1805
Microstructural assessment of myocardial non-compaction by cardiac diffusion tensor imaging1Institute for Biomedical Engineering, University and ETH Zurich, Zurich, Switzerland, 2Department of Cardiology, University Heart Center, University Hospital Zurich, Zurich, Switzerland, 3Diagnostic and Interventional Radiology, University Hospital Zurich, Zurich, Switzerland, 4Center for Preclinical Development, University of Zurich and University Hospital Zurich, Zurich, Switzerland
Synopsis
Keywords: Myocardium, Cardiomyopathy, non-compaction , cardiac diffusion tensor imaging, cDTI
Motivation: Left ventricular non-compaction cardiomyopathy (LVNC) is characterized by the presence of excessive trabeculation in the left ventricle.
Goal(s): To characterize the myocardial microstructure of LVNC patients in comparison to healthy controls using cardiac Diffusion Tensor Imaging (cDTI).
Approach: Second order motion compensated spin echo cardiac DTI was acquired in six LVNC patients and six healthy controls. Myocyte aggregate orientation is characterized by helix angle and relative percentage of right handed helical orientated myocytes.
Results: In the compacted myocardium, LVNC patients exhibited lower endocardial helix angles and a loss of the endocardial right handed helix when compared to controls.
Impact: Our findings indicate that in LVNC patients, a portion of the endocardial helix is dissolved into the non-compacted myocardium, which may impair optimal myocardial contraction in the affected segments as well as apical rotation as observed in LVNC patients.
Introduction
Left ventricular non-compaction cardiomyopathy (LVNC) is a rare heart condition characterized by the presence of excessive trabeculation in the left ventricle (LV). While early investigations of the disease reported a high mortality and morbidity from heart failure, thrombo-embolic events and ventricular arrhythmias, current evidence shows that the finding of excessive tabeculation is not associated with impaired prognosis in otherwise healthy subjects and does not alter prognosis in patients with dilated or hypertrophic cardiomyopathy. Therefore, the status of LVNC as a distinct cardiomyopathy is currently debated [1]. However, the characteristic morphology