1815
Long term cardiac MRI surveillance in patients transplanted for ischemic cardiomyopathy: myocardial ECV and strain variation.1Radiolgy, Northwestern University Feinberg School of Medicine, Chicago, IL, United States
Synopsis
Keywords: Myocardium, Cardiovascular, Transplant, Heart Transplant, Ischemia, Ischemic Cardiomyopathy
Motivation: Ischemic dilated cardiomyopathy (DCM) is associated with low-grade chronic inflammation which may persist after heart transplantation (HTx) and impact graft function and tissue characteristics in the post-HTx period.
Goal(s): Our goal was verify whether any difference in graft tissue characteristics or function was evident during long-term follow up by cardiac MRI between patients transplanted for ischemic DCM and those transplanted for non-ischemic indications.
Approach: Longitudinal analysis of graft tissue mapping and 2D FTS was performed on patients transplanted for ischemic DCM (n=13) and non-ischemic indications (n=50).
Results: In the non-ischemic DCM cohort, tissue mapping and FTS parameters, ECV and GCS, worsened over time.
Impact: No effect of pre-HTx low grade inflammation was evident on graft tissue characteristics and function in patients transplanted for ischemic DCM. Cardiac MRI may play an important role in long term monitoring of patients undergoing HTx.
INTRODUCTION
Long term monitoring and surveillance is recommended for patients after undergoing heart transplant (HTx). Cardiac magnetic resonance imaging (CMR), along with two-dimensional (2D) feature-tracking strain (FTS) is a powerful non-invasive tool that is useful for evaluation of tissue mapping and 2D FTS characteristics. Ischemic heart disease, one potential avenue of progression to end stage cardiomyopathy and eventually to heart transplant (HTx), can be associated with low grade local/systemic inflammation1-5 which may persist in the post-operative period. The aim of our study was to evaluate whether any tissue mapping or FTS differences exist and how they change over time between patients who underwent HTx for ischemic dilated cardiomyopathy (DCM) and patients who were transplanted for non-ischemic disease.METHODS
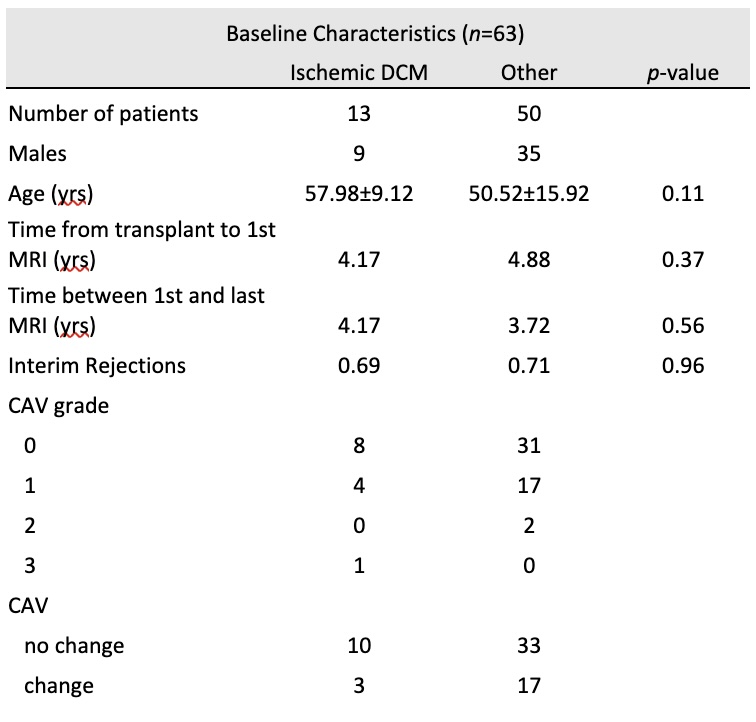
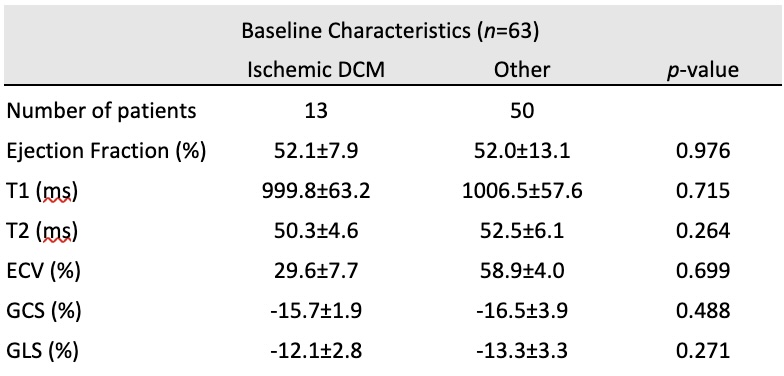
Using an IRB-approved protocol, 63 patients who received CMR as part of their surveillance for post-HTx cardiac allograft vasculopathy (CAV), were analyzed. Patients were separated into two groups, based on the etiology of the primary disease leading to HTx: Group 1 included patients with end-stage ischemic cardiomyopathy and group 2 included end stage non-ischemic cardiac disease leading to HTx. Group characteristics are reported in Table 1. Standard steady state (SSFP) sequences were utilized for cine imaging