1801
Cardiac Magnetic Resonance Assessment of Left Atrium Function and Strain in Hemodialysis Patients: A Preliminary Study1Department of Radiology, West China Hospital of Sichuan University, Chengdu, China, 2GE Healthcare, MR Research, Beijing, China, Beijing, China
Synopsis
Keywords: Myocardium, Cardiovascular
Motivation: Hemodialysis is a common risk factor for cardiovascular disease. Left atrial function and strain are effective predictors of cardiovascular morbidity and mortality.
Goal(s): The aim was to assess the alterations in left atrial function and strain following hemodialysis, with the objective of enabling early diagnosis of cardiac changes and risk stratification in patients with chronic kidney disease (CKD).
Approach: Patients with advanced CKD were enrolled, including those who had not started hemodialysis and those who had started regular hemodialysis. Left atrial function and strain parameters were compared between the two groups.
Results: Left atrial function and strain deteriorated with increasing hemodialysis age.
Impact: Early detection of left atrial function and strain changes and timely intervention are of great significance for the prevention of adverse cardiovascular events in patients with CKD.
Introduction
Hemodialysis is a prevalent risk factor for cardiovascular disease, and the assessment of left atrial function and strain has proven to be a valuable tool in predicting cardiovascular morbidity and mortality. Previous studies have mainly used changes in left ventricular structure and function to predict the occurrence of adverse cardiovascular events in patients with CKD. Several studies have shown that left atrial volume is associated with mortality in hemodialysis patients1, 2. Left atrial ejection fraction (LAEF) and strain have demonstrated a significant association with adverse cardiovascular events in the general population3, 4. However, LAEF and strain have not been extensively studied in the CKD population. Early detection of left atrial function and strain changes in CKD patients is of great significance for the prevention of adverse cardiovascular events. Cardiac magnetic resonance (CMR) feature tracking technique can obtain atrial function and strain parameters using cine sequence. Hence, our study aimed to evaluate the alterations in left atrial function and strain in hemodialysis patients by CMR.Methods
This study was approved by the Local Ethics Committee, and all subjects signed written informed consent. Patients with advanced CKD, including both those who did not initiate hemodialysis and those who commenced regular hemodialysis, were included in the study. Scanning was performed using balanced steady-state free precession (bSSFP) sequence on a 3.0T MR scanner (Signa Premier, GE Healthcare, USA) with electrocardiographic and respiratory gating. Images included continuous short-axis views covering the whole left ventricle, two-chamber, three-chamber, and four-chamber views. Cardiac analysis software CVI 42 version 5.14.2 (Circle Cardiovascular Imaging Inc., Canada) was used to obtain left atrial function and strain parameters. Statistical analyses were performed using IBM SPSS Statistics version 26.0 (IBM Corp., Armonk, NK). The differences between the two groups were compared using independent samples t-test and Mann-Whitney U test. Additionally, Spearman correlation analysis was used to evaluate the relationship between left atrial parameters and hemodialysis age.Results
