1810
Myocardial Microstructural Characterization in Patients with Hypertrophic Cardiomyopathy by In Vivo Cardiac Diffusion Tensor Imaging1Fuwai Hospital, National Center for Cardiovascular Diseases, State Key Laboratory of Cardiovascular, Beijing, China, 2Clinical & Technical Support, Philips Healthcare (Beijing), China, Beijing, China
Synopsis
Keywords: Myocardium, Diffusion Tensor Imaging
Motivation: The non-invasive imaging evaluation of myocyte disarray in hypertrophic cardiomyopathy (HCM) is still challenging.
Goal(s): We aimed to explore the myocardial microstructural characteristics of HCM by in-vivo cardiac diffusion tensor imaging (cDTI).
Approach: We prospectively enrolled thirty-five HCM patients and fifteen healthy controls for cDTI at 3.0T scanner.
Results: Myocardial disarray and abnormal microstructural dynamics of HCM can be characterized by in vivo cDTI. Moreover, cDTI allows early identification of myocardial microstructural changes, even before cardiovascular magnetic resonance (CMR) signs of fibrosis and hypertrophy.
Impact: Our findings shed light on the potential of cDTI for the early detection of myocyte disarray, further improving the value of CMR in the non-invasive myocardial tissue characterization of HCM.
Introduction
Myocardial disarray is an important histological feature of hypertrophic cardiomyopathy (HCM), which may serve as the substrate of ventricular arrhythmias and myocardial dysfunction1,2. As a robust non-invasive imaging modality with unique ability in tissue characterization, cardiac magnetic resonance (CMR) plays an increasing important role in HCM, especially for the detection of fibrosis3. Nevertheless, challenges still remain in the assessment of myocardial disarray4. By measuring the magnitudes and directions of intramyocardial water diffusion, the emerging cardiac diffusion tensor imaging (cDTI) provides possibility to the non-invasive evaluation of myocardial microstructural characteristics5-7. Currently, there is still a lack of studies on in-vivo cDTI in human HCM and the ability of cDTI in the early assessment of myocardial microstructural changes is still not clear. Accordingly, this study aims to explore the diffusion characteristics of HCM by in-vivo cDTI, and to further determine whether cDTI could identify abnormal myocardium beyond regular CMR findings.Methods