acquisition, T1 mapping was performed using a modified Look-Locker inversion recovery technique and T2-mapping was based on acquisition of three T2-prepared SSFP using T2-prep times. The baseline timepoint was the first post-HTx CMR scan at the time when patients entered CAV monitoring (1 or more years post-HTx), and the follow-up timepoint was the patient’s most recent CMR (less than 11 years post-HTx). Data collected from the CMRs was evaluated for both absolute change and percentage change from baseline. All parameters were indexed to time between scans (in years). Data are reported in Table 2 as mean and standard deviation, and level of significance are reported for comparisons.RESULTS
At baseline, no significant differences were found between the two groups in evaluation of cardiac function and 2D FTS (ejection fraction, global longitudinal strain (GLS), and global circumferential strain (GCS)) and tissue characteristics (T1, T2, extracellular volume (ECV)) (Table 2).From our longitudinal analysis, patients transplanted for ischemic DCM showed a significant difference in percentual GCS (considered as absolute value) decrease over time as well as in extracellular volume (ECV) variation, compared with patients transplanted for non-ischemic cause. (Figures 1, 2, and 3).DISCUSSION
In the post-HTx follow-up CAV monitoring, there was no evidence of worsening myocardial tissue or function parameters over time in patients transplanted for end-stage ischemic cardiomyopathy, compared to patients transplanted for non-ischemic disease. Moreover, in our longitudinal analysis, ischemic DCM HTx patients showed an attenuated increase in ECV and attenuated decrease of GCS during their post-HTx period.CONCLUSION
From our preliminary analysis, there is no evidence of a negative effect of ischemic DCM as a HTx indication on myocardial function and tissue characteristics in the post-transplant period (>1 year) in comparison to those transplanted for non-ischemic reasons. A subsequent and more comprehensive analysis, including systemic inflammatory markers, is warranted in these patients.Acknowledgements
No acknowledgement found.References
1.Libby P, Ridker PM, Maseri A. Inflammation and atherosclerosis. Circulation. 2002 Mar 5;105(9):1135-43. 2.Soehnlein, O., Libby, P. Targeting inflammation in atherosclerosis — from experimental insights to the clinic. Nat Rev Drug Discov 20, 589–610 (2021).
3.Robert A. Harrington, Targeting Inflammation in Coronary Artery Disease. N Engl J Med 2017; 377:1197-1198
4.Dennis Wolf, Klaus Ley, Immunity and Inflammation in Atherosclerosis. Circulation Research 2019;124:315–327
5.Sherer, Y., Shoenfeld, Y. Mechanisms of Disease: atherosclerosis in autoimmune diseases. Nat Rev Rheumatol 2, 99–106 (2006).
