1806
Diffusion Tensor Phenomapping of Local Microenvironments in the Pressure Overloaded Human Heart1Cardiovascular Research Center, Mass General Hospital, Boston, MA, United States, 2A.A Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Charlestown, MA, United States, 3Institute of Medical Physics and Radiation Protection, TH Mittelhessen University of Applied Sciences, Geissen, Germany, 4Cardiovascular Innovation Research Center, Heart, Vascular, and Thoracic Institute, Cleveland Clinic, Cleveland, OH, United States, 5Health Sciences and Technology Program, Harvard - Massachusetts Institute of Technology, Cambridge, MA, United States
Synopsis
Keywords: Myocardium, Radiomics
Motivation: DTI data in the heart are currently averaged to yield per-patient values that cannot detect local variations in the microstructural microenvironment.
Goal(s): We aimed to develop a voxel-based phenomapping approach to cluster the voxels in the myocardium into distinct groups based on their microstructural properties. We then used the approach to compare subjects with aortic stenosis (AS) to age-matched controls (CTL).
Approach: A population matrix of voxels was created using z-score normalization and evaluated with k-means clustering (k=4).
Results: 4 distinct clusters of voxels were present, each with different microstructural properties. No significant differences were seen between the AS and CTL subjects.
Impact: An approach to perform voxel-based phenomapping of DTI data in the heart was developed and used to classify the voxels in the myocardium into distinct microstructural clusters.
Introduction
Diffusion tensor imaging (DTI) enables non-invasive characterization of the heart’s microstructure. However, analysis of the data is currently performed by averaging parameters from all voxels into a single patient-based value. Here we introduce a voxel-wise approach, analogous to single cell RNASeq of tumors, that allows distinct microstructural environments in the myocardium to be detected.Methods
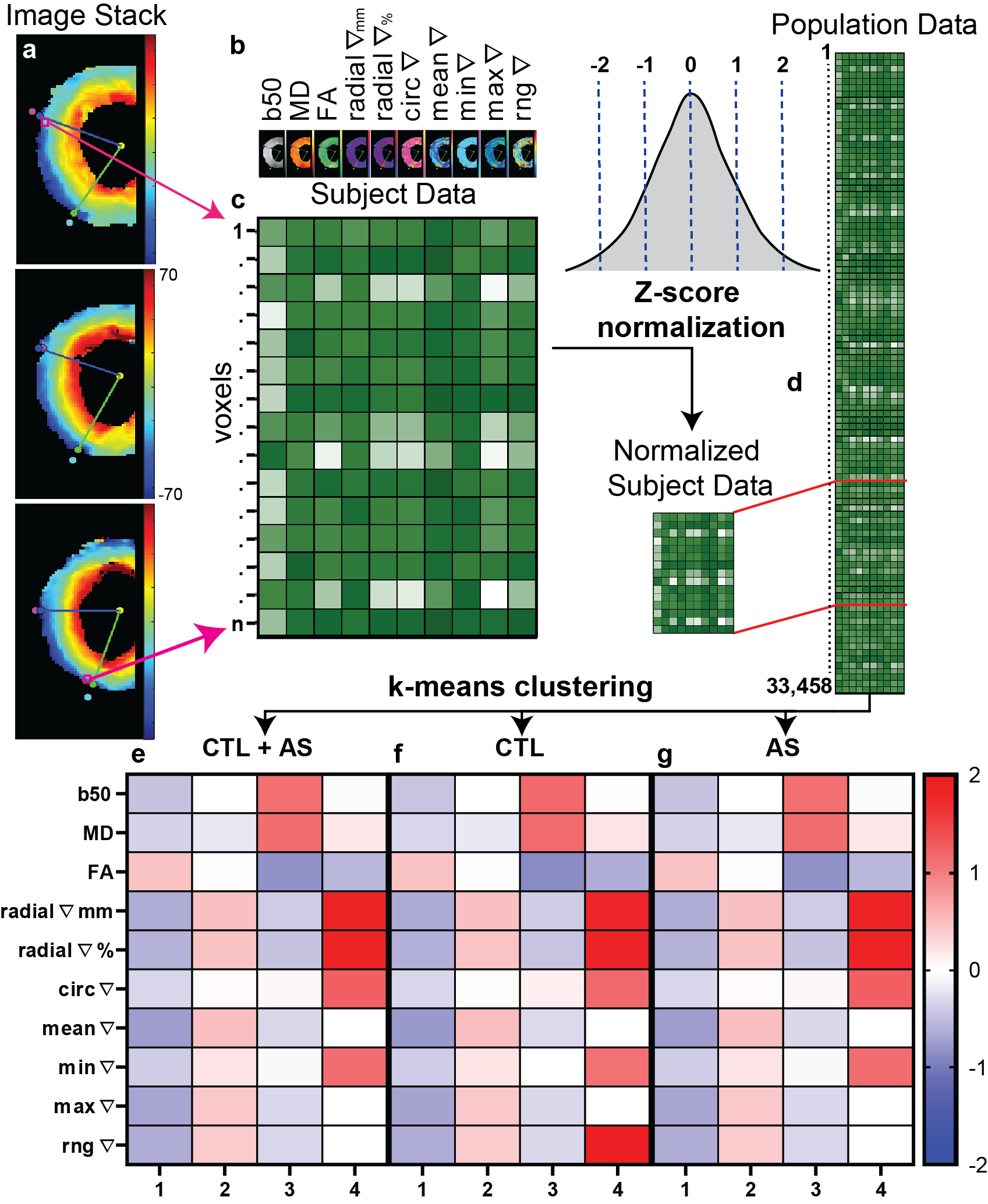
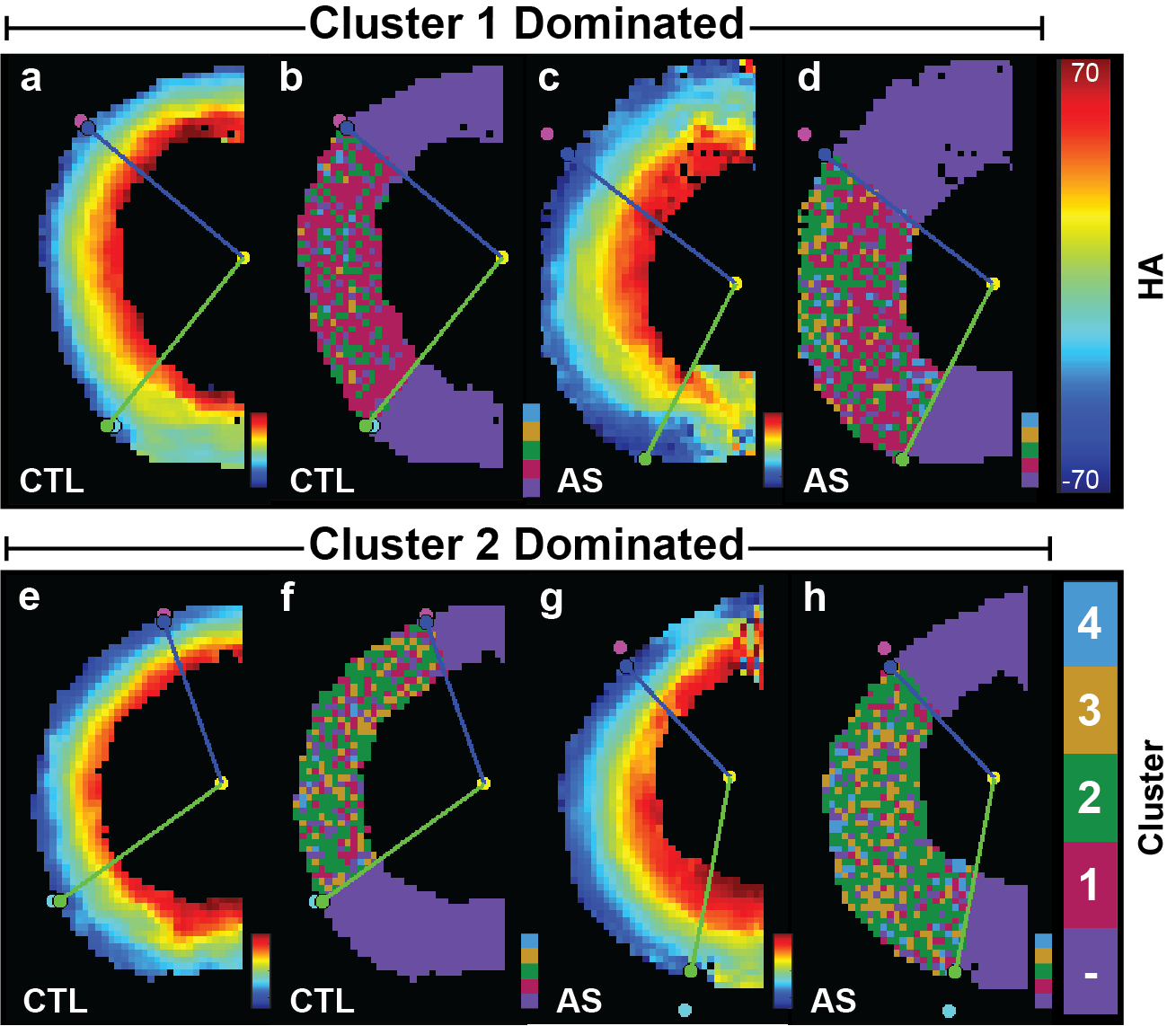
Subjects with severe AS (n=10) and age matched controls (CTL, n=10) underwent scanning on 3T scanner with 80mT/m gradients (Primsa, Siemens) using a custom-built 64-element cardiac array. This produced a stack of high-resolution (0.85x0.85mm in-plane) helix angle (HA) maps from which local HA gradients could be obtained. A series of 