1797
Early reverse remodeling of left heart morphology and function evaluated by cardiac magnetic resonance in HOCM afterTA-BSM1Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China, 2Department of Cardiovascular Surgery, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China
Synopsis
Keywords: Myocardium, Cardiomyopathy
Motivation: The assessment of early morphology and functional reverse remodeling of the heart is significant for HOCM patient prognosis.
Goal(s): This study aimed to evaluate the early cardiac morphology and function in HOCM after transapical beating-heart septal myectomy (TA-BSM) using CMR.
Approach: 41 HOCM patients who underwent CMR before after TA-BSM were prospectively enrolled in the study. Preoperative and postoperative cardiac morphological and functional parameters were compared.
Results: LVEF, wall thickness, LVMI, and LVRI decreased after TA-BSM. The △LVOTG and baseline LVMI were independently associated with greater left ventricular mass regression.
Impact: Surgery relieves the mechanical stress overload of the left ventricle (LV) and greatly improves the LV hyperdynamic state. It is essential to evaluate left heart morphology and function accurately after TA-BSM.
Introduction
Hypertrophic cardiomyopathy (HCM) is an autosomal dominant cardiomyopathy with an incidence of 0.2 to 0.5% and is characterized by asymmetric myocardial hypertrophy [1]. Hypertrophic obstructive cardiomyopathy (HOCM) often causes severe symptoms and decreased labor endurance, placing patients at high risk of sudden cardiac death (SCD) and progressive heart failure (HF) [2]. Transapical beating-heart septal myectomy (TA-BSM) [3] is a new type of precision ventricular septal myectomy characterized by being minimally invasive and independent of the need for extracorporeal circulation. This study aimed to evaluate the morphological and functional parameters of the left heart before and after TA-BSM in HOCM patients using CMR and to further explore the factors associated with reverse remodeling.Methods
Study cohortThe study prospectively enrolled 80 HOCM patients who underwent TA-BSM in Tongji Hospital from April 2022 to January 2023. All patients were diagnosed as having HCM based on the published guidance.
Cardiac MRI scanning protocol
All patients underwent a standard CMR examination on a 3T system (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany). Cine images were acquired with ECG-gated and breath-holding using a segmented, balanced, steady-state free-precession sequence.
MRI data analysis
All CMR function analyses were performed using commercial cardiac software (CVI 42, version 5.14.0, Circle Cardiovascular Imaging Inc., Canada). Left ventricular end-diastolic diameter (LVEDD) was measured in the middle short-axial slice at the end-diastolic phase. Left ventricular end-diastolic volume (LVEDV), left ventricular end-systolic volume (LVESV), stroke volume (SV), cardiac output (CO), left ventricular ejection fraction (LVEF), and left ventricular mass (LVM) were obtained through end-diastolic and end-diastolic delineation. The left ventricular remodeling index (LVRI) was calculated as: LVRI = LVM / LVEDV.
Statistical analysis
Statistical analysis of preoperative and postoperative CMR data was performed using SPSS statistical software (version 25.0, IBM SPSS Inc., Chicago, IL). Parameters at baseline and follow-up CMR were compared using the paired t-test or paired Wilcoxon signed-ranks test. Predictors of the left ventricular mass index (LVMI) reduction and LVRI were calculated using a stepwise multiple linear regression model entered as covariate factors. P<0.05 was considered statistically significant.