of LVNC and consistent findings of reduced strain and apical rotation imply pathological myocardial alterations [2]. Cardiac diffusion tensor imaging (cDTI) enables the assessment of cardiac microstructure and myocyte aggregate orientation [3]. The objective of the present work was to investigate the myocardial microstructure of LVNC patients in comparison to healthy controls using cDTI.Methods
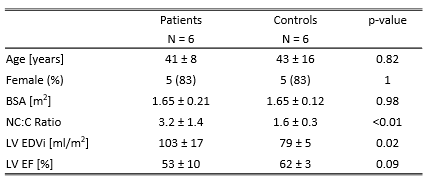
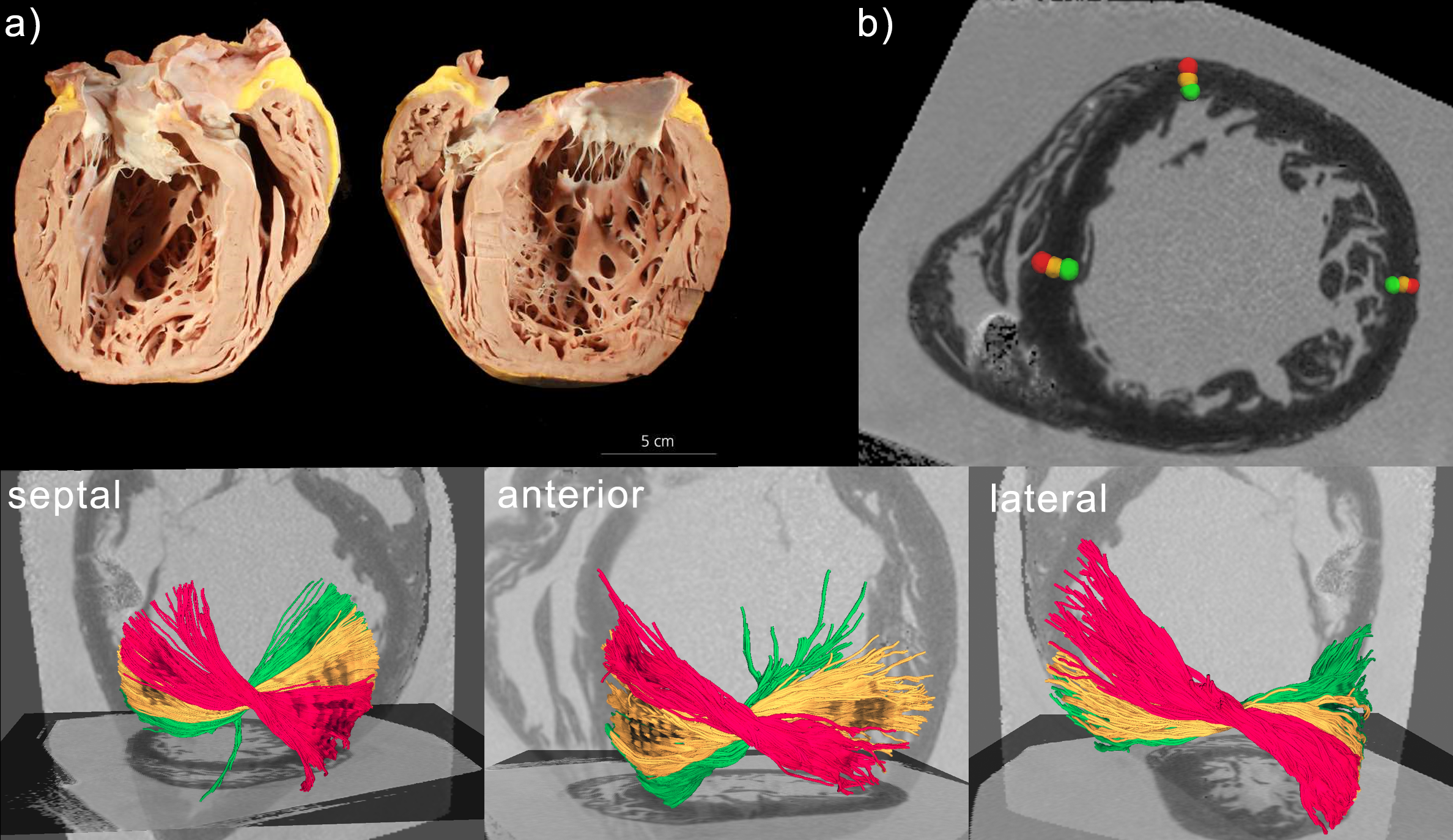
In this preliminary study we included six patients diagnosed with LVNC as well as six healthy controls. All study participants provided written informed consent and the protocol was approved by the local ethics committee. CMR was performed on a clinical 1.5T system (Achieva, Philips Healthcare, Best, The Netherlands) with a high-performance gradient system (80mT/m maximum gradient strength, 100mT/m/ms slew rate) and included functional cine imaging as well as cDTI. Imaging parameters are provided in Table 1. In brief: functional imaging was performed by retrospectively ECG gated, balance SSFP cine imaging in short axis orientation covering the entire heart; cDTI was performed using a second order motion compensated spine echo sequence [3] with water selective spectral spatial excitation, a reduced FOV [4], respiratory navigator based slice tracking and ECG triggering to 65% end systole. Cine data was evaluated using clinical evaluation software (ISP, Philips Healthcare, Best, The Netherlands) and LV volumes and function are reported. cDTI data was first registered [5] and consequently complex averaged [6]. Diffusion Tensors were computed using an in-house software tool (Matlab, Mathworks, Natick, MA, USA) and MD, FA, Helix angle (HA) maps as well as the relative percentage of right-handed helical alignment (HA>30°) of myocyte aggregates are reported.One ex-vivo heart was imaged post explanation from an additional heart transplant patient. The sample was formalin fixated (4% buffered formalin solution) and imaged using a spin echo sequence with 3D segmented echo planar imaging readout and conventional Stejskal-Tanner diffusion encoding. Imaging was performed on the same scanner as in-vivo imaging. Fibre tracking was performed using DSI studio.