A total of 43 patients who had started regular hemodialysis and 10 patients who had not started hemodialysis were enrolled. Hemodialysis patients had a significantly lower left ventricular ejection fraction (LVEF) (58.3 ± 8.1% versus 63.6 ± 6.0%, P = 0.036), LAEF total (36.2 ± 8.5% versus 45.9 ± 7.3%, P = 0.002), LAEF booster (21.4 ± 8.2% versus 29.3 ± 7.8%, P = 0.005), global longitudinal strain (GLS) (30.1 ± 8.8% versus 44.1 ± 10.1%, P <0,001) and global radial strain (GRS) (−16.4 ± 3.6% versus −20.4 ± 2.9%, P = 0.002) compared to patients without hemodialysis. LAEF total (r = −0.50, P < 0.001), LAEF passive (r = −0.33, P = 0.016), LAEF booster (r= −0.37, P = 0.006), GLS (r = −0.46, P = 0.001) and GRS (r = 0.43, P = 0.001) were negatively correlated with hemodialysis age. LVEF and right ventricular ejection fraction (RVEF) were not significantly correlated with dialysis age (P > 0.05).Discussion
Left ventricular diastolic dysfunction, hypertrophy, and volume overload may lead to elevated left ventricular filling pressure and left atrial afterload in patients with CKD. These changes trigger a compensatory mechanism in the left atrium, characterized by left atrial dilation and stretching of the myocardium5. This remodeling will lead to left atrial systolic and diastolic dysfunction. Because the left atrial wall is thinner, the changes in left atrial function and strain parameters can reflect cardiac changes earlier than LVEF. In our study, although LVEF was lower in hemodialysis patients compared to non-hemodialysis patients, it remained within the normal range due to the robust compensatory function of the left ventricle. However, LAEF and strain was negatively correlated with the hemodialysis age, suggesting that the longer the duration of hemodialysis, the more severe the deterioration of left atrial function and strain. LVEF did not change significantly with the increase of hemodialysis age due to the strong compensatory capacity of left ventricle. Left atrial size and function serve as indicators of the duration and severity of elevated left ventricular filling pressure3. Our study demonstrated that left atrial function and strain are impaired prior to volume changes, thus being able to predict changes in left atrial diastolic and systolic function. By measuring LAEF and strain, cardiac changes in hemodialysis patients can be detected in a timely manner, facilitating early intervention and improving patient survival rates.Conclusion
With the increase of hemodialysis age, left atrial function and strain in CKD patients deteriorate gradually. LAEF and strain change earlier than LVEF and left atrial volume, which is helpful for early detection of the effect of hemodialysis on the heart in CKD patients.Acknowledgements
No acknowledgement found.References
1. Rankin AJ, Zhu L, Mangion K, et al. Global longitudinal strain by feature-tracking cardiovascular magnetic resonance imaging predicts mortality in patients with end-stage kidney disease. Clinical Kidney Journal. 2021;14(10):2187-2196.
2. Chen S-C, Chang J-M, Tsai Y-C, et al. Left Atrial Diameter and Albumin with Renal Outcomes in Chronic Kidney Disease. International Journal of Medical Sciences. 2013;10(5):575-584.
3. Tanasa A, Tapoi L, Ureche C, et al. Left atrial strain: A novel “biomarker” for chronic kidney disease patients? Echocardiography. 2021;38(12):2077-2082.
4. Kloosterman M, Rienstra M, Crijns HJ, et al. The left atrium: An overlooked prognostic tool. European Journal of Preventive Cardiology. 2017;24(4):389-391.
5. Kaesler N, Babler A, Floege J, Kramann R. Cardiac Remodeling in Chronic Kidney Disease. Toxins. 2020;12(3).
Figures
Figure 1 Flow chart of patient enrollment.
