1802
Biventricular Remodeling Predicts Adverse Outcomes in Long-Term Follow-up of Chronic Thromboembolic Pulmonary Hypertension: A CMR Study1Department of Radiology, Beijing Chaoyang Hospital, Capital Medical University, Beijing, China, Beijing, China
Synopsis
Keywords: Myocardium, Cardiovascular, Chronic thromboembolic pulmonary hypertension; cardiovascular magnetic resonance; prognosis; ventricular remodeling
Motivation: While cardiovascular magnetic resonance (CMR) is a well-established tool for assessing heart remodeling and predicting outcomes, its application in Chronic thromboembolic pulmonary hypertension (CTEPH) has received limited attention.
Goal(s): This study investigated whether biventricular remodeling derived form CMR could predict adverse clinical outcomes during the long-term follow-up of CTEPH patients.
Approach: Establish a CMR-only model and compare its predictive value with the model that combines clinical data and invasive RHC.
Results: CMR-derived biventricular remodeling have prognostic value in long-term follow-up CTEPH. Risk assessment based on CMR alone is at least as effective as that of clinic combined RHC.
Impact: These findings contribute to the optimization of early patient care and timely intervention. it's advisable to add CMR parameters in the management score. And performing noninvasive CMR alone is sufficient, as it also demonstrates excellent predictive efficacy.