3-5 mid-ventricular slices (Fig. 1A) were selected in each subject for analysis. Local HA gradients were calculated using Matlab (Natick, MA) by measuring changes in HA between adjacent in-plane voxels. 10 coregistered parameter maps were derived for each voxel (Fig. 1B) and normalized via a Z-score (Fig. 1C). The normalized subject data was then combined to generate a population matrix on which k-means (k=4) clustering using Matlab was performed (Fig. 1D). Cluster maps were generated, where each voxel was classified by the microstructural cluster it fell into (Fig. 2).Results
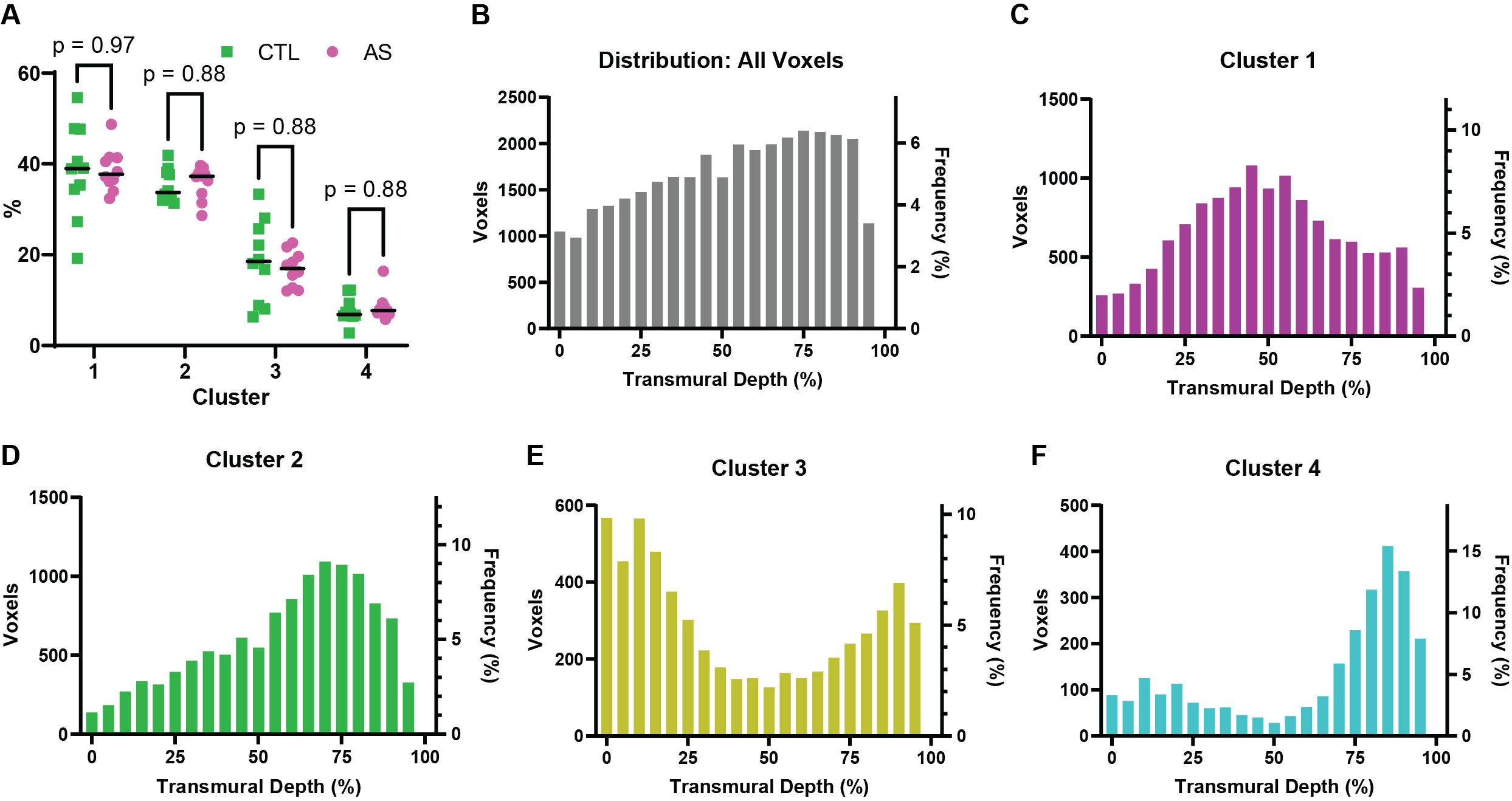
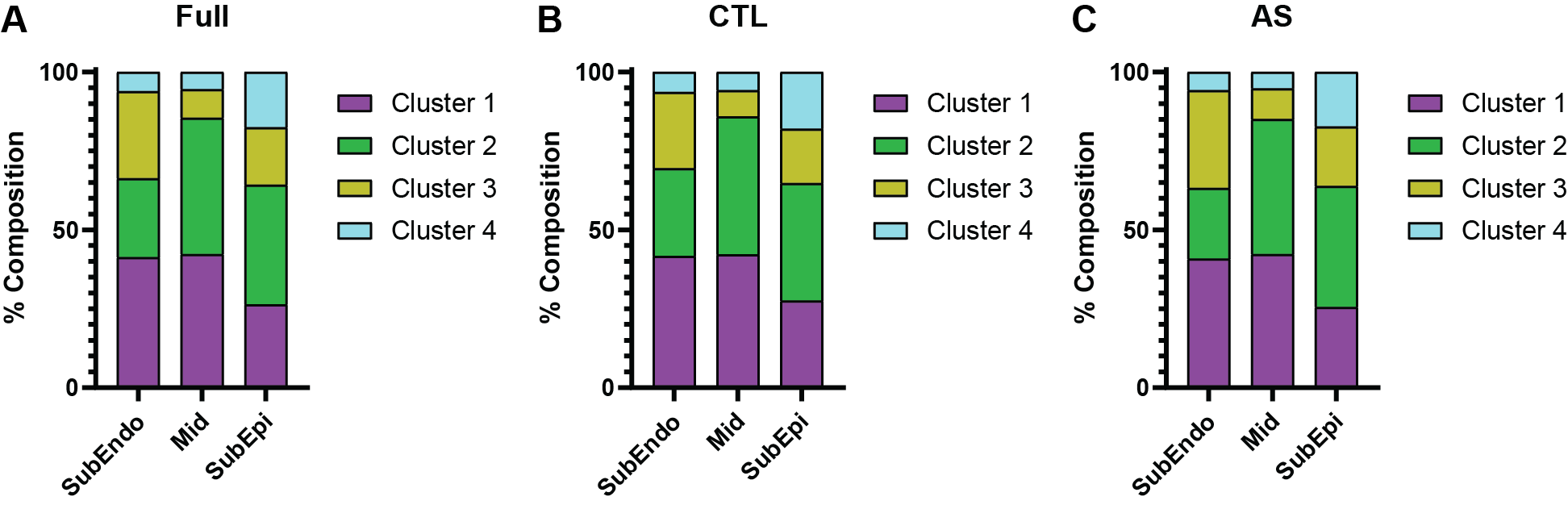
4 different voxel clusters were identified (Fig 1E-F, Fig.2). The first cluster contained highly ordered voxels, with below average HA gradients, low MD and high FA. This was the most common cluster (~39%, Fig. 3A) and was most concentrated in the midmyocardium (Fig. 3C). The second most common cluster (~36%, Fig. 3A) contained voxels with above-average gradients and average MD and FA. These voxels showed a small preference for the subepicardium (Fig. 3D). Cluster 3 (~17%, Fig. 3A) consisted of voxels with lower HA gradients but also lower FA and