1800
Analysis of the Myocardial Transit-time (MyoTT) between normal subjects and hypertrophic cardiomyopathy patients from a single center in China1Radiology, 1st Medical Center of Chinese PLA General Hospital, Bei Jing, China, 2Radiology, Peking University Cancer Hospital & Institute, Beijing, China, 3Philips Healthcare, BeiJing, China, 4Radiology, Beijing Jishuitan Hospital, Capital Medical University, BeiJing, China, 5Radiology, 1st Medical Center of Chinese PLA General Hospital, Beijing, BeiJing, China
Synopsis
Keywords: Myocardium, Cardiomyopathy
Motivation: Myocardial microvascular disease is widespread in cardiovascular disease and is associated with an increased risk of adverse events. MyoTT, as a relatively novel, non-invasive, and easy-to-perform CMR parameter, played an important role in the diagnosis of disease.
Goal(s): The study aims to observe the differences in myocardial microcirculation time between normal subjects and HCM patients.
Approach: In this study, the CMR resting-state first-pass perfusion imaging sequence was used to measure the change of signal intensities from the coronary ostium to the coronary sinus to calculate the blood circulation time.
Results: Patients with HCM had a significantly prolonged MyoTT compared to controls
Impact: MyoTT could be easily added to current CMR protocols and does not prolong CMR scan time. And future studies are required to evaluate the diagnostic as well as prognostic value of MyoTT in different cardiovascular diseases.
Introduction
Myocardial microvascular diseases are a series of diseases caused by changes in microvascular anatomy, changes in the microvascular wall structure, and changes in the autonomic fine-tuning of vascular tone. Microcirculation dysfunction can lead to myocardial injury and fibrosis. The presence of