Thirty-five HCM patients and fifteen healthy controls were prospectively enrolled for CMR imaging in 3.0T scanner (Ingenia, Philips Healthcare, Best, The Netherlands), equipped with 32 channel anterior and posterior array coils. Imaging protocol for HCM patients consisted of multiple- slice short axis cine imaging using a balanced Steady-State-Free-Precession (bSSFP) sequence, late gadolinium enhancement (LGE), T1 mapping using a Modified Look Locker Inversion (MOLLI) recovery sequence (native 5(3)3 and post-contrast 4(1)3(1)2) before and after enhancement and cDTI at a single mid-ventricular short-axis slice at the diastolic pause. cDTI data were obtained using an electrocardiography-triggered single-shot spin-echo echoplanar imaging (EPI) sequence with asymmetric bipolar diffusion waveforms for second-order motion-compensated and diaphragm navigator gating for respiratory compensation8. Radio-frequency (RF) shimming was used adaptively to reduce the B1 inhomogeneity. Post-processing of all regular CMR images were conducted using offline commercial software (cvi42 version 5.12.4, Circle Cardiovascular Imaging, Calgary, Alberta, Canada). Diffusion tensor analysis was performed using a custom-build software written in house using MATLAB (Mathworks, MA, USA). For segmental analysis, all the CMR images including cine, LGE, native T1 maps, ECV maps and cDTI maps of mid-ventricular slice were divided into six American Heart Association (AHA) segments for analysis using the anterior interventricular insertion point as reference. According to the presence of LGE, we divided all the segments into LGE positive (LGE+) and LGE negative (LGE-) group. Then LGE- segments were further divided into segments with hypertrophy but no LGE (H+LGE-) and segments with no hypertrophy or LGE (H-LGE-), in which hypertrophy were defined as segmental averaged thickness reaching 12 mm or larger9. The differences in CMR parameters between patients and controls or between different segmental categories, and the associations between T1 mapping and cDTI parameters were assessed using SPSS (Version 26.0).Results