higher MD. These voxels were most concentrated in the sunendocardium and subepicardium (Fig. 3E). Cluster 4 (~8%, Fig. 3A) contained voxels with high radial and circumferential gradients, lower FA, and slightly elevated MD. These voxels were most frequently found in the subepicardium (Fig. 3F). The relative contribution of voxels from each cluster across the layers of the heart is shown in Figure 4. In the subendocardium voxels, cluster 1 were the most prominent (41%) followed by similar proportions from cluster 2 (25%) and cluster 3 (28%). In the midmyocardium, the contributions of cluster 1 (42%) and cluster 2 (43%) were similar. In the subepicardium, the proportion of voxels from cluster 1 decreased (26%), while that from cluster 4 increased (18%). No significant differences in the overall breakdown of the clusters (Fig 3A) their transmural distribution (Fig 3B-F) or their prevalence in the various layers of the myocardium (Fig 4B&C) were seen between the aortic stenosis and control subjects.Discussion
Voxel-based phenomapping allows local variations in the microstructural microenvironment in the heart to be detected using a formalism analogous to single cell RNA sequencing for categorizing cells within a tissue. The largest cluster (cluster 1) contained highly ordered voxels and was most concentrated in the midmyocardium (Fig. 3C). The voxels of cluster 3 were also highly ordered but contained higher MD values, suggesting they might represent mixed voxels with cardiomyocytes adjacent to blood vessels. The least ordered voxels of cluster 4 were present throughout the myocardium, but were most prevalent in the subepicardium. No significant differences in overall cluster composition (Fig 3) or regional fractional composition (Fig 4) were seen in the AS subjects vs. CTLs. This suggests that in well compensated AS, the structural microenvironment in the myocardium maintains its architectural integrity.Conclusions
A formalism to perform voxel-based phenomapping was developed and applied in a cohort of patients with severe AS and age-matched controls. 4 clusters of voxels were identified in the myocardium and were similar in AS and CTLs. The proposed phenomapping approach provides a new formalism for the analysis of microstructure in the heart and could provide important new insights into the biology of the myocardium.Acknowledgements
No acknowledgement found.References
No reference found.Figures