myocardial microvascular disease is associated with an increased risk of adverse cardiovascular events, and assessment of myocardial microcirculation is of great help in clinical diagnosis and treatment. In hypertrophic cardiomyopathy patients, its severity is strongly associated with a poor prognosis. However, myocardial microcirculation cannot be directly visualized [1]. Although it could be measured by interventional or nuclear medicine methods, these methods are invasive and radioactive, which are not conducive to widespread clinical development. Cardiac magnetic resonance imaging has gradually gained more clinical favors due to its non-invasiveness and non-ionizing radiation. The purpose of this study was to measure myocardial transit-time" (MyoTT) parameter using cardiac magnetic resonance resting-state first-pass perfusion imaging sequences [2].Materials and Methods
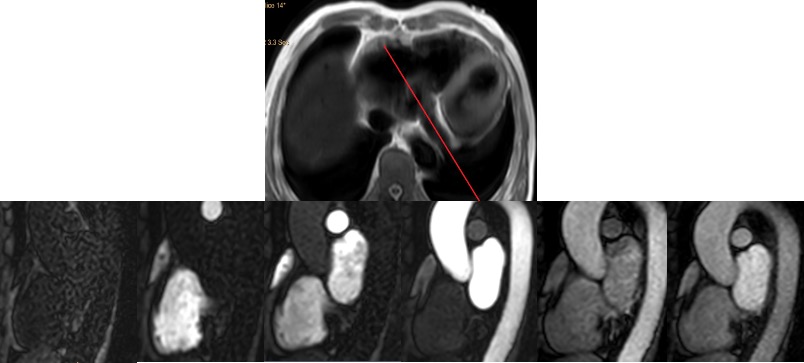
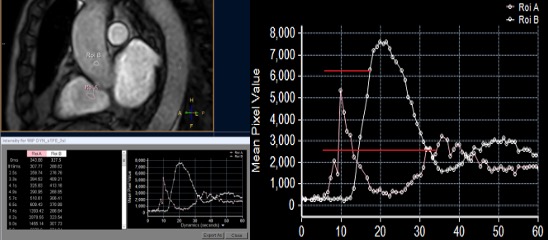
This study included 21 hypertrophic cardiomyopathy patients diagnosed by CMR and clinician (16 male patients and 5 female patients; mean age 50.0±16.0), 21 normal subjects as control group (9 males and 12 females, mean age 41.5±15.2). The BMI of all patients were recorded and classified into 4 degrade according to WHO. All CMR protocols were performed on Philips Ingenia CX 3.0 MRI scanner (Philips Healthcare, Best, The Netherlands) with a 16-channel body phase array coil. The resting state first-pass perfusion images were collected by dynamic turbo-Field echo (TFE) sequence in the free-breathing state. The injection flow rate of the contrast agent was 4.0ml/s. Then 20ml of normal saline was injected at the same rate. The image acquisition parameters were as follows: TR: shortest (2ms)/TE: shortest (1ms), FOV: 300×300mm, Voxel: 