameters of 3D T2 mapping with MRCA sequence was as follows: TR/TE = 2.2/1.1 ms, slices thickness = 2.0 mm, voxel size = 2.0 × 2.0 × 2.0mm, CS factor = 6.0, slices = 300, acquisition duration = 118.0 ms, startu-up echo = 10, k-space trajectory = low-high, Flip angle = 70 degree, fat suppression = SPIR, T2prep TE = 0, 25, 50 ms, coronal orientation, cardiac trigger = end diastole and acquisition time = 5:26 (HR = 60 bpm). Figure 2 shows a schematic of T2 mapping and MRCA imaging. For quantitative evaluation, T2 values were measured from 2D T2 mapping (2D-GRASE) and 3D T2mapping.RESULTS
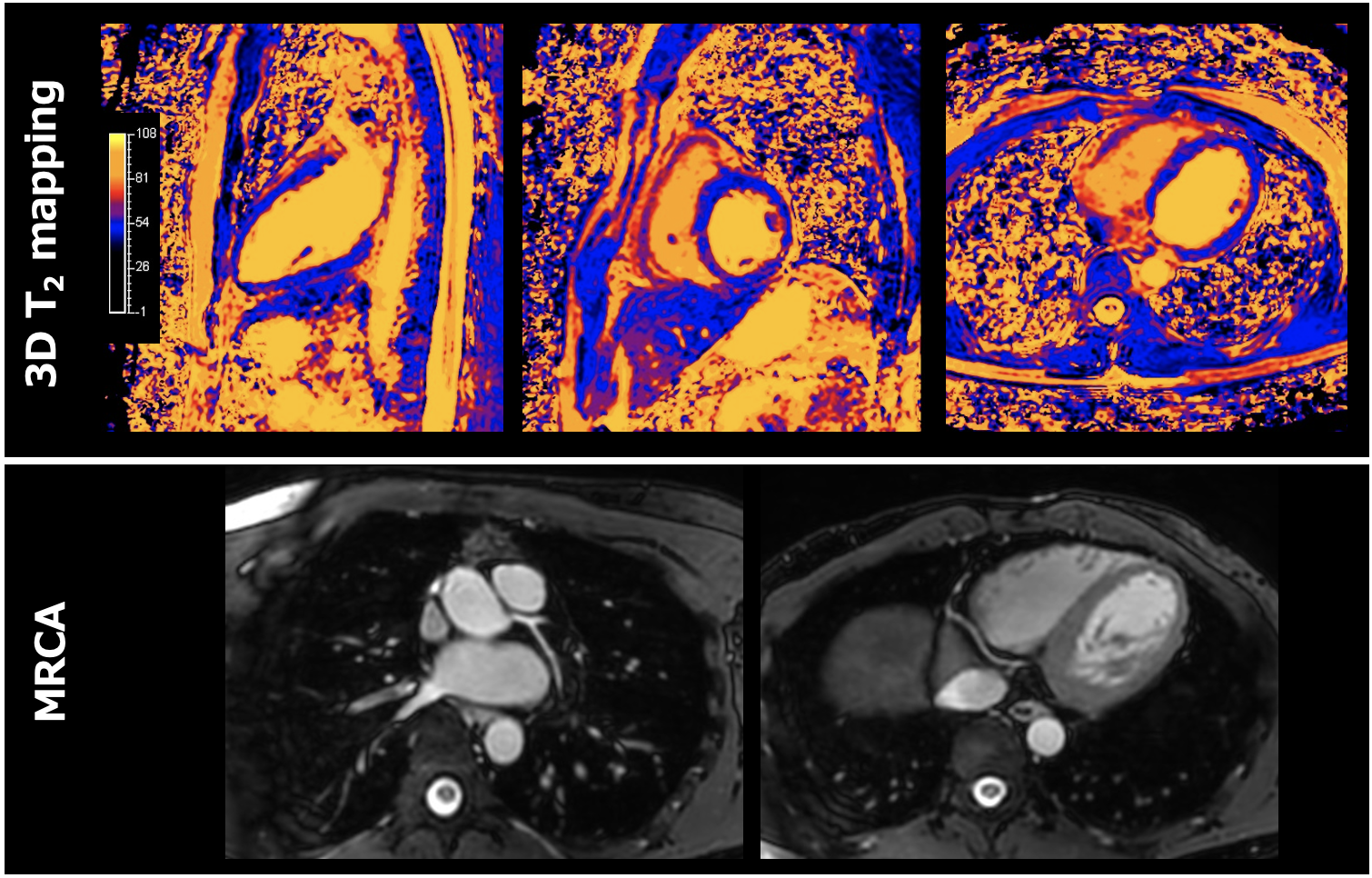
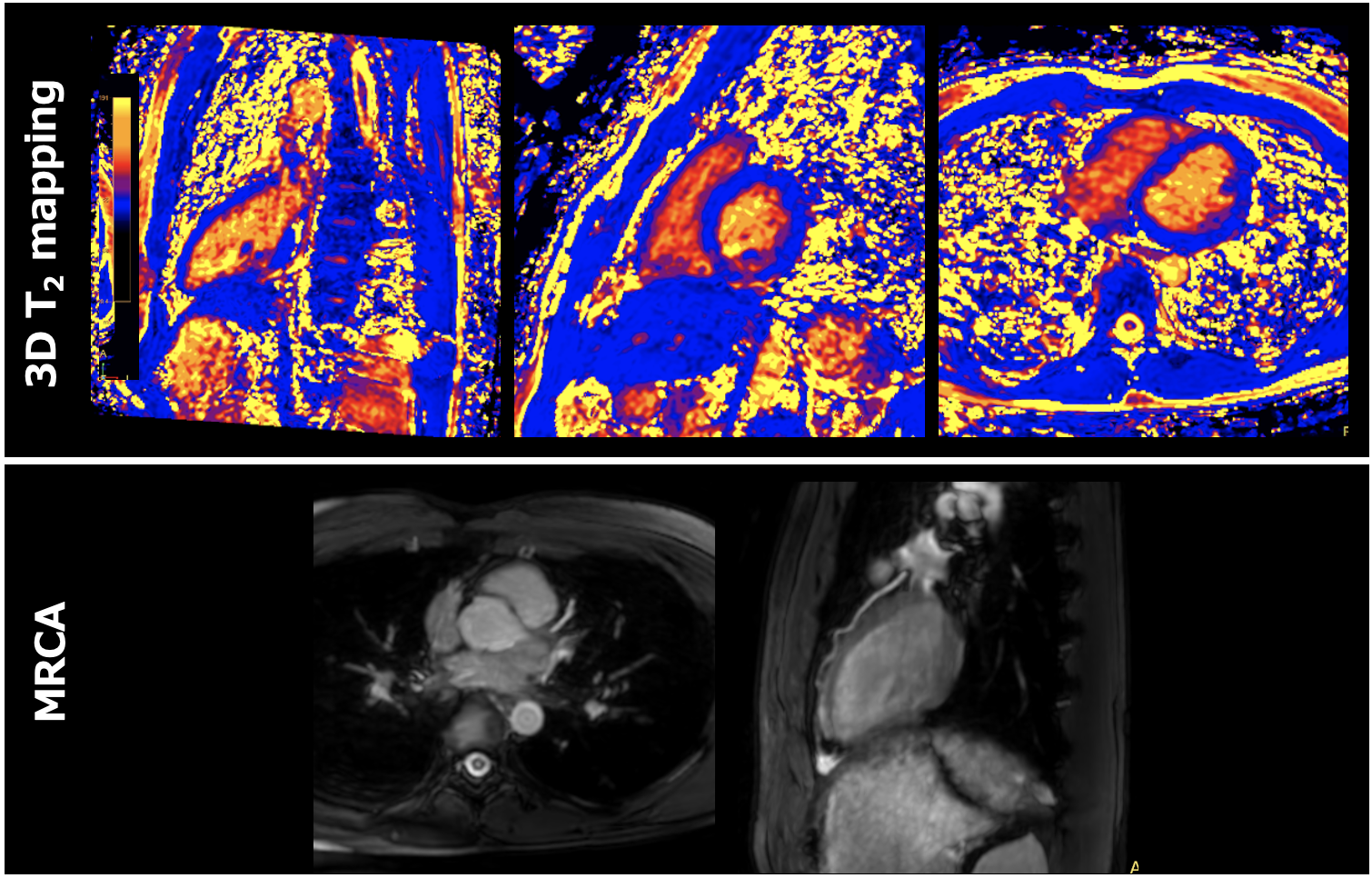
The T2 values obtained from 3D T2 mapping and 2D-GRASE were 46 ± 2 ms and 44 ± 2 ms, respectively. Figures 3 and 4 show representative T2 mapping and MRCA images of volunteers with HR=60 bpm and HR=90 bpm. The averaged actual scan time of all volunteers was 8 minutes ± 35 seconds.DISCUSSION
There was no significant difference between 3D T2 mapping and 2D GRASE T2 values. This indicates the stability of 3D T2 mapping. In the volunteer images, neither T2 mapping nor MRCA showed significant image quality loss even in the high heart rate volunteers, suggesting that it can be adapted in any patients.Limitations include volunteer evaluation only, 3-T MR system only, and lack of agreement on T2 mapping methods.CONCLUSION