Introduction
Chronic thromboembolic pulmonary hypertension (CTEPH) is a prevalent and significant cause of pulmonary hypertension (PH)1, leading to cardiac remodeling, eventual functional failure, and death.2,3 While cardiovascular magnetic resonance (CMR) is an established prognostic tool for assessing cardiac remodeling and has been used for prognostic assessment in patients with pulmonary arterial hypertension (PAH)1,4–7, few studies have investigated its potential application in CTEPH.Methods
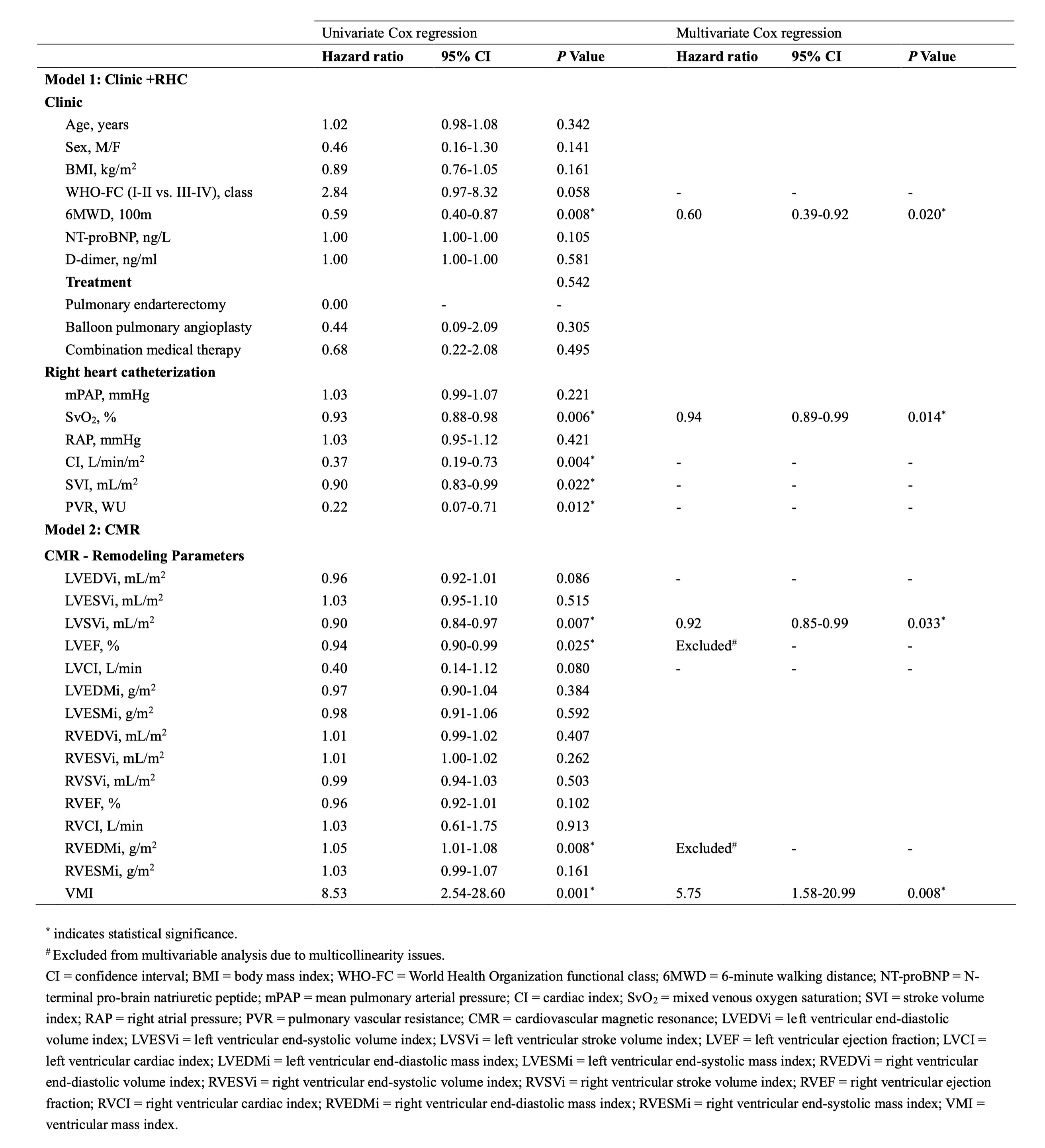
Sixty-five patients with CTEPH who underwent CMR and right heart catheterization (RHC) examination within 7 days were included in this study. The median follow-up time was 43 months (interquartile range: 39-54 months), and fifteen patients experienced adverse clinical outcomes (all-cause mortality or rehospitalization for worsening of World Health Organization functional class).CMR were performed on a 3.0 Tesla scanner (MAGNETOM Prisma, Siemens, Erlangen, Germany) with an 18-channel phased-array surface coil and with retrospective electrocardiogram gating steady-state free precession (SSFP). Standard long-axis 4-chamber and RV long-axis 