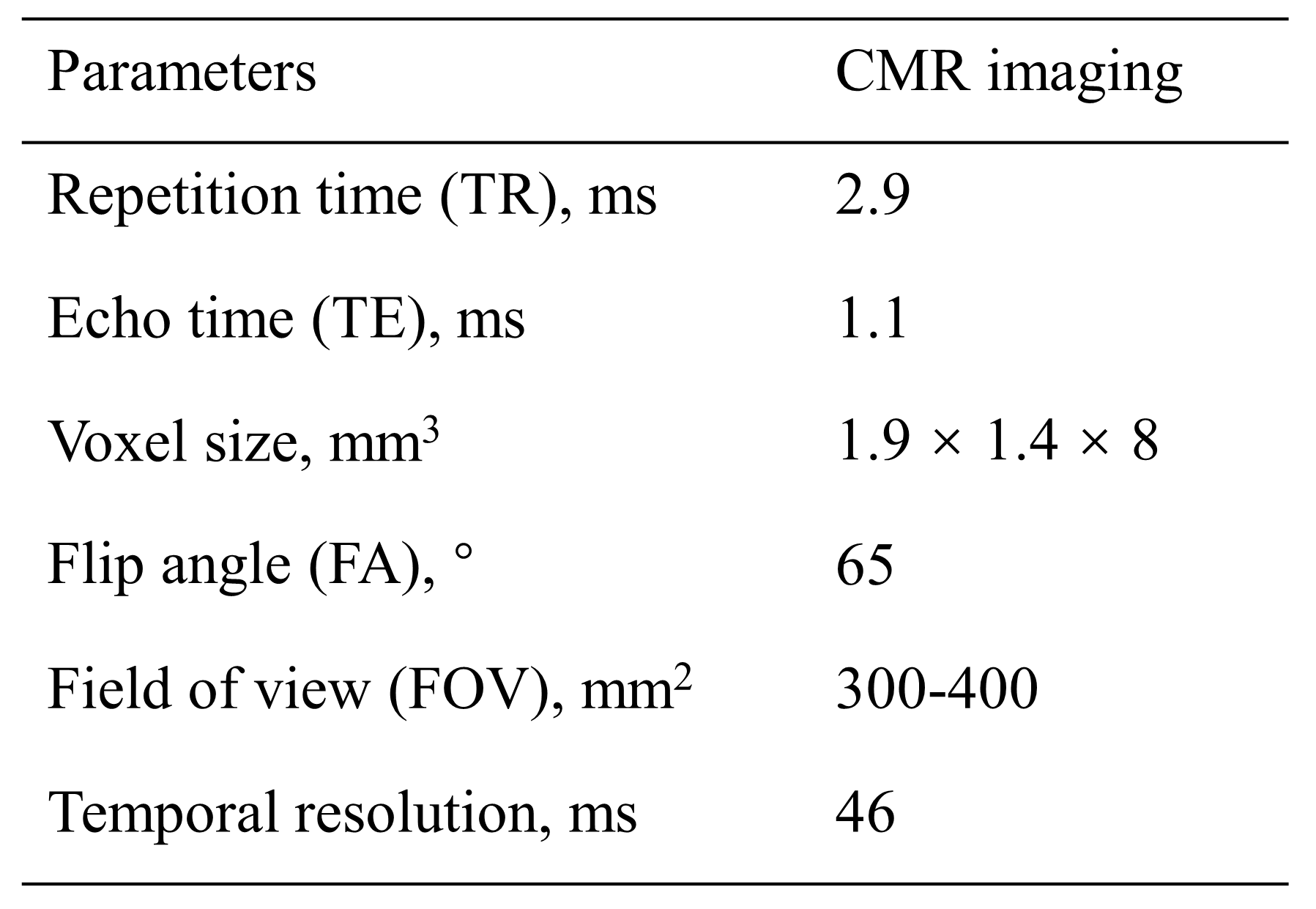
Figure 2 Magnetic resonance scanning parameters.
