1794
Impact of Epicardial Adipose Tissue Assessed by CMR on Atrial Fibrillation in Heart Failure with Preserved Ejection Fraction1the Second Affiliated Hospital of Harbin Medical University, HarBin, China, 2Beihang University, BeiJing, China
Synopsis
Keywords: Heart Failure, Heart
Motivation: Heart failure with preserved ejection fraction (HFpEF) frequently presents with atrial fibrillation (AF). But the mechanism of AF in HFpEF are incompletely understood. Epicardial adipose tissue (EAT) is linked with left atrial volume and function changes.
Goal(s): This study aims to evaluate the relationships between EAT volumes and AF in patients with HFpEF.
Approach: All subjects were imaged with a 3.0T Philips scanner. CMR parameters were quantified with a stack of short axis views perpendicular to the long axis of the left ventricle.
Results: EAT was an independent predictor for the presence of AF in patients with HFpEF and demonstrated high prediction power.
Impact: EAT plays an important role in the progression of HFpEF and may be a promising therapeutic target.
Introduction
Heart failure with preserved ejection fraction (HFpEF) presenting as diastolic dysfunction that affects about half of all patients with heart failure. HFpEF is frequently characterized by atrial fibrillation (AF), which is associated with increased embolic risk and mortality 1. Epicardial adipose tissue (EAT), a metabolically active visceral fat depot located between the pericardium and myocardium 2, 3. It has the potential cardiotoxic implications via the secretion of proinflammatory and profibrotic cytokines by paracrine, endocrine and vasocrine pathway 4, 5, which is associated with heart remodeling and dysfunction 5-7. It was demonstrated that patients with HFpEF exhibited higher EAT than those control subjects 8. Recently, studies have revealed that EAT was associated with left atrial (LA) volume and function changes9-11. However, to date, the available evidence linking EAT to HFpEF and the pathogenesis of AF is limited. In this study, we aimed to clarify the association between EAT and AF and cardiac function derived by CMR-FT in patients with HFpEF through accurately volumetric assessment of EAT using CMR imaging.Methods
In total, 108 HFpEF patients fulfilled the inclusion criteria. All participants underwent cardiac magnetic resonance (CMR) examination on 3.0T platform (Ingenia CX, Philips Healthcare, the Netherlands). EAT volume and LV and LA strains were measured by CVI42 software, LA strain with different phases were included, such as reservoir, conduit and booster pump strain.Results
HFpEF patients had significant impaired diastolic function, evidenced by larger GLS (-12.1±3.7 vs. -17.3±2.2, P <0.001), paralleling smaller LA reservoir strain (20.2 ± 10.8 vs. 40.8 ± 11.8, P <0.001), conduit strain (8.9 ± 6.4 vs. 21.2 ± 8.7, P <0.001), and booster pump strain (11.1 ± 7.1 vs. 19.1 ± 7.8, P <0.001) (Table 1). Regarding the correlations with EAT and CMR functional parameters, heart rate, LVEDV index, LVESV index, LA volume index and LVM index were significant correlation with EAT (r = 0.169, 0.16, 0.21, 0.20 and 0.316, respectively) (Table 2). Figure 1 shows correlations between EAT and CMR diastolic functional parameters, that greater EAT volume was associated with lower reservoir, conduit, and booster pump strain (r = -0.417, -0.364 and -0.298, respectively) and impaired GLS (r = 0.368, P<0.001).After adjustment for hypertension, heart rate, LV mass index, LA volume index, cardiac index, and LV global longitudinal strain (GLS), and LA strains, EAT was the independent risk of AF occurrence in any of the multivariable models (Table 3). EAT had a high predictive ability for AF (AUC = 0.65, 95% CI, 0.56-0.74, P=0.000). Furthermore, receiver operating characteristic curve analysis demonstrated that integration of EAT, GLS, LA reservoir strain, LA conduit strain, and LA booster pump strain provided better discriminatory abilities for incident AF in HFpEF patients with the high sensitivity of 91.7% and the specificity of 82.1% (AUC=0.921, 95% CI, 0.853–0.964, P= 0.000) (Figure 2).Discussion