2-chamber cine imaging were acquired using SSFP sequences. Furthermore, contiguous cine short-axis (SA) slices were obtained, covering both ventricles from the base to the apex. Biventricular volume and mass were determined by contouring endocardial and epicardial borders at end-systole and end-diastole semi-automatically from SA stacks using CVI42 (Version 5.8, Circle Cardiovascular Imaging). All volume and mass parameters were indexed to body surface area (BSA).Cox proportional hazard regression analyses were done to determine the best predictive Clinic combined RHC, and/or CMR model. Receiver operating characteristic (ROC) analyses were performed to determin the optimal cut-off values using the Youden index. Kaplan-Meier survival analyses stratified patients by cut-off values, with log-rank tests. For model comparing, AUC and AIC were used to compare predictive accuracy of each model.Results
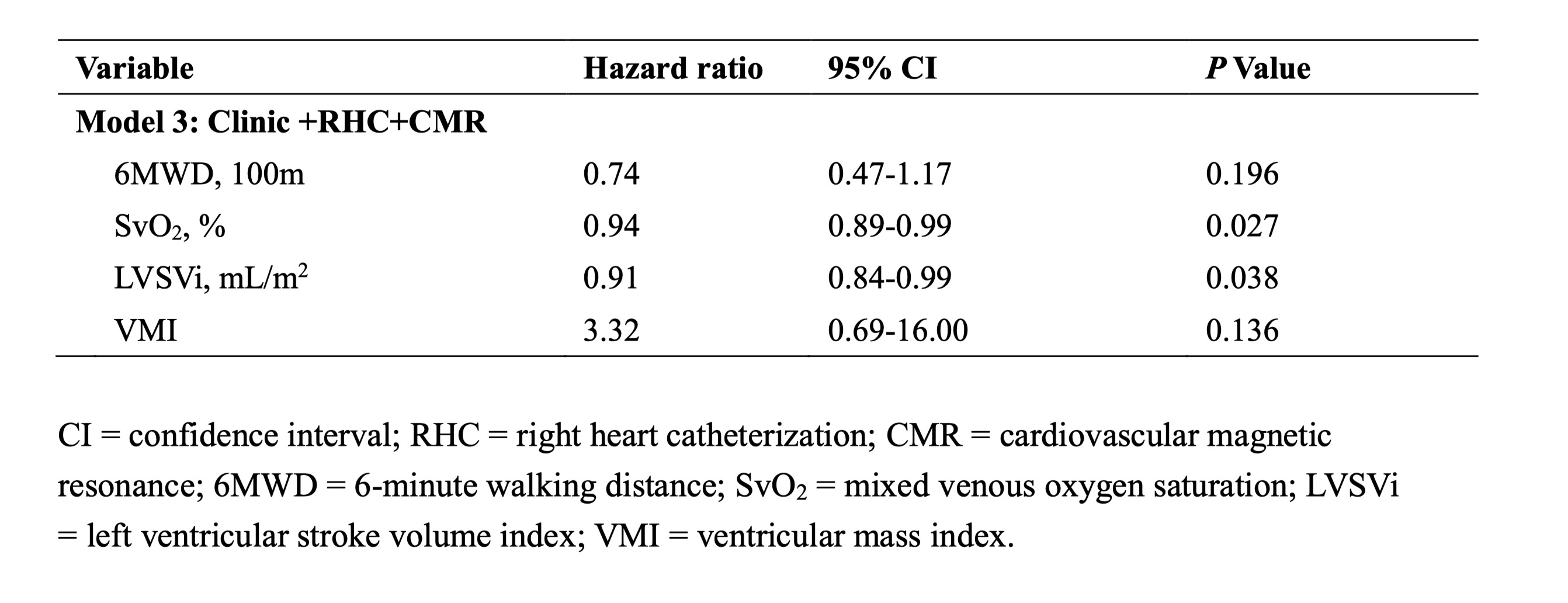
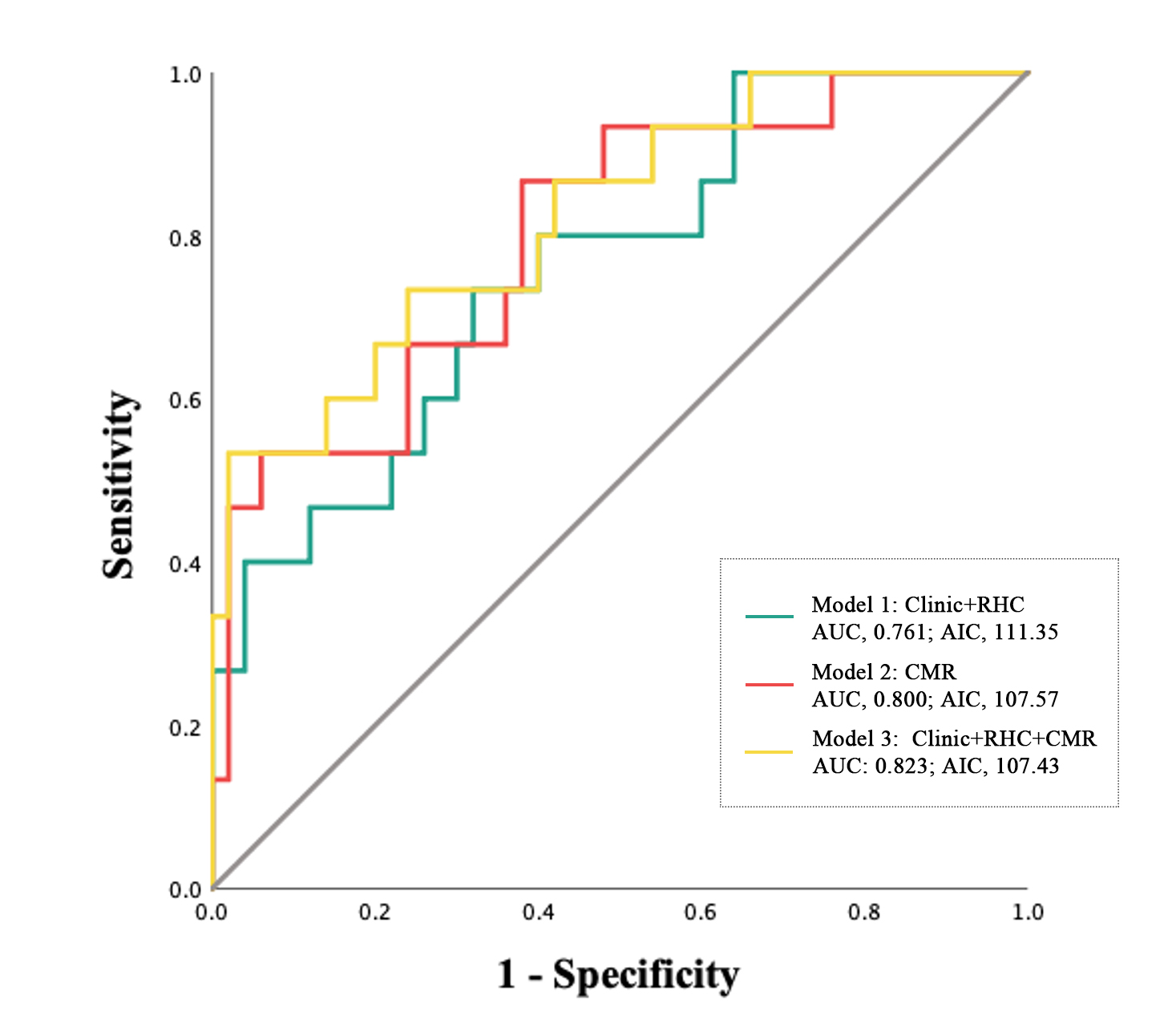
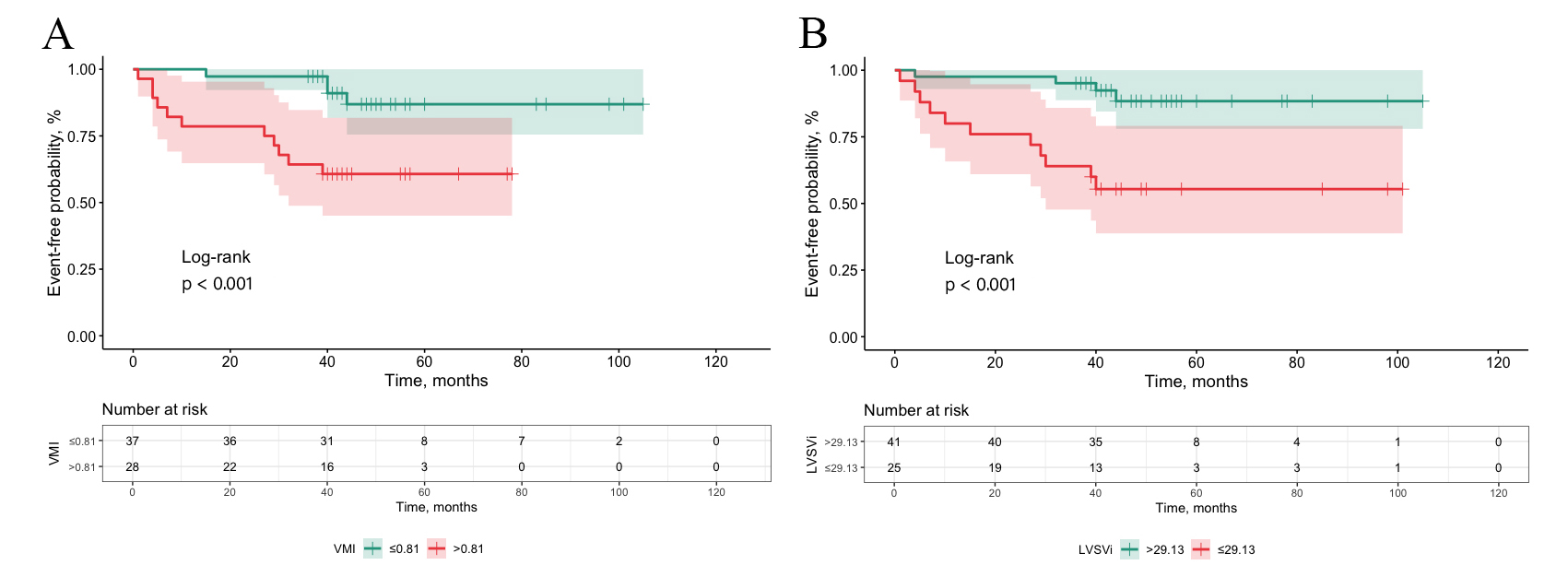
The multivariate Cox analysis showed that the ventricular mass index (VMI) (Hazard ratio [HR], 5.75; 95% confidence interval [CI], 1.58-20.99; P = 0.008) and left ventricular stroke volume index (LVSVi) (HR, 0.92; 95% CI, 0.85-0.99; P = 0.033) could predict adverse clinical