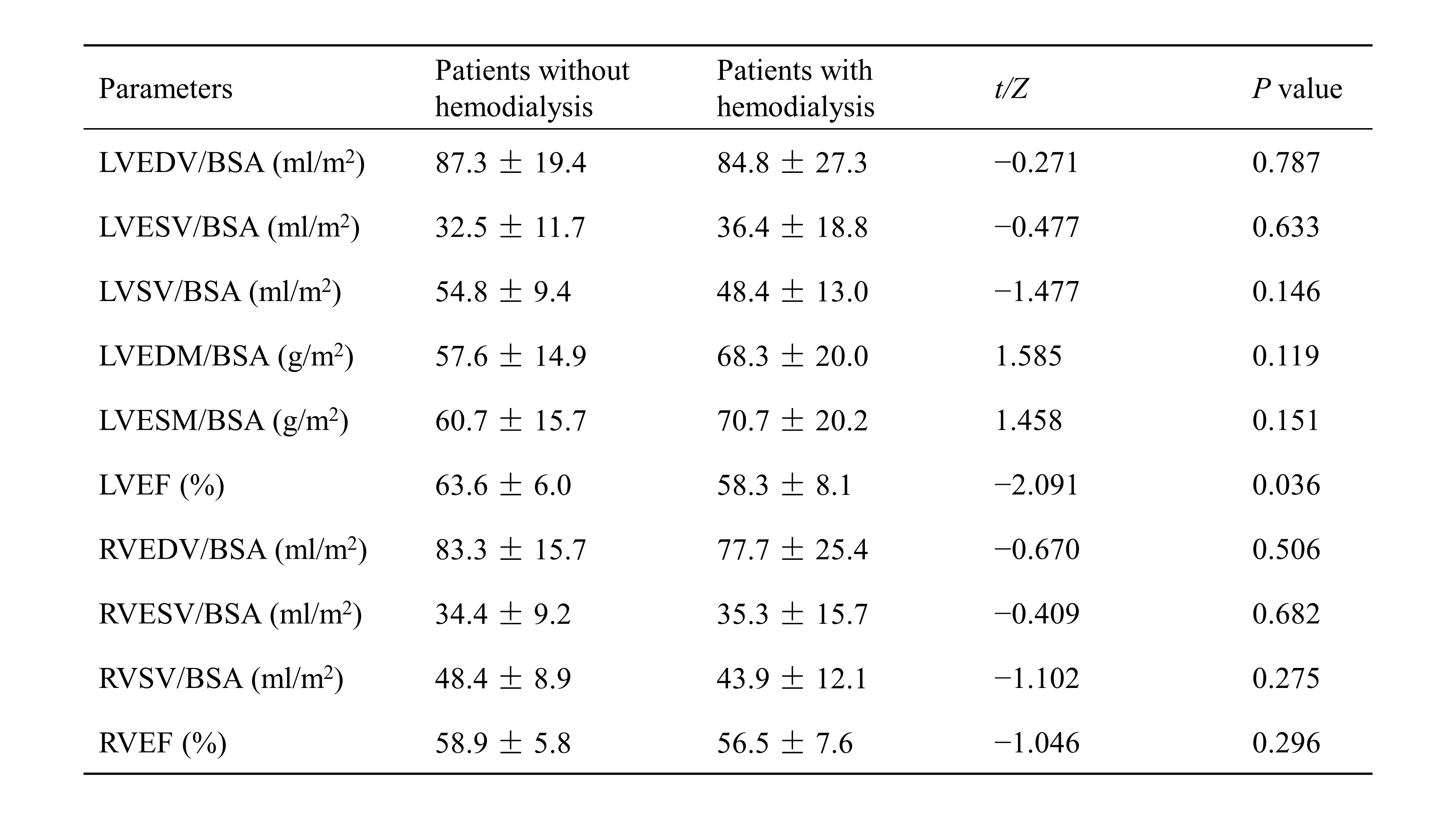
Figure 3 Comparison of ventricular parameters between patients with and without hemodialysis. Note: Left ventricular end-diastolic volume = LVEDV; BSA = body surface area; left ventricular end-systolic volume = LVESV; left ventricular stroke volume = LVSV; left ventricular end-diastolic mass = LVEDM; left ventricular end-systolic mass = LVESM; left ventricular ejection fraction = LVEF; right ventricular end-diastolic volume = RVEDV; right ventricular end-systolic volume = RVESV; right ventricular ejection fraction = RVEF; right ventricular stroke volume = RVSV.