2.5x2.5x10mm³, SENSE: 2.3, flip angle:15°. To establish an objective and measurable parameter, we did not just rely on visual observation but accurately recorded the in the signal intensity of the coronary sinus and aortic root at different time during the first-pass perfusion process. The regions of interest (ROI) were placed at aortic root and coronary sinus with an area of at least 0.3cm2. During analysis, the position of the ROI must be manually adjusted to correct for cardiac motion. The detailed description of scanning positioning and measurement of MyoTT are shown in Figure 1 and Figure 2. The changes of the signal intensity of coronary sinus and the required time were exported. The time difference between 80% of the second peak enhancement of the coronary sinus and 80% of the first peak of the aortic root enhancement was calculated to reflect the time of myocardial microcirculation.Results
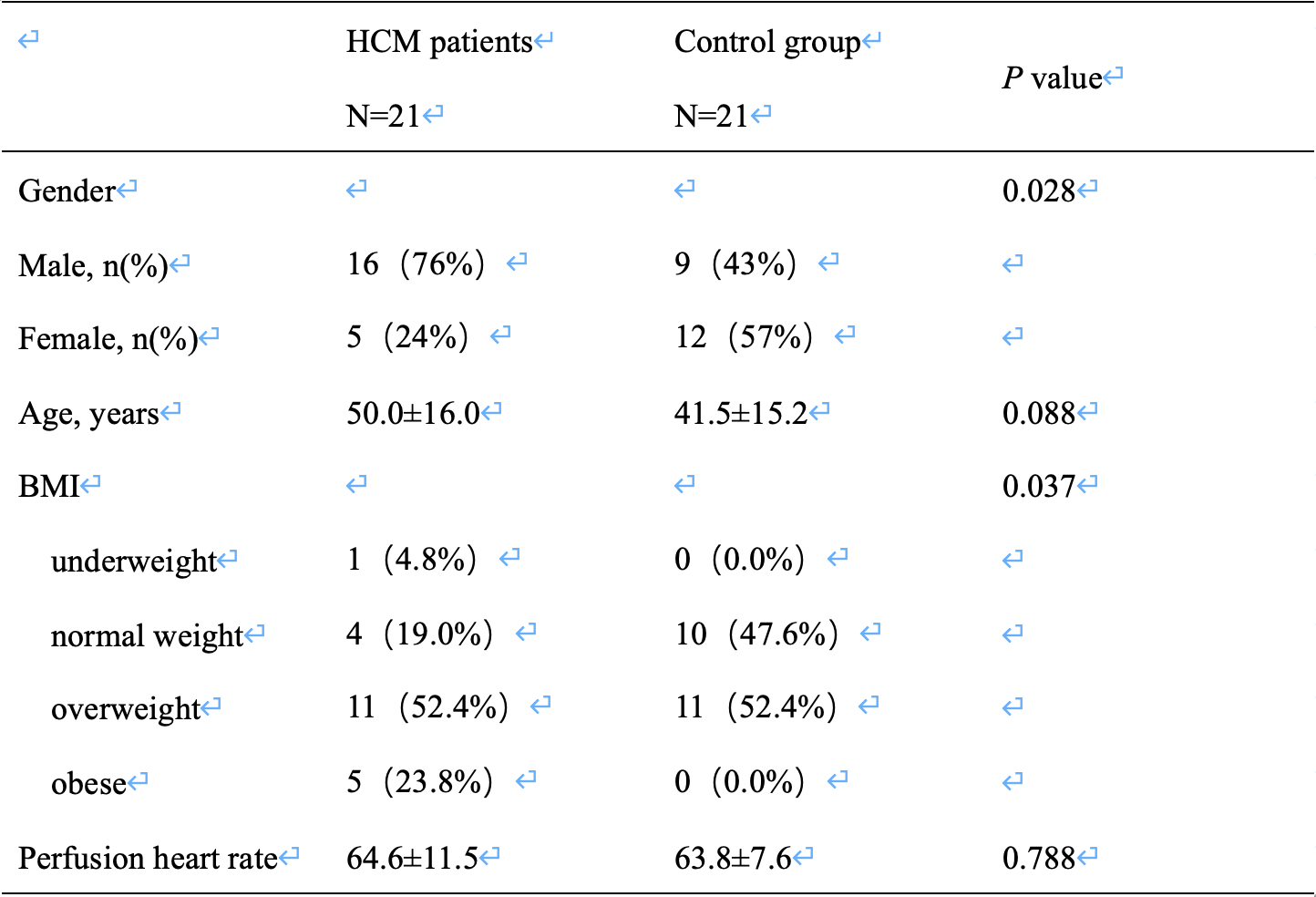
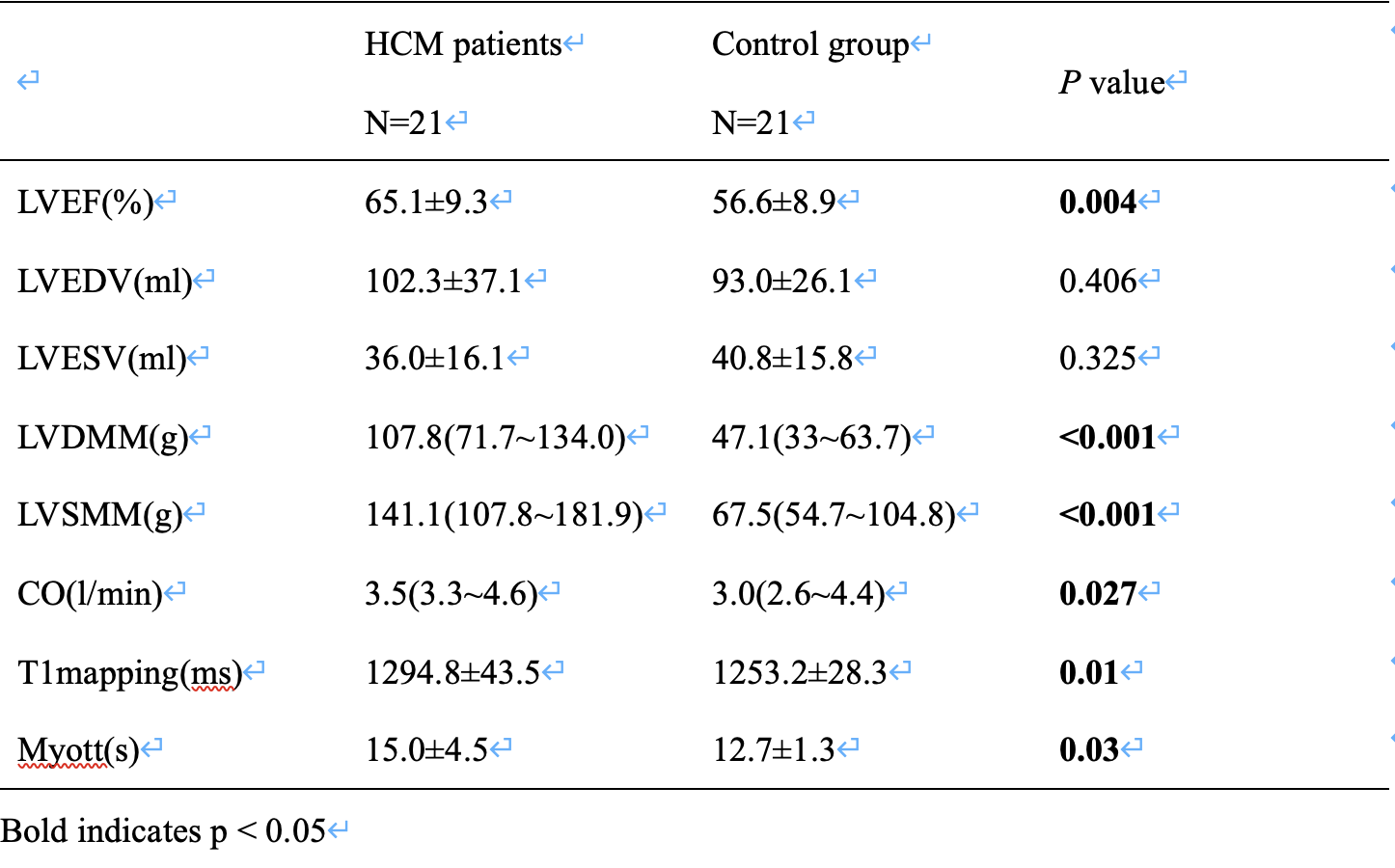
1.The baseline characteristics of the study groups are listed in Table 1. Mean age and perfusion heart rate did not differ significantly between the HCM and the control group. There were slightly more men in the HCM group (76%, p = 0.028) as expected due to the higher prevalence of HCM in males. BMI shows significantly different between the HCM and the control group.2.Functional and structural CMR findings are illustrated in Table 2. Myott shows significantly different between the HCM and the control group. Also,LVEF, CO and T1 values were significantly differ in HCM patients compared to controls. As expected, HCM patients were characterized by an asymmetric pattern of septal wall hypertrophy and a significantly higher LVDMM and LVSMM (both p < 0.001). Left ventricular EDV and ESV did not differ significantly between the HCM and the control group.