Accumulating evidence supported the association between EAT and the presence of AF 12, 13, as well as an association between EAT and the recurrence of AF following postablation14. A meta-analysis included 10 studies conducted by Zhu et al. suggested that EAT volume could be associated with AF and the EAT volume was larger in patients with persistent AF than that in patients with paroxysmal AF15. Our current study demonstrated that EAT could be an independent predictor of the presence of AF in patients with HFpEF and demonstrated high prediction power. Moreover, integration of EAT, GLS and three LA strains offered a significantly better predictive ability in patients with HFpEF with AUC of 0.921(95% CI, 0.85-0.96).EAT may potentially cause myocardial fibrosis and microcirculation disturbance, which could lead to the onset of AF. EAT has been demonstrated to secrete large amounts of adipokines such as TGF-β1, cTGF, and activin A, which may promote the progression of myocardial fibrosis16-18. In addition, the ability of EAT for promoting myocardial fibrosis has also been substantiated in an animal study19. Meanwhile, the pro-inflammatory adipokines secreted by EAT including leptin, TNF-α, IL-1β, and IL-6, could introduce microvascular obstruction20, ultimately leading to diastolic dysfunction21. The pro-fibrotic factors (i.e., MMPs and TGF-β1) released by EAT affect the interstitial expansion of atrial myocyte bundles, consequently promoting the electrophysiological remodeling of the atria22. Recent clinical studies have shown that reducing the EAT through weight reduction or pharmacologic interventions could improve the cardiac function23, 24.
Conclusions
EAT serves as an independent factor in the development of AF in patients with HFpEF. EAT may indeed play an significant role in the progression of HFpEF and may be a promising therapeutic target.Acknowledgements
No acknowledgement found.References
1. Reddy Y, Obokata M, Verbrugge F, Lin G, Borlaug B. Atrial Dysfunction in Patients With Heart Failure With Preserved Ejection Fraction and Atrial Fibrillation. Journal of the American College of Cardiology. 2020;76(9):1051-1064.
2. Pugliese N, Paneni F, Mazzola M, et al. Impact of epicardial adipose tissue on cardiovascular haemodynamics, metabolic profile, and prognosis in heart failure. European journal of heart failure. 2021;23(11):1858-1871.
3. Koepp K, Obokata M, Reddy Y, Olson T, Borlaug B. Hemodynamic and Functional Impact of Epicardial Adipose Tissue in Heart Failure With Preserved Ejection Fraction. JACC Heart failure. 2020;8(8):657-666.
4. Iacobellis G. Local and systemic effects of the multifaceted epicardial adipose tissue depot. Nature reviews Endocrinology. 2015;11(6):363-371.
5. Iacobellis G. Epicardial adipose tissue in contemporary cardiology. Nature reviews Cardiology. 2022;19(9):593-606.
6. Iacobellis G, Barbaro G. Epicardial adipose tissue feeding and overfeeding the heart. Nutrition (Burbank, Los Angeles County, Calif). 2019;59:1-6.7. Sacks H, Fain J. Human epicardial fat: what is new and what is missing? Clinical and experimental pharmacology & physiology. 2011;38(12):879-887.
8. van Woerden G, Gorter TM, Westenbrink BD, Willems TP, van Veldhuisen DJ, Rienstra M. Epicardial fat in heart failure patients with mid-range and preserved ejection fraction. Eur J Heart Fail. 2018;20(11):1559-1566.
9. Mookadam F, Goel R, Alharthi MS, Jiamsripong P, Cha S. Epicardial fat and its association with cardiovascular risk: a cross-sectional observational study. Heart Views. 2010;11(3):103-108.