Figures
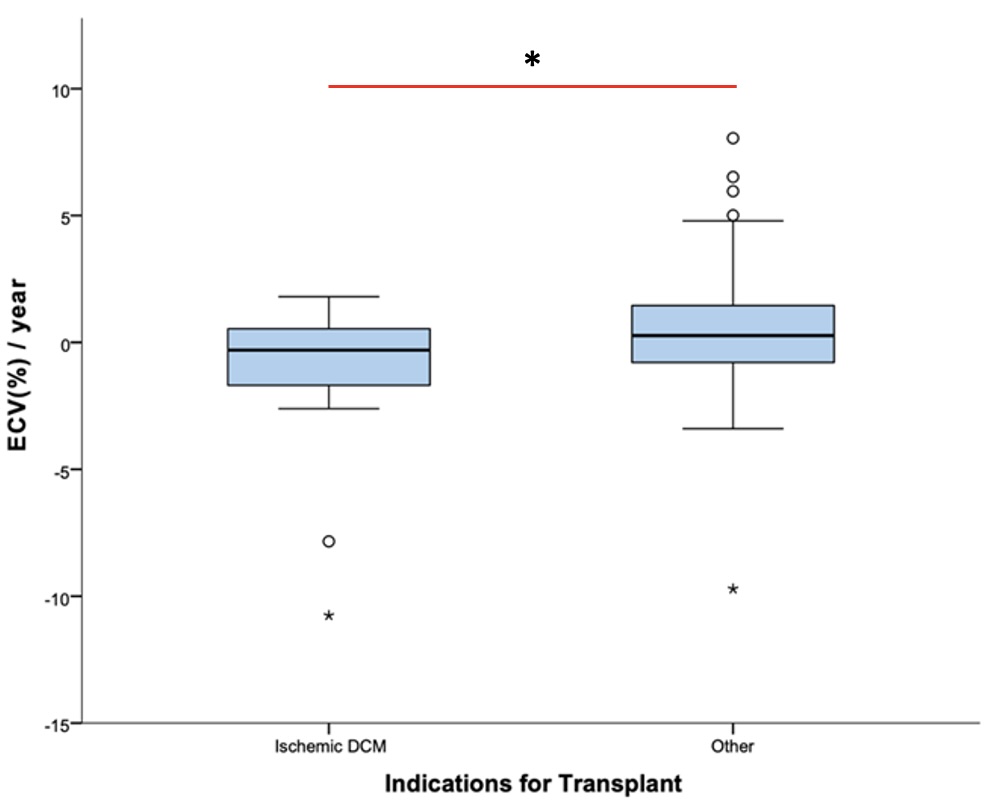
* = significance at level of p<0.05
Figure 1: Box plot depicting the absolute change in ECV (%) per year in HTx patients split into two groups based on indication for transplant (ischemic DCM and non-ischemic (Other)).
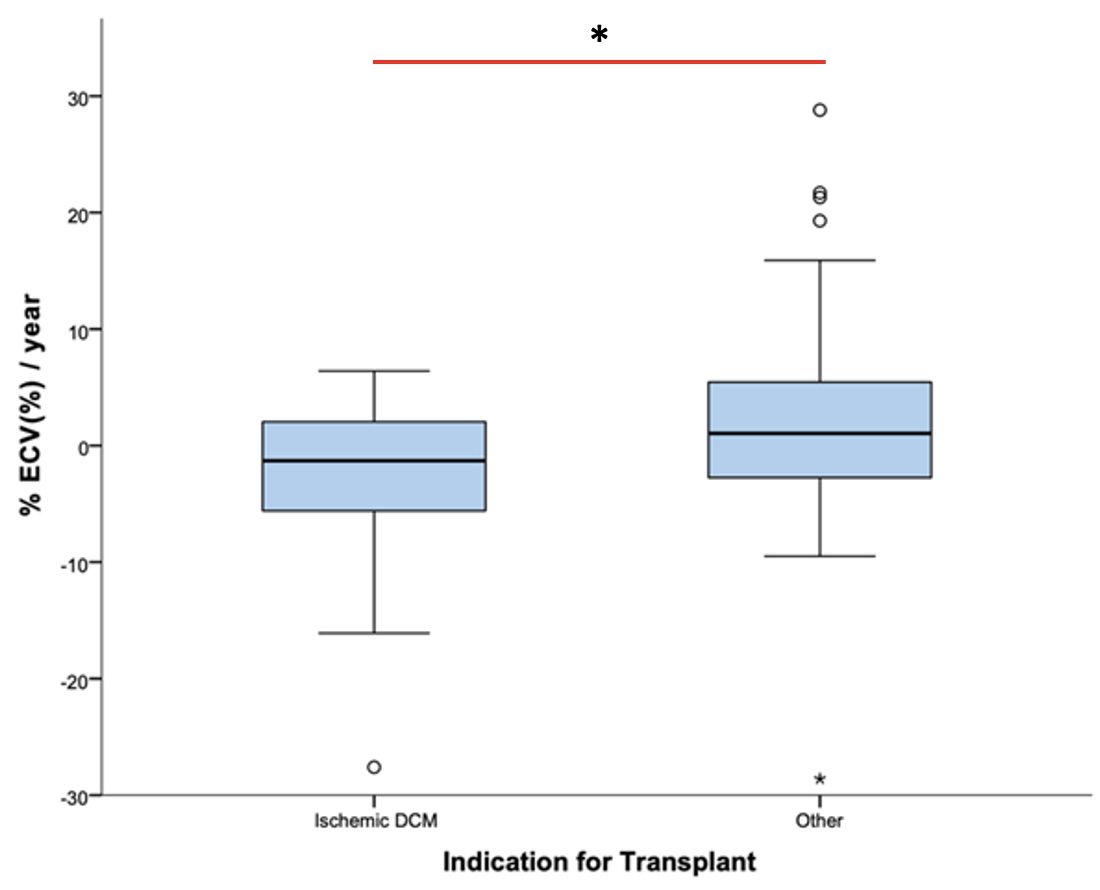
* = significance at level of p<0.05
Figure 2: Box plot depicting the percentage change in ECV (%) per year in HTx patients split into two groups based on indication for transplant (ischemic DCM and non-ischemic (Other)).