Results
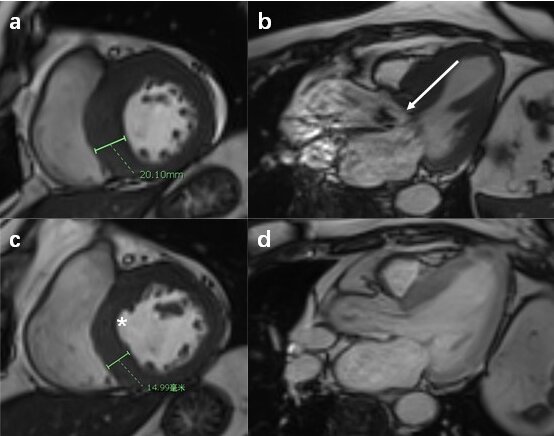
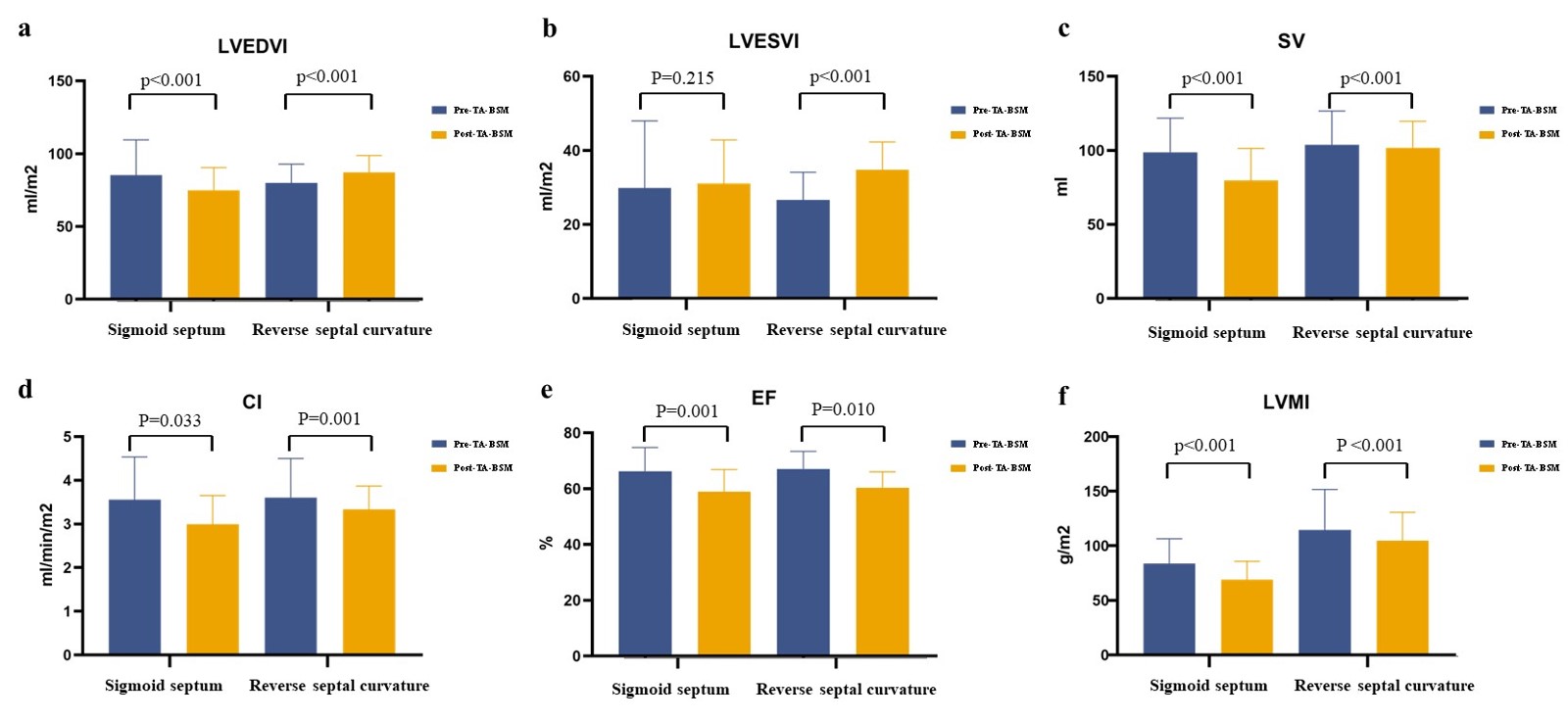
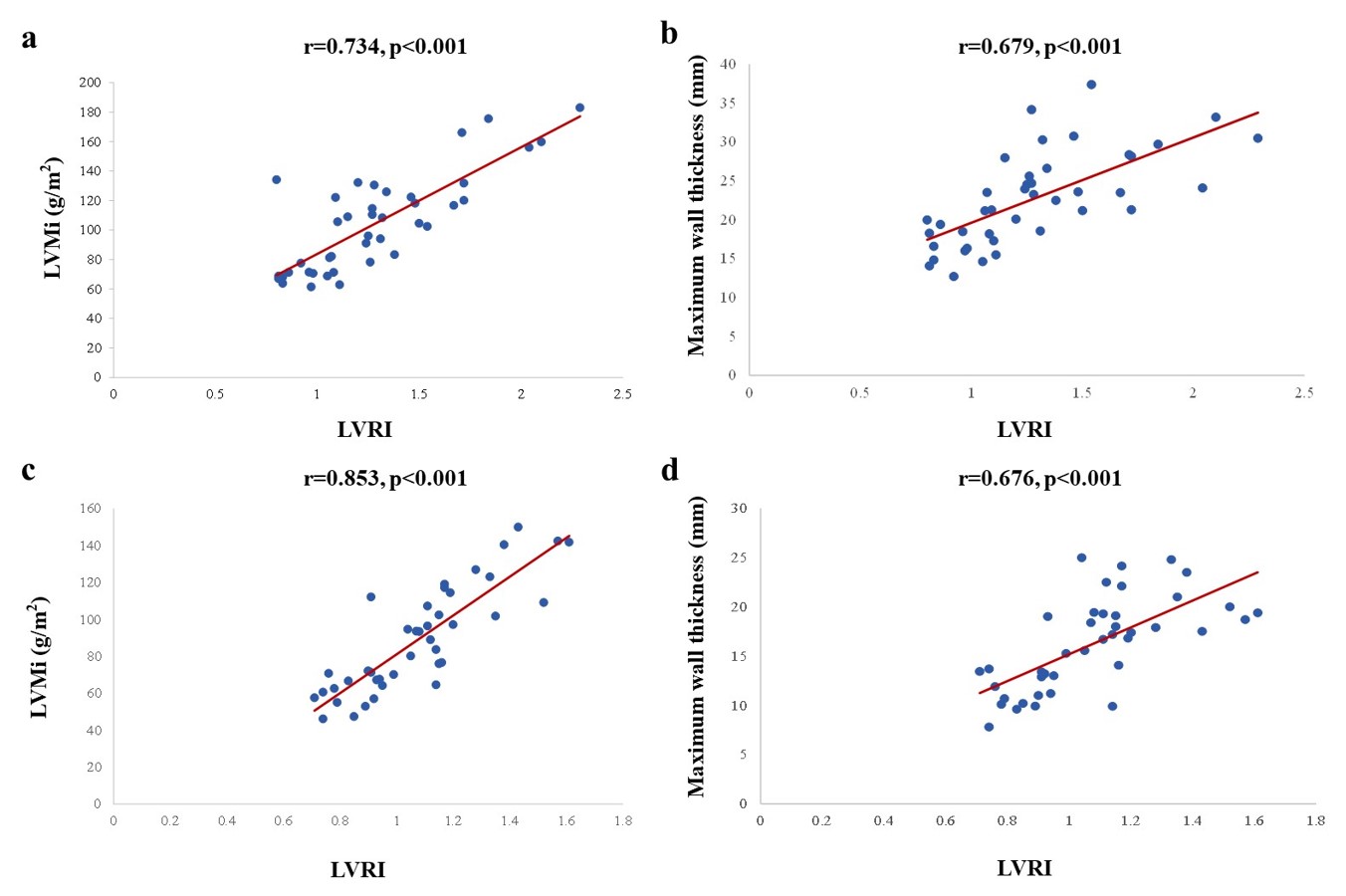
Changes in morphology and functionSV, CI, LVMI, LVRI, LVEF, maximum wall thickness, maximum wall thickness in non-surgical segments, and LVMI decreased after TA-BSM (all p < 0.05) (Fig. 2). The left ventricular end-diastolic volume index (LVEDVI) and LVEDD decreased in patients with a sigmoid septum postoperatively (82.7 ml/m2 vs. 72.8 ml/m2, 50.6 (48.2, 56.5) mm vs. 47.2 (42.7, 50.1) mm, both p < 0.001) but increased in patients with reverse septal curvature (79.6 ml/m2 vs. 87.0 ml/m2, 44.9±1.1 mm vs. 51.3 ± 0.9, both p < 0.001) LVMI and maximum wall thickness were significantly correlated with LVRI preoperatively (rs = 0.734 and r = 0.679, both p < 0.001). After TA-BSM, both remained significantly associated with LVRI (Fig. 3). n the multivariate analysis,△LVOTG (adjusted β = 0.323, p = 0.018) and baseline LVMI (adjusted β = 0.436, p < 0.040) were independent predictors of LV mass regression. In addition, the weight of the resected myocardium (adjusted β = 0.476, p = 0.005) and △mitral regurgitation degree (adjusted β = -0.245, p = 0.040) were associated with △LVRI.