outcomes in the CMR model. And, the optimal cut-off of VMI and LVSVi are 0.81 and 29.13 mL/m2, respectively.The CMR model (Area under the curve [AUC], 0.800; 95% CI, 0.67-0.93; Akaike information criterion [AIC], 107.57; sensitivity, 86.7%; specificity, 62.0%) has much value in predicting adverse events than the Clinic combined RHC model (AUC, 0.761; 95% CI, 0.63-0.90; AIC, 111.35; sensitivity, 73.3%; specificity, 68.0%). Finally, the predictive value improved when the parameters of both models (AUC, 0. 823; 95% CI, 0.70-0.95; AIC, 107.43; sensitivity, 53.3%; specificity, 98.0%).Discussion
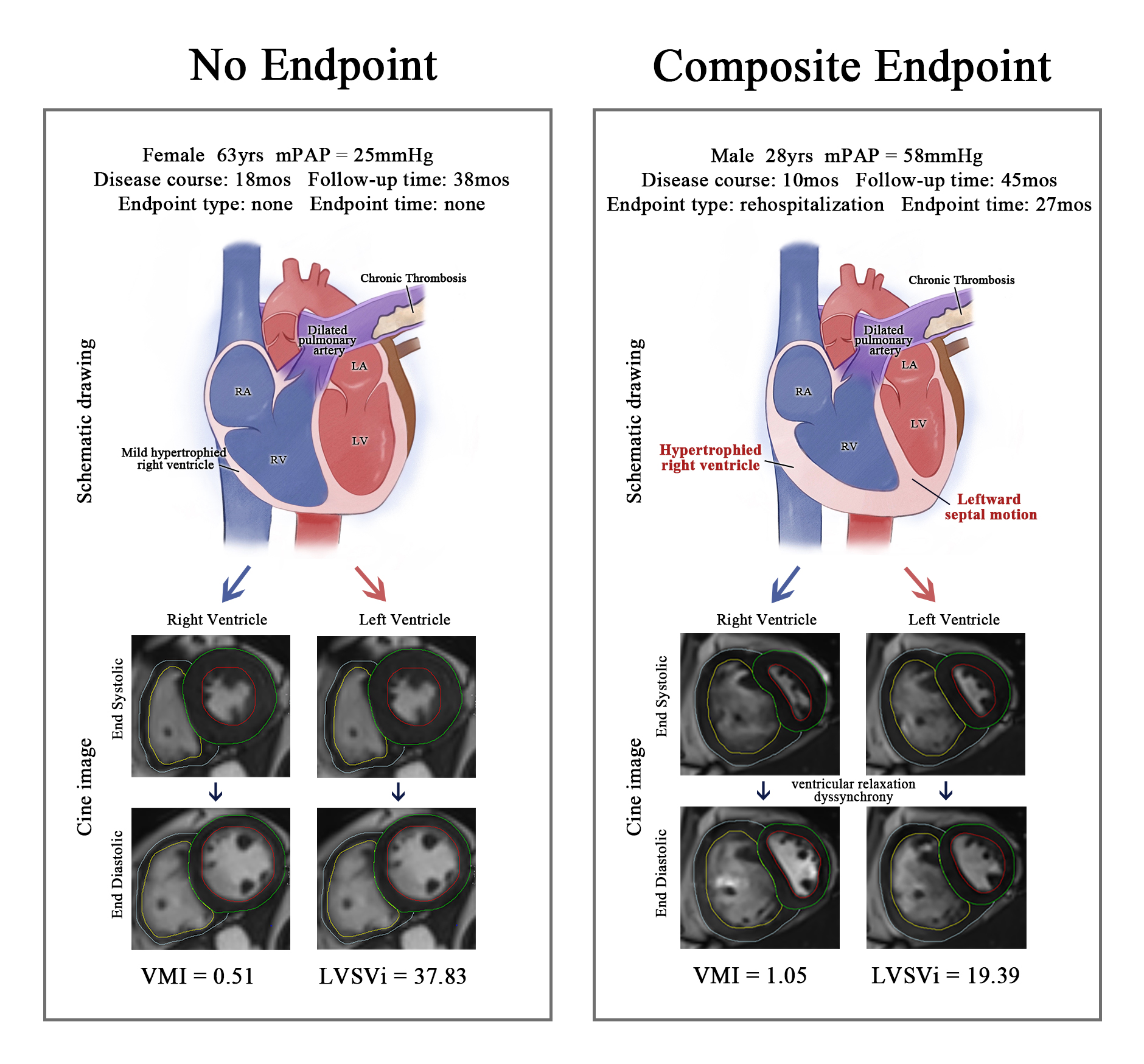
In CTEPH, the adaptability of both the right ventricle (RV) and left ventricle (LV) plays a significant role in determining functional capacity and survival.8 The Frank–Starling mechanism explains the initial RV hypertrophy in response to elevated pulmonary arterial pressure. As the disease progresses, the RV myocardium thins, and RV volume increases.9 Simultaneously, the LV undergoes adaptive atrophy of cardiomyocytes, emphasizing the growing importance of the LV in prognosis.10,11 CMR offers several advantages, such as superior imaging quality and reproducibility, making it an ideal choice for assessing biventricular remodeling in CTEPH.7 This assessment