10. Kilicaslan B, Ozdogan O, Aydin M, Dursun H, Susam I, Ertas F. Increased epicardial fat thickness is associated with cardiac functional changes in healthy women. Tohoku J Exp Med. 2012;228(2):119-124.
11. Fox CS, Gona P, Hoffmann U, et al. Pericardial fat, intrathoracic fat, and measures of left ventricular structure and function: the Framingham Heart Study. Circulation. 2009;119(12):1586-1591.
12. Haemers P, Hamdi H, Guedj K, et al. Atrial fibrillation is associated with the fibrotic remodelling of adipose tissue in the subepicardium of human and sheep atria. European heart journal. 2017;38(1):53-61.
13. Kusayama T, Furusho H, Kashiwagi H, et al. Inflammation of left atrial epicardial adipose tissue is associated with paroxysmal atrial fibrillation. Journal of cardiology. 2016;68(5):406-411.
14. Anagnostopoulos I, Kousta M, Kossyvakis C, et al. Epicardial Adipose Tissue and Atrial Fibrillation Recurrence following Catheter Ablation: A Systematic Review and Meta-Analysis. Journal of clinical medicine. 2023;12(19).
15. Zhu W, Zhang H, Guo L, Hong K. Relationship between epicardial adipose tissue volume and atrial fibrillation : A systematic review and meta-analysis. Herz. 2016;41(5):421-427.
16. Zeller J, Krüger C, Lamounier-Zepter V, et al. The adipo-fibrokine activin A is associated with metabolic abnormalities and left ventricular diastolic dysfunction in obese patients. ESC heart failure. 2019;6(2):362-370.
17. Al-Talabany S, Mordi I, Graeme Houston J, et al. Epicardial adipose tissue is related to arterial stiffness and inflammation in patients with cardiovascular disease and type 2 diabetes. BMC cardiovascular disorders. 2018;18(1):31.
18. Chen Y, Liu F, Han F, et al. Omentin-1 is associated with atrial fibrillation in patients with cardiac valve disease. BMC cardiovascular disorders. 2020;20(1):214.
19. Venteclef N, Guglielmi V, Balse E, et al. Human epicardial adipose tissue induces fibrosis of the atrial myocardium through the secretion of adipo-fibrokines. European heart journal. 2015;36(13):795-805a.
20. Gruzdeva O, Akbasheva O, Dyleva Y, et al. Adipokine and Cytokine Profiles of Epicardial and Subcutaneous Adipose Tissue in Patients with Coronary Heart Disease. Bulletin of experimental biology and medicine. 2017;163(5):608-611.
21. Zhou H, An D, Ni Z, et al. Magnetic Resonance Imaging Quantification of Accumulation of Epicardial Adipose Tissue Adds Independent Risks for Diastolic Dysfunction among Dialysis Patients. Journal of magnetic resonance imaging : JMRI. 2022;56(4):1184-1194.
22. Fang W, Xie S, Deng W. Epicardial Adipose Tissue: a Potential Therapeutic Target for Cardiovascular Diseases. Journal of cardiovascular translational research. 2023.
23. Ishikawa H, Otsuka K, Kono Y, et al. Extent of coronary atherosclerosis is associated with deterioration of left ventricular global longitudinal strain in patients with preserved ejection fraction undergoing coronary computed tomography angiography. International journal of cardiology Heart & vasculature. 2023;44:101176.
24. Zhao N, Wang X, Wang Y, et al. The Effect of Liraglutide on Epicardial Adipose Tissue in Type 2 Diabetes. Journal of diabetes research. 2021;2021:5578216.