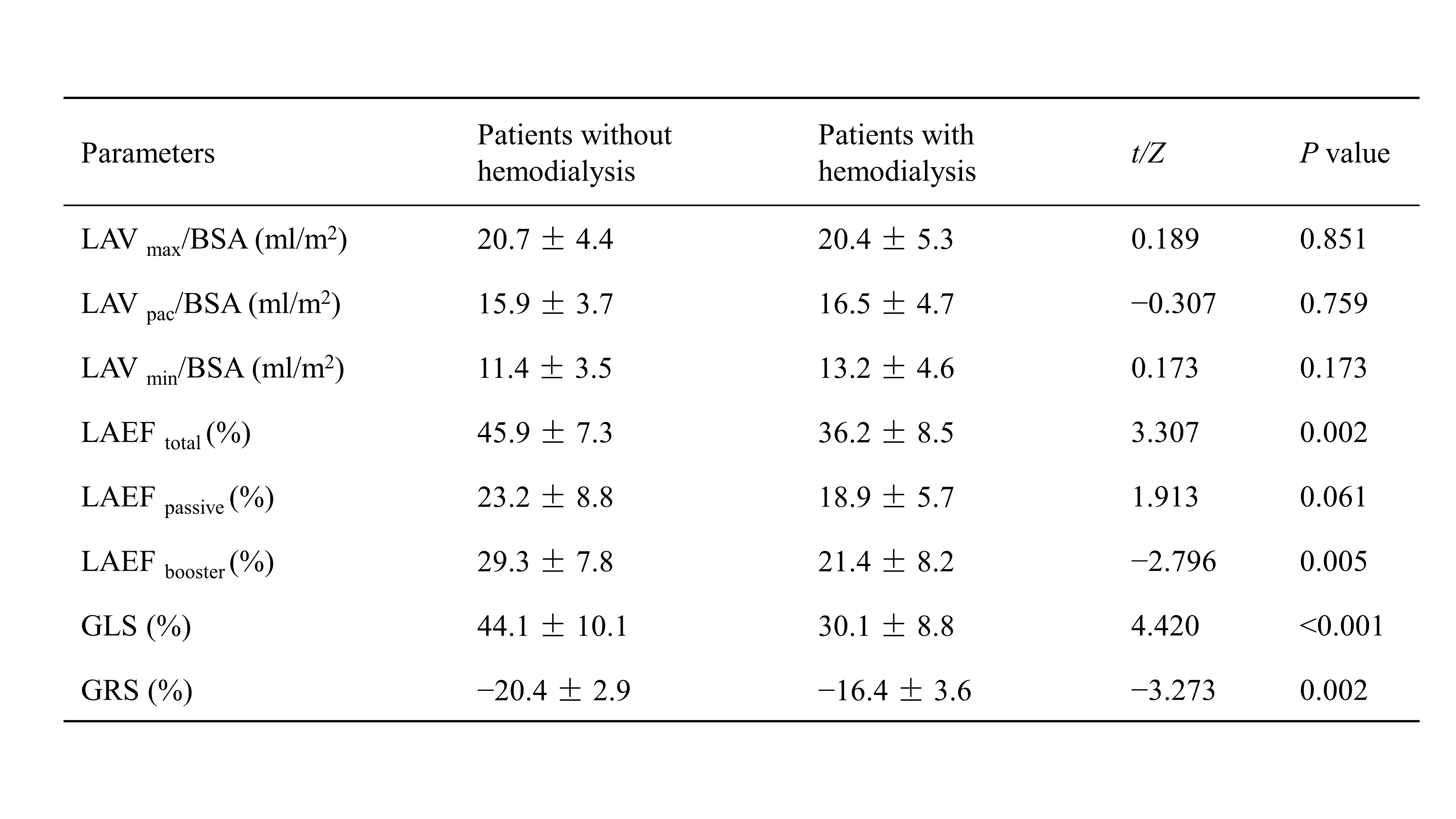
Figure 4 Comparison of left atrial function and strain parameters between patients with and without hemodialysis. Note: Left atrial volume = LAV; BSA = body surface area; left atrial ejection fraction = LAEF; global longitudinal strain = GLS; global radial strain = GRS.