cannot be effectively achieved using the current management scoring system. Our study found that VMI is an independent risk factor in CTEPH, which contrasts with other forms of PAH, where RV hypertrophy is considered an adaptive response.12 The disproportionate increase in RV mass or VMI is associated with lower mortality in idiopathic PAH.13,14 The observed ventricular morphological changes in CTEPH may result from pathogenic factors affecting pulmonary small vessels and myocardium, including factors like transforming growth factor β and tumor necrosis factor-α. This could explain the persistence of RV dysfunction and PH recurrence in many patients even after treating unresolved thrombosis.15,16 LVSVi emerged as a robust protective factor in CTEPH, given the shared changes in biventricles caused by PH.18 This is particularly relevant because augmented RV contractile function and dyssynchrony can negatively impact LV diastolic function and, subsequently, reduce LVSVi.19 CMR has demonstrated its value in predicting adverse clinical outcomes in CTEPH patients, proving at least as effective as current evaluation methods, including invasive hemodynamic measurements. Incorporating CMR-derived biventricular remodeling parameters into management scores can enhance the predictive value. Furthermore, noninvasive CMR alone offers excellent predictive efficacy. Physicians can identify higher-risk patients more accurately when using CMR-based models, especially during the adaptive change phase, allowing for timely and proactive treatment.Conclusion
Biventricular remodeling derived from CMR have long-term value in CTEPH patients to predict adverse clinical outcomes. Risk assessment based on CMR alone is at least as effective as that of clinic combined RHC.Acknowledgements
We thank the Scientific Research Department of the Siemens Company for invaluable technical support.References
1. Humbert M, Kovacs G, Hoeper M M, et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. European Respiratory Journal, 2022: 2200879.
2. Simonneau G, Dorfmüller P, Guignabert C, et al. Chronic thromboembolic pulmonary hypertension: the magic of pathophysiology. Annals of Cardiothoracic Surgery, 2022, 11(2): 106–119.
3. Simonneau G, Torbicki A, Dorfmüller P, et al. The pathophysiology of chronic thromboembolic pulmonary hypertension[J]. European Respiratory Review, 2017, 26(143): 160112.
4. Kawut S M, Poor H D, Parikh M A, et al. Cor pulmonale parvus in chronic obstructive pulmonary disease and emphysema: the MESA COPD study. Journal of the American College of Cardiology, 2014, 64(19): 2000–2009.