Results
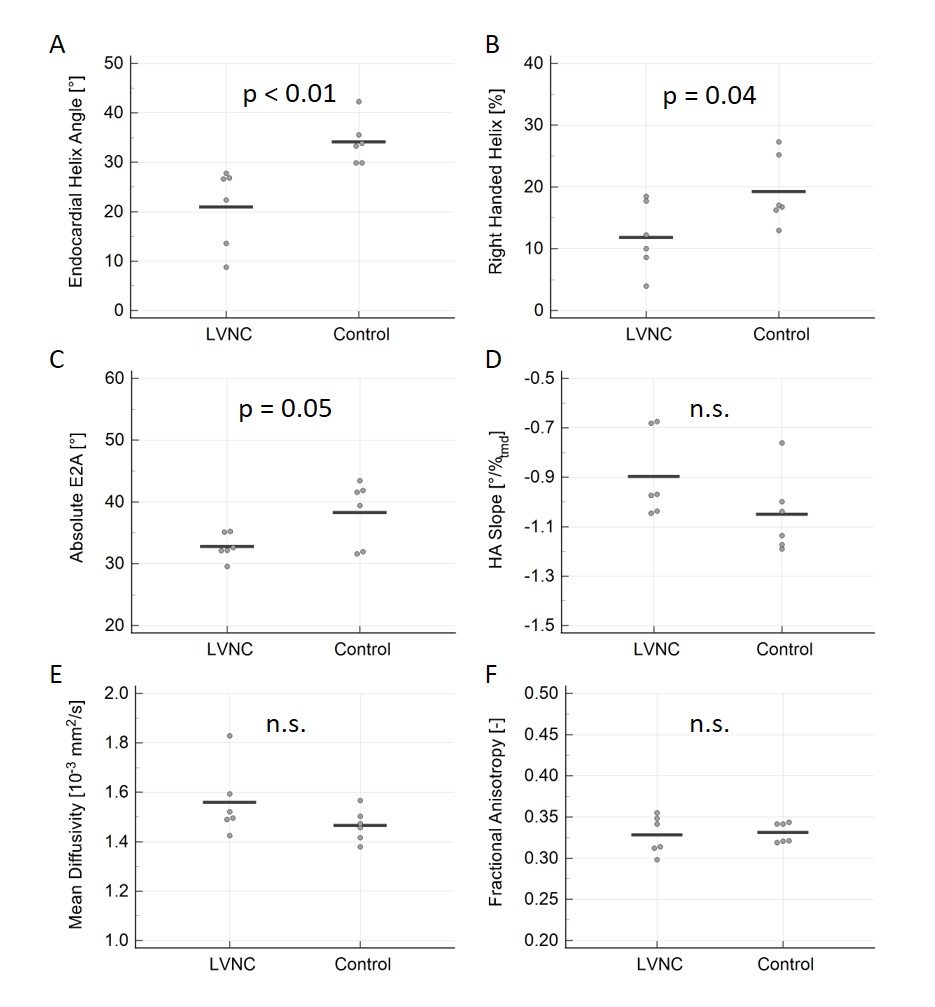
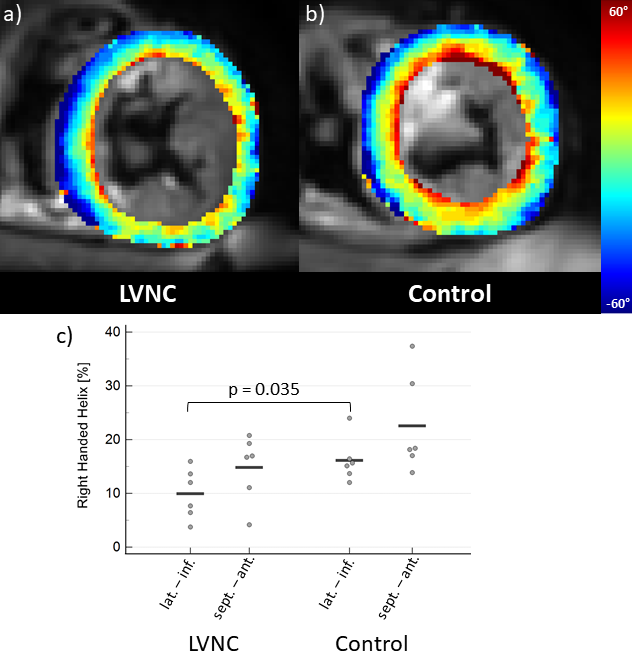
In vivo:Table 2 shows the baseline characteristics of the LVNC patient and control groups. LVNC patients had larger LVs, a higher non-compacted to compacted tissue (NC:C) ratio and a trend towards lower LVEF. Two LVNC patients had reduced LVEF (<50%). In the compacted myocardium, LVNC patients exhibited lower endocardial helix angles (p<0.01) and a loss of the endocardial right handed helix (p=0.04) when compared to controls. The absolute E2A sheet angle was lower in LVNC patients (p=0.05) while MD, FA and the HA slope where not statistically significant different between both groups (Figure 1). Figure 2 a) and b) shows representative HA maps of an LVNC patient and a control subject. When viewed on a segmental level, the loss of the endocardial right-handed helix was most prominent in the lateral and inferior segments, which are known to be most affected by LVNC (Figure 2 c).