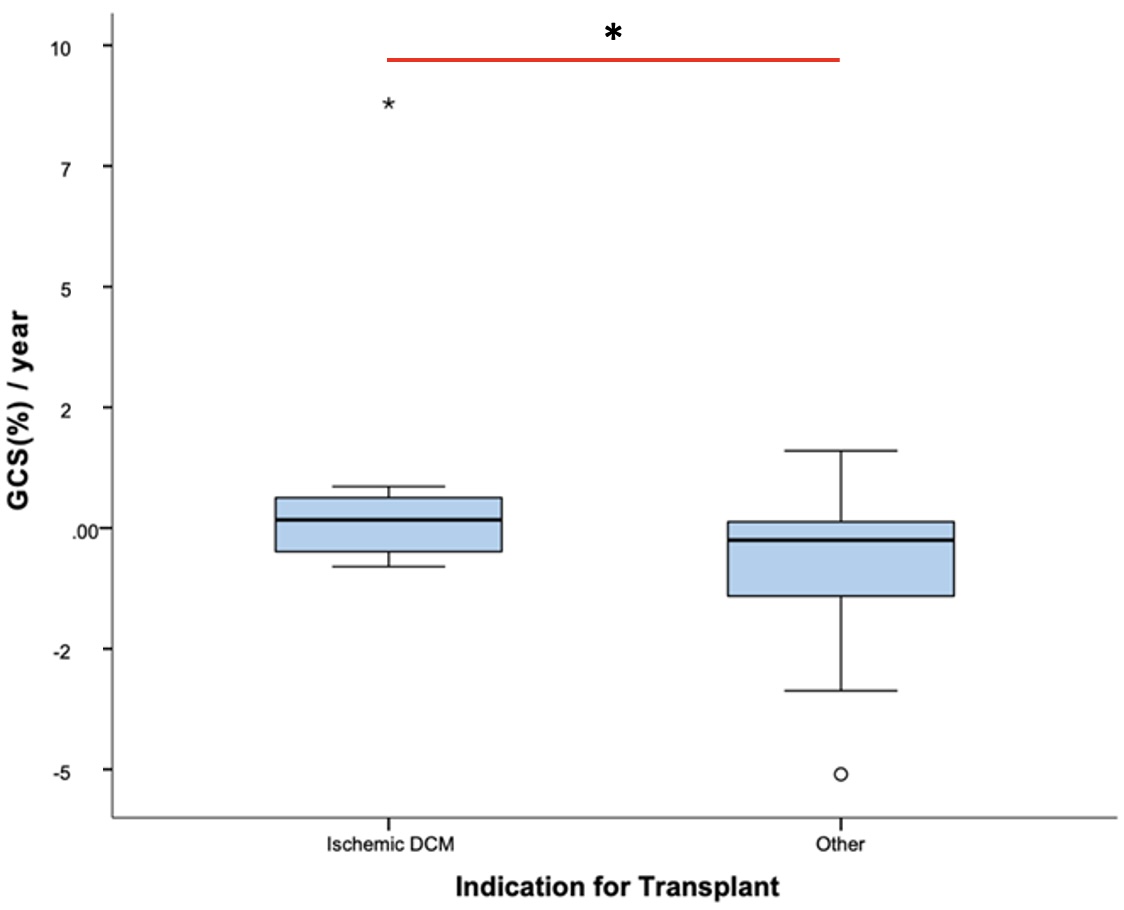
* = significance at level of p<0.05
Figure 3: Box plot depicting the change in GCS (%) per year in HTx patients split into two groups based on indication for transplant (ischemic DCM and non-ischemic (Other)).