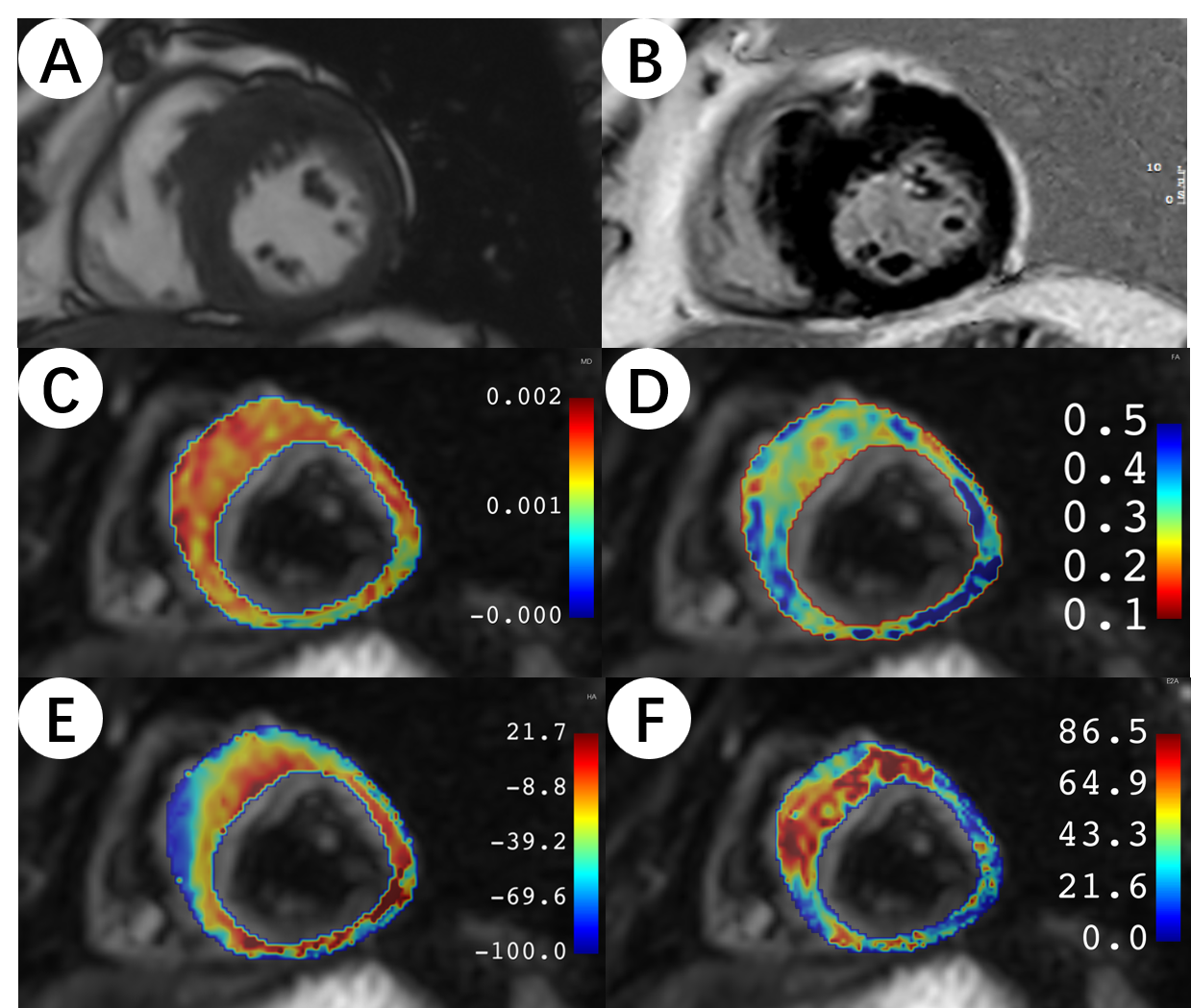
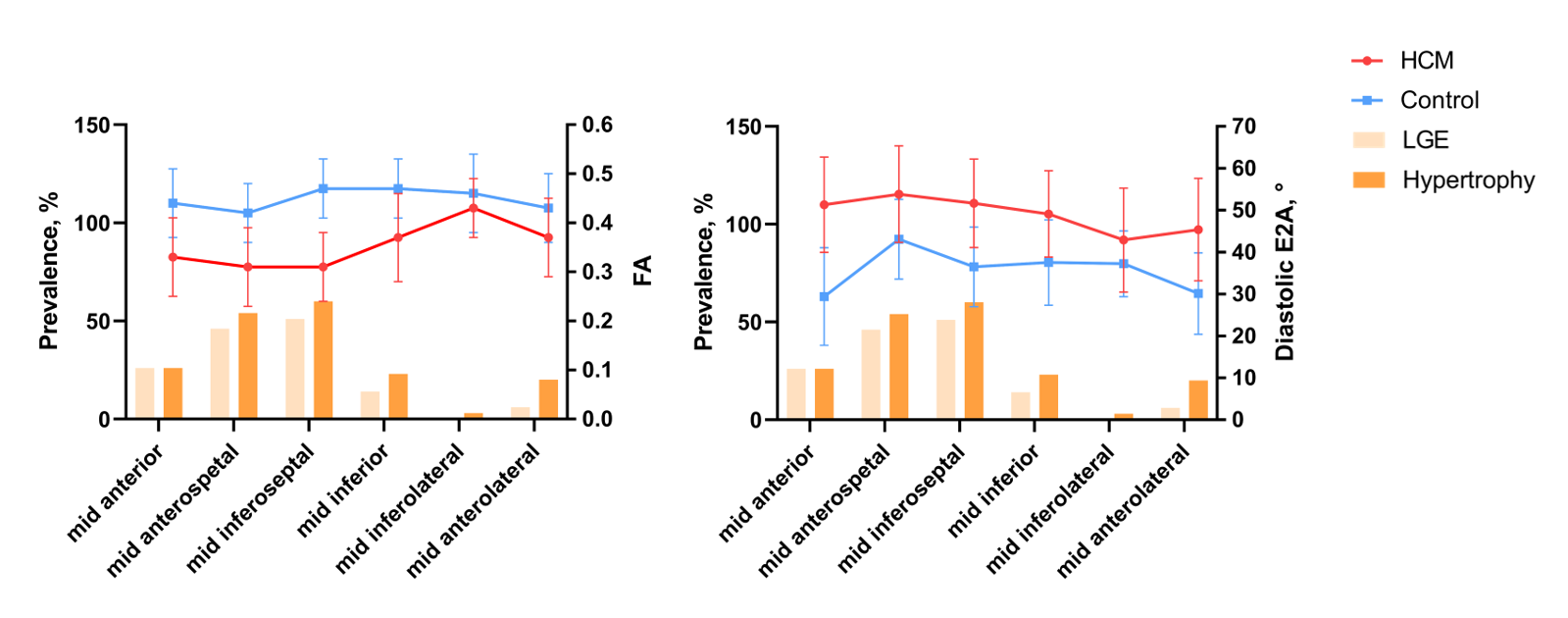
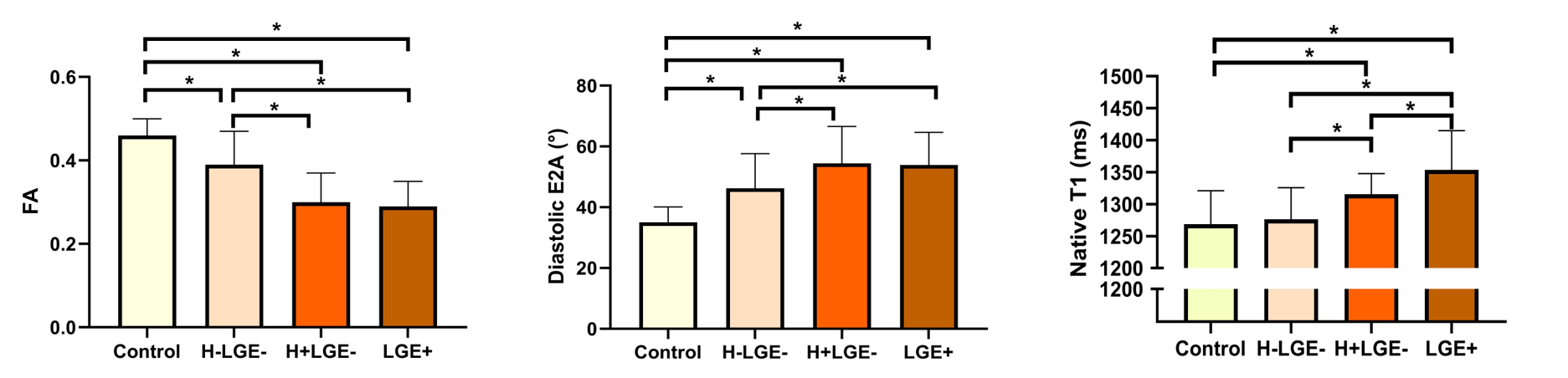
cDTI data were successfully acquired in all cases (Fig. 1). Compared with controls, HCM patients showed significantly reduced global FA (0.33±0.05 vs. 0.46±0.04, p<0.001) and increased global E2A in diastole (48.85±7.13 vs. 35.05±5.06, p<0.001). As for segmental analysis, average segmental FA in HCM was significantly reduced in the segments with higher LGE prevalence and greater hypertrophy extent (anteroseptum or inferoseptum) compared to the inferolateral segment, while diastolic E2A was significantly increased (all p<0.05) (Fig. 2). Among different segmental categories, segments with hypertrophy or LGE had significantly reduced FA, increased diastolic E2A and native T1 than controls (all p<0.001). Most importantly, the FA and diastolic E2A of H-LGE- segments in HCM were also significantly abnormal than controls (FA: 0.39±0.08 vs. 0.45±0.07; E2A: 46.23±11.43 vs. 35.69±10.52, both p<0.001), while native T1 was not (1276.40±49.26 ms vs. 1268.77±52.08 ms, p=0.21) (Fig. 3). Correlation analysis indicate that both FA (r=-0.43, p<0.001) and diastolic E2A (r=0.31, p<0.001) were significantly associated with native T1 values.Conclusion
Myocardial disarray and abnormal microstructural dynamics of HCM can be characterized by in vivo cDTI. Reduced FA and abnormal diastolic E2A could be observed in HCM even if without significant myocardial hypertrophy or LGE, suggesting the potential of cDTI to improve the value of CMR in tissue characterization of HCM.Summary of Main Findings
In hypertrophic cardiomyopathy, myocardial microstructural abnormalities could be detected by in-vivo cardiac diffusion tensor imaging no matter the presence of hypertrophy or fibrosis, providing novel insights to the non-invasive myocardial tissue characterization.Acknowledgements