3.Patients with HCM had a significantly prolonged MyoTT compared to controls (15.0±4.5s vs. 12.7±1.3 s, p=0.03), as shown in Table 3. In addition, a receiver-operating-characteristic (ROC) analysis was performed, revealing an area-under-the-curve (AUC) of 0.685 to delineate the presence of HCM by MyoTT (Fig. 3). Using a cut-off value of 13.75 s for MyoTT resulted in a sensitivity of 61.9% and a specificity of 81% regarding the correct assessment of HCM based on MyoTT.
Conclusions
MyoTT is a novel, non-invasive and easy-to-implement method to rapidly assess myocardial microcirculation and play an important future role regarding accurate diagnosis and subsequent monitoring of temporal changes of HCM. MyoTT could be easily added to current CMR protocols and does not prolong CMR scan time. In addition, its subsequent analysis can be completed within 3 minutes on average. And future studies are required to evaluate the diagnostic as well as prognostic value of MyoTT in different cardiovascular diseases.Acknowledgements
No acknowledgement found.References
1. Chatzantonis G, Bietenbeck M, Florian A, Meier C, Korthals D, Reinecke H, Yilmaz A. "Myocardial transit-time" (MyoTT): a novel and easy-to-perform CMR parameter to assess microvascular disease. Clin Res Cardiol. 2020 Apr;109(4):488-497. doi: 10.1007/s00392-019-01530-x. Epub 2019 Jul 18. PMID: 31321491.
2. Chatzantonis G, Bietenbeck M, Florian A, Meier C, Stalling P, Korthals D, Reinecke H, Yilmaz A. Diagnostic value of the novel CMR parameter "myocardial transit-time" (MyoTT) for the assessment of microvascular changes in cardiac amyloidosis and hypertrophic cardiomyopathy. Clin Res Cardiol. 2021 Jan;110(1):136-145. doi: 10.1007/s00392-020-01661-6. Epub 2020 May 5. PMID: 32372287; PMCID: PMC7806531.
Figures