Ex vivo:
Figure 3 shows the fiber tracking results of the post-transplant ex-vivo heart as well as the degree of non-compaction in the pathology image. The entire lateral wall presents endocardial non-compacted myocardium. Fiber tracking at epi, meso and endocardium of the compacted myocardium in the remote (septal), borderline (anterior) and affected (lateral) area reveals the lack of right handed endocardial (green) helical structure in the affected region.
Conclusion
Our findings indicate that in LVNC patients, a portion of the endocardial helix is dissolved into the non-compacted myocardium, which may impair optimal myocardial contraction in the affected segments. In conjunction with the ex vivo findings, we hypothesise that the thinned, compacted myocardium in the lateral and inferior segments of LVNC patients contains only the midmyocardial and epicardial helical structures of a normal myocardium. This observation could explain the lack of apical rotation observed in LVNC patients. The finding of reduced absolute E2A has previously been described in patients with dilated cardiomyopathy (DCM), which appears coherent given the known overlap between DCM and LVNC cohorts. The small number of patients is the major limitation of this ongoing study.Acknowledgements
No acknowledgement found.References
[1] S. E. Petersen u. a., „Excessive Trabeculation of the Left Ventricle: JACC: Cardiovascular Imaging Expert Panel Paper“, JACC Cardiovasc. Imaging, Bd. 16, Nr. 3, S. 408–425, März 2023, doi: 10.1016/j.jcmg.2022.12.026.
[2] M. Gastl u. a., „Determinants of myocardial function characterized by CMR-derived strain parameters in left ventricular non-compaction cardiomyopathy“, Sci. Rep., Bd. 9, Nr. 1, S. 15882, Nov. 2019, doi: 10.1038/s41598-019-52161-1.
[3] C. T. Stoeck, C. Von Deuster, M. GeneT, D. Atkinson, und S. Kozerke, „Second-order motion-compensated spin echo diffusion tensor imaging of the human heart“, Magn. Reson. Med., Bd. 75, Nr. 4, 2016, doi: 10.1002/mrm.25784.
[4] B. J. Wilm, J. Svensson, a Henning, K. P. Pruessmann, P. Boesiger, und S. S. Kollias, „Reduced field-of-view MRI using outer volume suppression for spinal cord diffusion imaging.“, Magn. Reson. Med. Off. J. Soc. Magn. Reson. Med. Soc. Magn. Reson. Med., Bd. 57, Nr. 3, S. 625–30, März 2007, doi: 10.1002/mrm.21167.
[5] V. Vishnevskiy, T. Gass, G. Szekely, C. Tanner, und O. Goksel, „Isotropic Total Variation Regularization of Displacements in Parametric Image Registration“, IEEE Trans. Med. Imaging, Bd. 0062, Nr. c, S. 1–1, 2016, doi: 10.1109/TMI.2016.2610583.
[6] A. D. Scott, S. Nielles-Vallespin, P. F. Ferreira, L. A. McGill, D. J. Pennell, und D. N. Firmin, „The effects of noise in cardiac diffusion tensor imaging and the benefits of averaging complex data“, NMR Biomed., Bd. 29, Nr. 5, S. 588–599, 2016, doi: 10.1002/nbm.3500.
Figures