This method, which enables simultaneous acquisition of 3D T2 mapping and MRCA, can provide stable image quality and T2 values, and will be of great benefit in future imaging.Acknowledgements
No acknowledgement found.References
1. Ding H, Fernandez-de-Manuel L, Schär M, et al. Three-dimensional whole-heart T2 mapping at 3T. Magn Reson Med 2015;74(3):803–816.
2. vanHeeswijkRB,PicciniD,FelicianoH,HullinR,SchwitterJ,StuberM.Self-navigated isotropic three-dimensional cardiac T2 mapping. Magn Reson Med 2015;73(4):1549– 1554.
3. Bustin A, Milotta G, Ismail TF, Neji R, Botnar RM, Prieto C. Accelerated free-breath- ing whole-heart 3D T mapping with high isotropic resolution. Magn Reson Med 2020;83(3):988–1002.
4. Tangcharoen T, Bell A, Hegde S, Hussain T, Beerbaum P, Schaeffter T, et al. Detection of coronary artery anomalies in infants and young children with congenital heart disease by using MR imaging. Radiology. (2011) 259:240–47.
5. Su JT, Chung T, Muthupillai R, Pignatelli RH, Kung GC, Diaz LK, et al. Usefulness of real-time navigator magnetic resonance imaging for evaluating coronary artery origins in pediatric patients. Am J Cardiol. (2005) 95:679–82.
6. Lin L, Wang L, Zhang XN, Li X, Wang J, Shen ZJ, et al. A clinical strategy to improve the diagnostic accuracy of 1.5-T non-contrast MR coronary angiography for detection of coronary artery disease: combination of whole-heart and volume-targeted imaging. Eur Radiol. (2021) 31:1894–904.
Figures
Free-breathing 3D bSSFP whole-heart T2 mapping sequence with MRCA.