Discussion
In this study, we performed a pre- and postoperative structural and functional analysis of the left heart during the TA-BSM procedure. There are two primary mechanisms of myocardial hypertrophy. The first is when genetic factors lead to cardiomyocyte hypertrophy and extracellular matrix fibrosis; the other is secondary hypertrophy caused by increased afterload [4]. Genes are the initiating factors that drive cardiomyocyte hypertrophy and extracellular matrix proliferation. Hypertrophic myocardium has hypercontractility, resulting in increased power output [5]. However, the normal turbulent state of blood in the aorta is disturbed due to LVOT obstruction, particularly in patients with basal ventricular septal hypertrophy. Abnormal ejection and the increased contractile capacity of cardiomyocytes further increase left ventricular systolic pressure. Abnormal circulation in the heart chambers and outflow tract prompts further myocardial remodeling and aggravation of fibrosis. Initially, myocardial remodeling was used to describe changes in ventricular expansion and cardiomyocytes after myocardial infarction [6]. Ventricular remodeling describes changes in the overall geometry and deterioration of ventricular contractile function [4]. The process of left ventricular remodeling is due to prolonged volume or pressure overload, myocardial cell degeneration, and changes in the extracellular composition [7]. Subsequently, the end-diastolic pressure-volume relationship in the ventricle was introduced to evaluate structural remodeling [8].Conclusions
Our study summarizes the CMR findings indicative of left heart remodeling after TA-BSM. The structure and function were recovered to some extent.Acknowledgements
No acknowledgement found.References
[1] Elliott PM, Anastasakis A, Borger MA, Borggrefe M, Cecchi F, Charron P, Hagege AA, Lafont A, Limongelli G, Mahrholdt H, McKenna WJ, Mogensen J, Nihoyannopoulos P, Nistri S, Pieper PG, Pieske B, Rapezzi C, Rutten FH, Tillmanns C, Watkins H. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: the Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur Heart J. 2014 Oct 14;35(39):2733-79. doi: 10.1093/eurheartj/ehu284. Epub 2014 Aug 29. PMID: 25173338.
[2] Maron BJ, Maron MS. Hypertrophic cardiomyopathy. Lancet. 2013 Jan 19;381(9862):242-55. doi: 10.1016/S0140-6736(12)60397-3. Epub 2012 Aug 6. PMID: 22874472.
[3] Fang J, Liu Y, Zhu Y, Li R, Wang R, Wang DW, Song Y, Li C, Chen Y, Cheng L, Zheng K, Zhao Y, Li S, Cheng C, Xia L, Chen X, Wan S, Wei X. First-in-Human Transapical Beating-Heart Septal Myectomy in Patients With Hypertrophic Obstructive Cardiomyopathy. J Am Coll Cardiol. 2023 Aug 15;82(7):575-586. doi: 10.1016/j.jacc.2023.05.052. PMID: 37558369.
[4] Kim GH, Uriel N, Burkhoff D. Reverse remodelling and myocardial recovery in heart failure. Nat Rev Cardiol. 2018 Feb;15(2):83-96. doi: 10.1038/nrcardio.2017.139. Epub 2017 Sep 21. PMID: 28933783.
[5] Baxi AJ, Restrepo CS, Vargas D, Marmol-Velez A, Ocazionez D, Murillo H. Hypertrophic Cardiomyopathy from A to Z: Genetics, Pathophysiology, Imaging, and Management. Radiographics. 2016 Mar-Apr;36(2):335-54. doi: 10.1148/rg.2016150137. PMID: 26963450.
[6] Hochman JS, Bulkley BH. Expansion of acute myocardial infarction: an experimental study. Circulation. 1982 Jun;65(7):1446-50. doi: 10.1161/01.cir.65.7.1446. PMID: 7074800.
[7] Sutton MS, Keane MG. Reverse remodelling in heart failure with cardiac resynchronisation therapy. Heart. 2007 Feb;93(2):167-71. doi: 10.1136/hrt.2005.067967. Epub 2006 Apr 27. PMID: 16644861; PMCID: PMC1861399.
[8] Pfeffer JM, Pfeffer MA, Fletcher PJ, Braunwald E. Progressive ventricular remodeling in rat with myocardial infarction. Am J Physiol. 1991 May;260(5 Pt 2):H1406-14. doi: 10.1152/ajpheart.1991.260.5.H1406. PMID: 2035662.
Figures