This study was co-funded by Key Project of National Natural Science Foundation of China (No. 81930044) and National Key R&D Program of China (No. 2021YFF0501400 and 2021YFF0501404).References
1. Cui H, Schaff HV, Lentz Carvalho J, et al. Myocardial Histopathology in Patients With Obstructive Hypertrophic Cardiomyopathy. Journal of the American College of Cardiology. 2021;77:2159-2170.2. Varnava AM, Elliott PM, Mahon N, et al. Relation between myocyte disarray and outcome in hypertrophic cardiomyopathy. Am J Cardiol. 2001;88:275-279.
3. Lu M, Zhu L, Prasad SK, et al. Magnetic resonance imaging mimicking pathology detects myocardial fibrosis: a door to hope for improving the whole course management. Sci Bull (Beijing). 2023;68:864-867.
4. McGill L-A, Ismail TF, Nielles-Vallespin S, et al. Reproducibility of in-vivo diffusion tensor cardiovascular magnetic resonance in hypertrophic cardiomyopathy. Journal of cardiovascular magnetic resonance : official journal of the Society for Cardiovascular Magnetic Resonance. 2012;14:86.
5. Pashakhanloo F, Herzka DA, Mori S, et al. Submillimeter diffusion tensor imaging and late gadolinium enhancement cardiovascular magnetic resonance of chronic myocardial infarction. Journal of cardiovascular magnetic resonance : official journal of the Society for Cardiovascular Magnetic Resonance. 2017;19:9.
6. Ariga R, Tunnicliffe EM, Manohar SG, et al. Identification of Myocardial Disarray in Patients With Hypertrophic Cardiomyopathy and Ventricular Arrhythmias. Journal of the American College of Cardiology. 2019;73:2493-2502.
7. Khalique Z, Ferreira PF, Scott AD, et al. Diffusion Tensor Cardiovascular Magnetic Resonance Imaging: A Clinical Perspective. JACC Cardiovascular imaging. 2020;13:1235-1255.
8. Stoeck CT, von Deuster C, Genet M, et al. Second-order motion-compensated spin echo diffusion tensor imaging of the human heart. Magnetic Resonance In Medicine. 2016;75:1669-1676.
9. Wang L, Wang Y, Wang J, et al. Myocardial Activity at 18F-FAPI PET/CT and Risk for Sudden Cardiac Death in Hypertrophic Cardiomyopathy. Radiology. 2023;306:e221052.
Figures