Figures
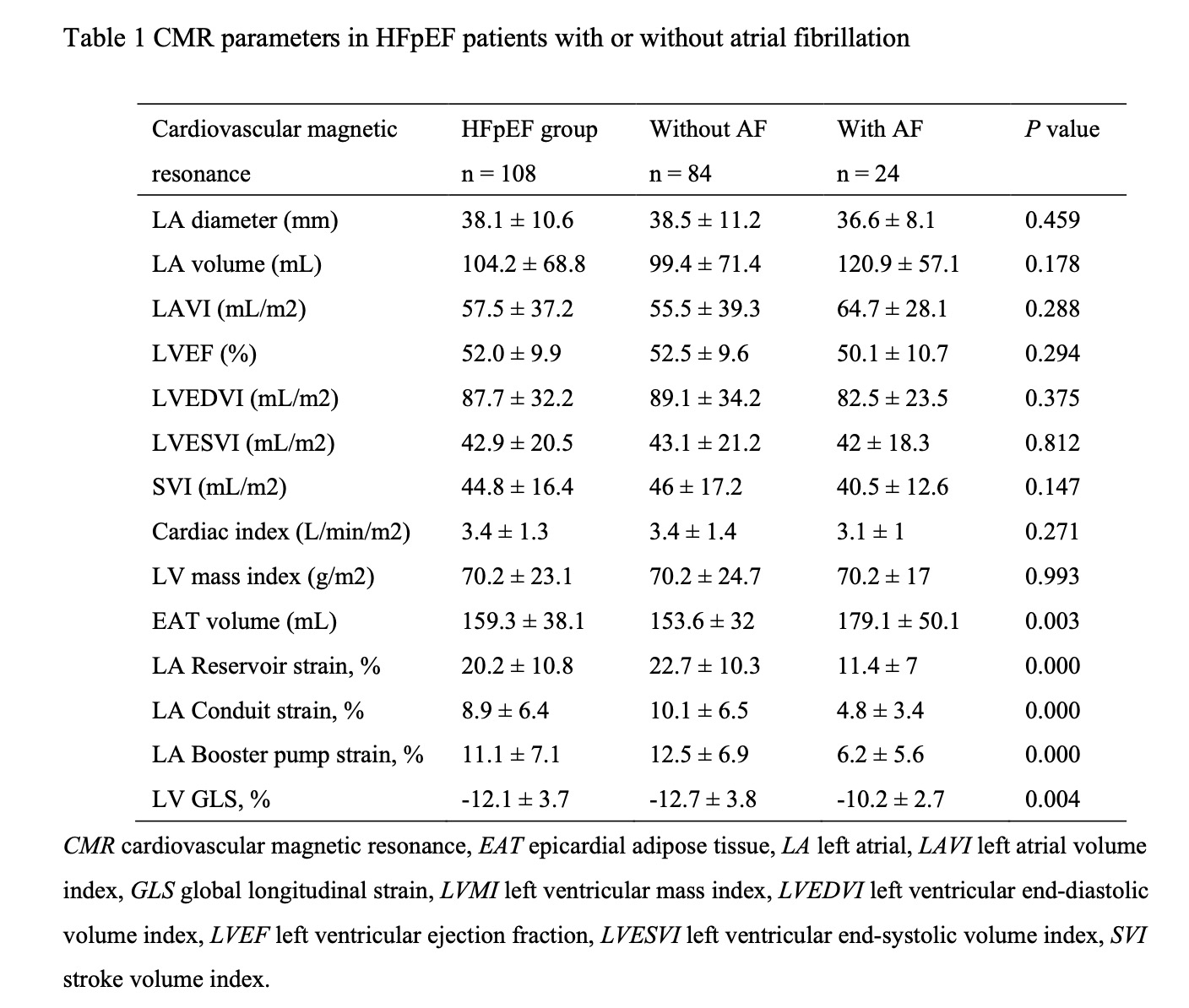
Table 1 CMR parameters in HFpEF patients with or without atrial fibrillation
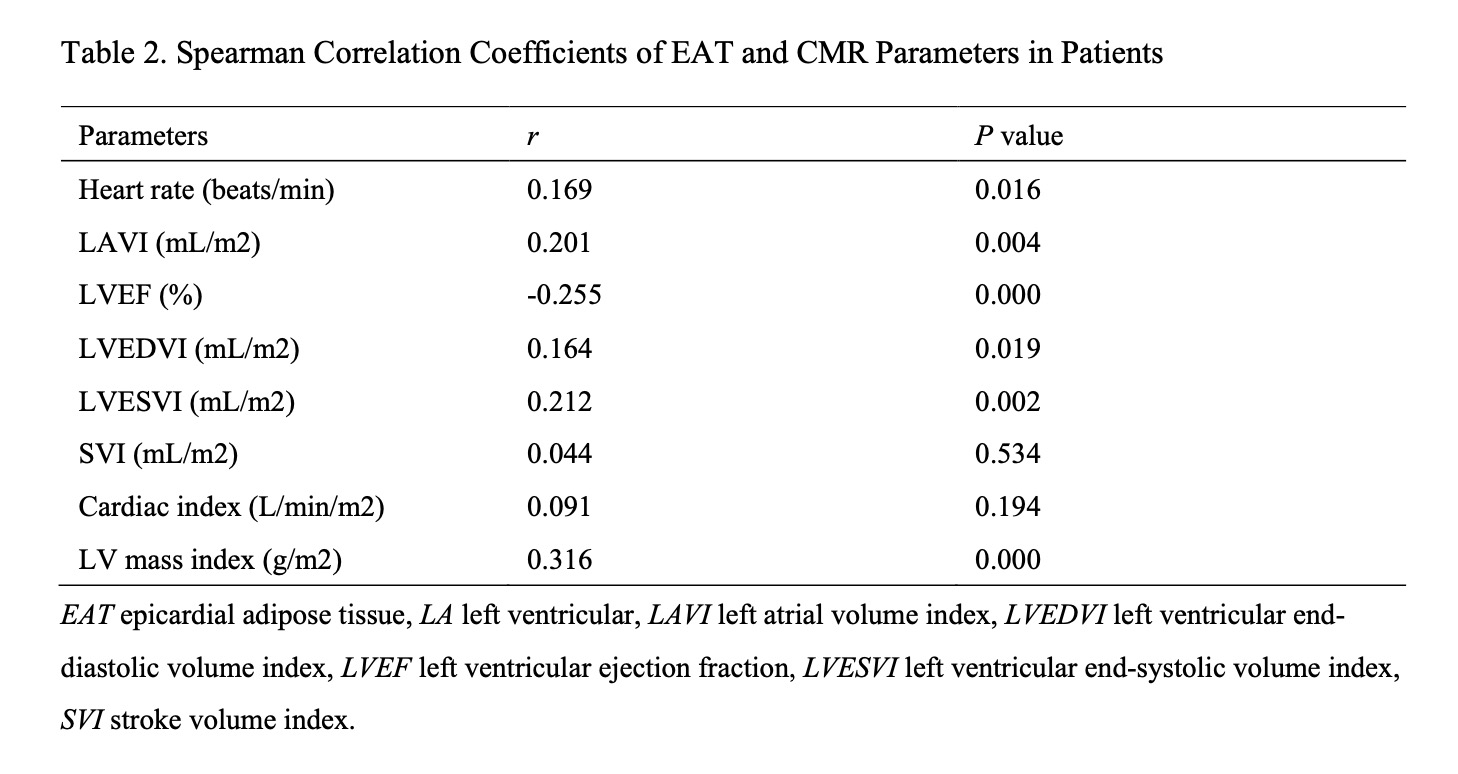