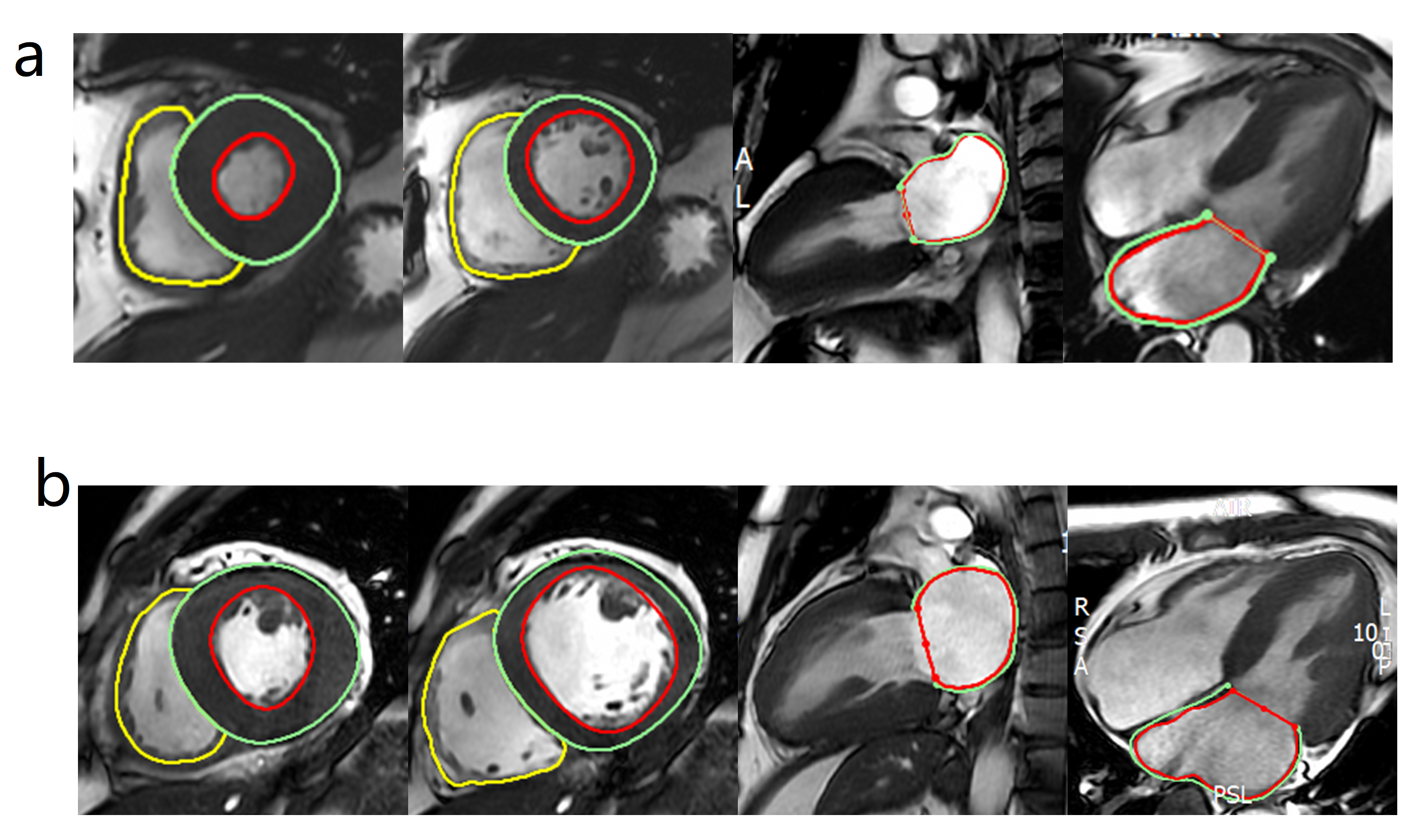
Figure 5 Delineation of endocardial and epicardial borders in hemodialysis (a) and non-hemodialysis (b) patients.