5. Van Wolferen S A, Marcus J T, Boonstra A, et al. Prognostic value of right ventricular mass, volume, and function in idiopathic pulmonary arterial hypertension. European Heart Journal, 2007, 28(10): 1250–1257.
6. Swift A J, Rajaram S, Campbell M J, et al. Prognostic Value of Cardiovascular Magnetic Resonance Imaging Measurements Corrected for Age and Sex in Idiopathic Pulmonary Arterial Hypertension. Circulation: Cardiovascular Imaging, 2014, 7(1): 100–106.
7. Bossone E, D’Andrea A, D’Alto M, et al. Echocardiography in pulmonary arterial hypertension: from diagnosis to prognosis. Journal of the American Society of Echocardiography: Official Publication of the American Society of Echocardiography, 2013, 26(1): 1–14.
8. Claeys M, Claessen G, La Gerche A, et al. Impaired Cardiac Reserve and Abnormal Vascular Load Limit Exercise Capacity in Chronic Thromboembolic Disease. JACC. Cardiovascular imaging, 2019, 12(8 Pt 1): 1444–1456.
9. Vonk-Noordegraaf A, Haddad F, Chin K M, et al. Right heart adaptation to pulmonary arterial hypertension: physiology and pathobiology. Journal of the American College of Cardiology, 2013, 62(25 Suppl): D22-33.
10. Homsi R, Luetkens J A, Skowasch D, et al. Left Ventricular Myocardial Fibrosis, Atrophy, and Impaired Contractility in Patients With Pulmonary Arterial Hypertension and a Preserved Left Ventricular Function: A Cardiac Magnetic Resonance Study. Journal of Thoracic Imaging, 2017, 32(1): 36–42.
11. Manders E, Bogaard H-J, Handoko M L, et al. Contractile dysfunction of left ventricular cardiomyocytes in patients with pulmonary arterial hypertension. Journal of the American College of Cardiology, 2014, 64(1): 28–37.
12. Badagliacca R, Poscia R, Pezzuto B, et al. Right ventricular remodeling in idiopathic pulmonary arterial hypertension: adaptive versus maladaptive morphology. The Journal of Heart and Lung Transplantation: The Official Publication of the International Society for Heart Transplantation, 2015, 34(3): 395–403.
13. Goh Z M, Alabed S, Shahin Y, et al. Right Ventricular Adaptation Assessed Using Cardiac Magnetic Resonance Predicts Survival in Pulmonary Arterial Hypertension. JACC. Cardiovascular imaging, 2021, 14(6): 1271–1272.
14. Badagliacca R, Poscia R, Pezzuto B, et al. Right ventricular concentric hypertrophy and clinical worsening in idiopathic pulmonary arterial hypertension. The Journal of Heart and Lung Transplantation: The Official Publication of the International Society for Heart Transplantation, 2016, 35(11): 1321–1329.
15. Kim N H S, Fesler P, Channick R N, et al. Preoperative partitioning of pulmonary vascular resistance correlates with early outcome after thromboendarterectomy for chronic thromboembolic pulmonary hypertension. Circulation, 2004, 109(1): 18–22.
16. Gerges C, Gerges M, Friewald R, et al. Microvascular Disease in Chronic Thromboembolic Pulmonary Hypertension: Hemodynamic Phenotyping and Histomorphometric Assessment. Circulation, 2020, 141(5): 376–386.
17. Simpson C E, Damico R L, Kolb T M, et al. Ventricular mass as a prognostic imaging biomarker in incident pulmonary arterial hypertension. The European Respiratory Journal, 2019, 53(4): 1802067.
18. Cao J, Li S, Cui L, et al. Biventricular Myocardial Strain Analysis in Patients with Pulmonary Arterial Hypertension Using Cardiac Magnetic Resonance Tissue-Tracking Technology. Journal of Clinical Medicine, 2022, 11(8): 2230.
19. Palau-Caballero G, Walmsley J, Van Empel V, et al. Why septal motion is a marker of right ventricular failure in pulmonary arterial hypertension: mechanistic analysis using a computer model. American Journal of Physiology. Heart and Circulatory Physiology, 2017, 312(4): H691–H700.
Figures