Table 2. Spearman Correlation Coefficients of EAT and CMR Parameters in Patients
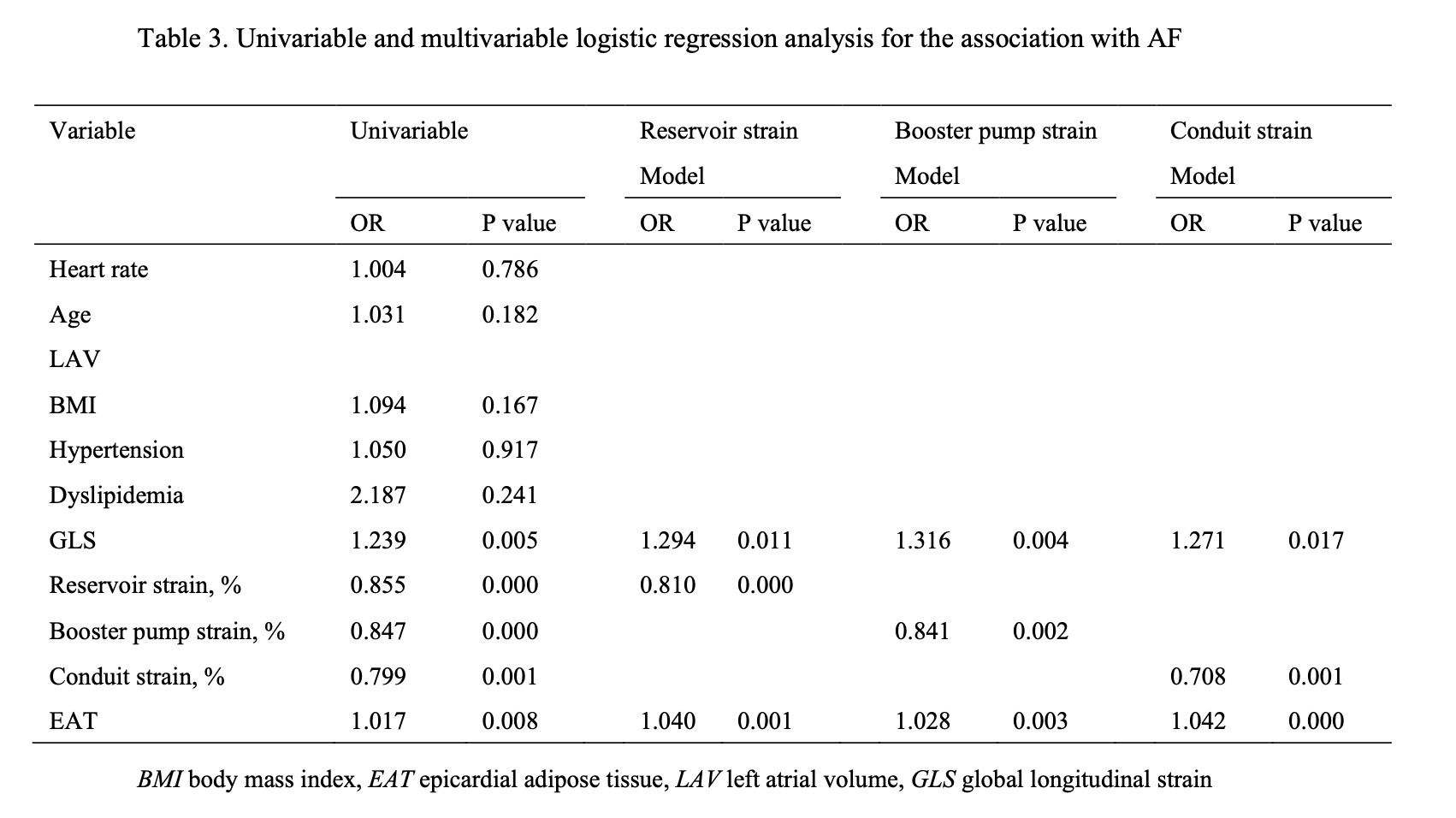
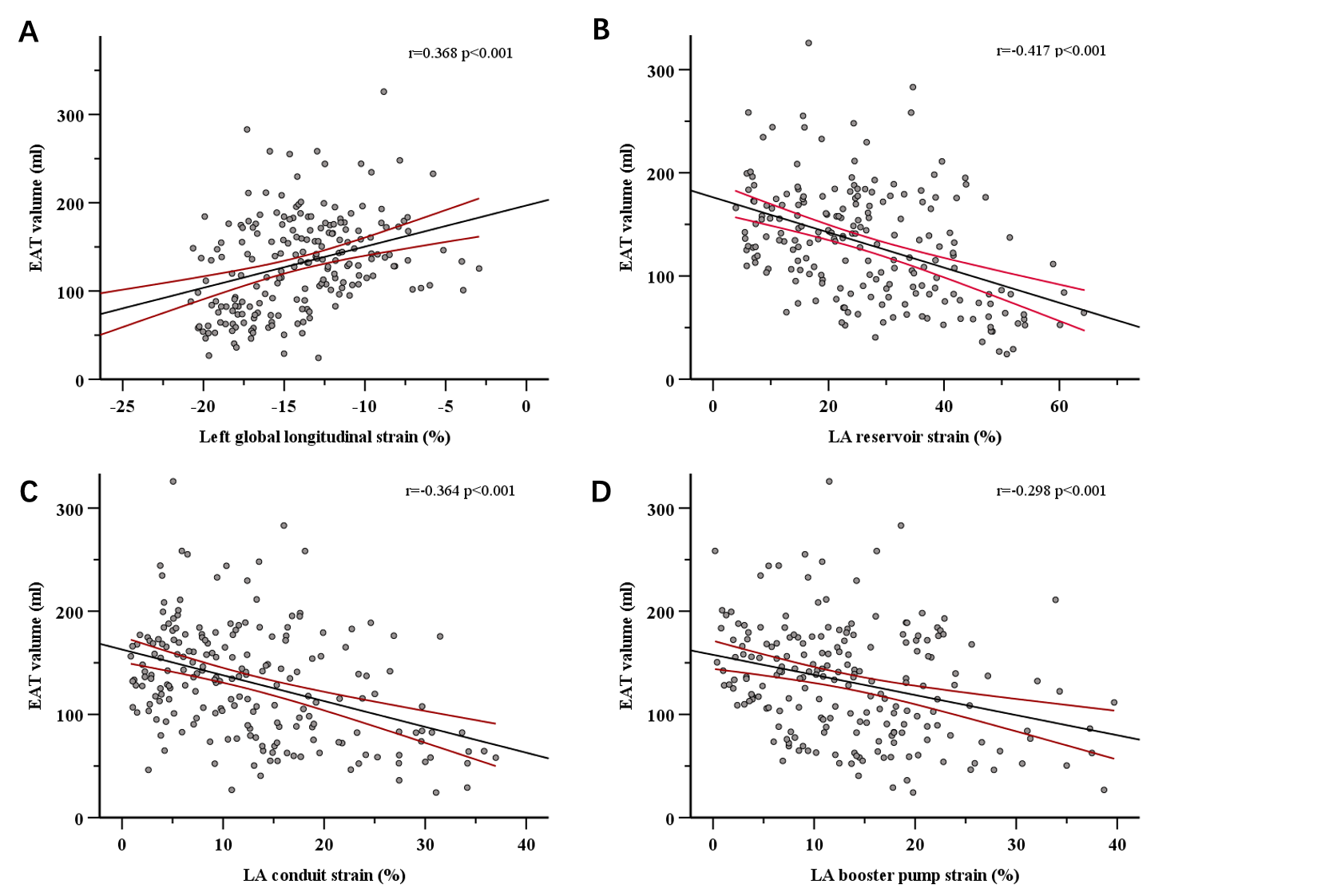
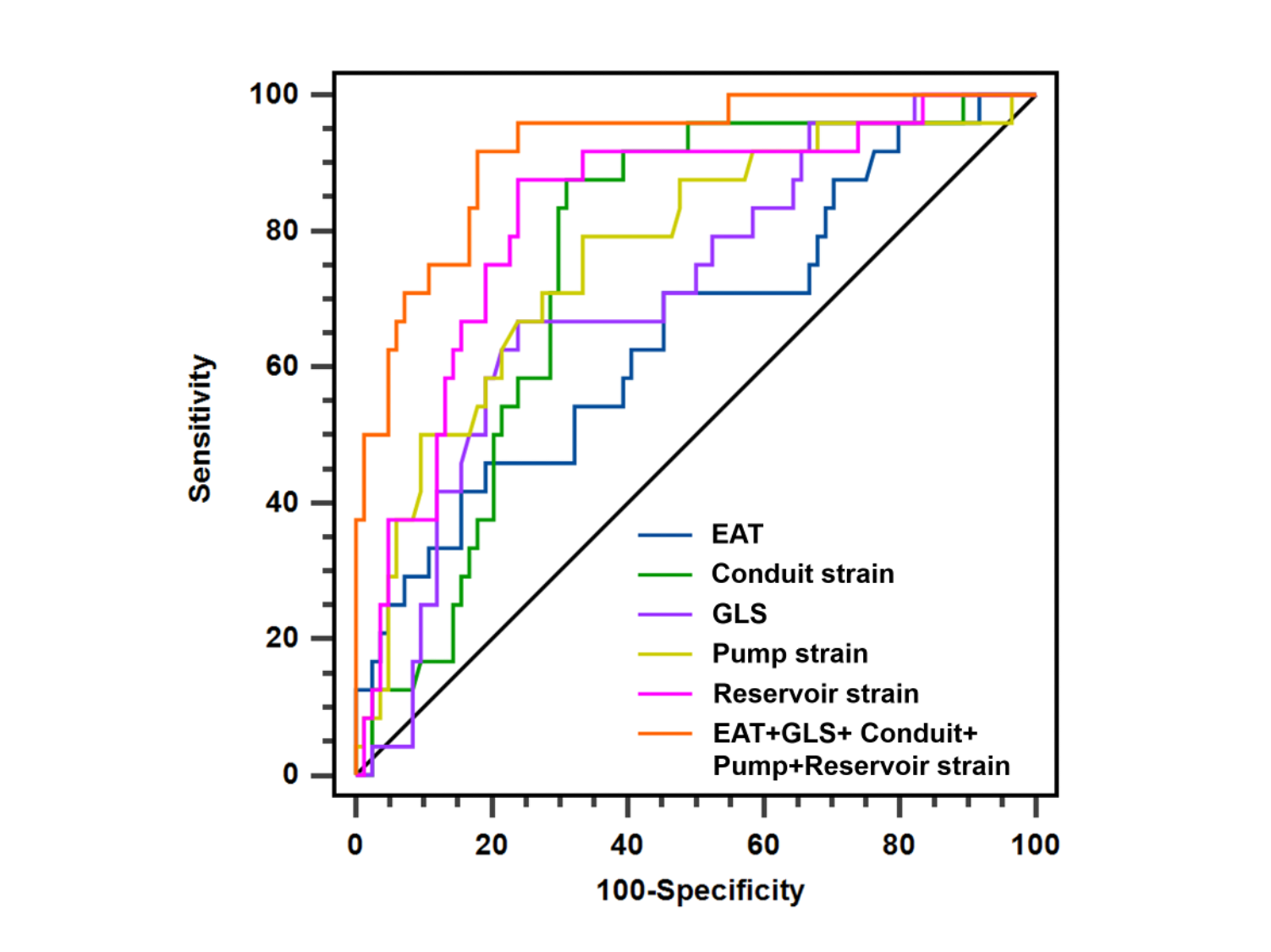
Figure 2: Receiver operating characteristic (ROC) curve analysis for EAT, GLS, LA reservoir strain, LA conduit strain, LA booster pump strain , and the combination to predict the presence of AF in HFpEF patients.
AF atrial fibrillation, EAT epicardial adipose tissue, GLS global longitudinal strain, HFpEF heart failure with preserved ejection fraction, LA left atrial volume index