1791
Association of pulmonary transit time by CMR with diastolic dysfunction and left ventricle deformation in restrictive cardiomyopathy1west china hospital, chengdu, China
Synopsis
Keywords: Myocardium, Cardiovascular
Motivation: Cardiopulmonary circulation usually present hemodynamic congestion in RCM patients. Pulmonary transit time (PTT) and pulmonary blood volume index (PBVi) are physiological parameters reflective of cardiopulmonary hemodynamics statue.
Goal(s): Evaluate the PTT and PBVi in RCM patients, and evaluated the association with LV function and deformation.
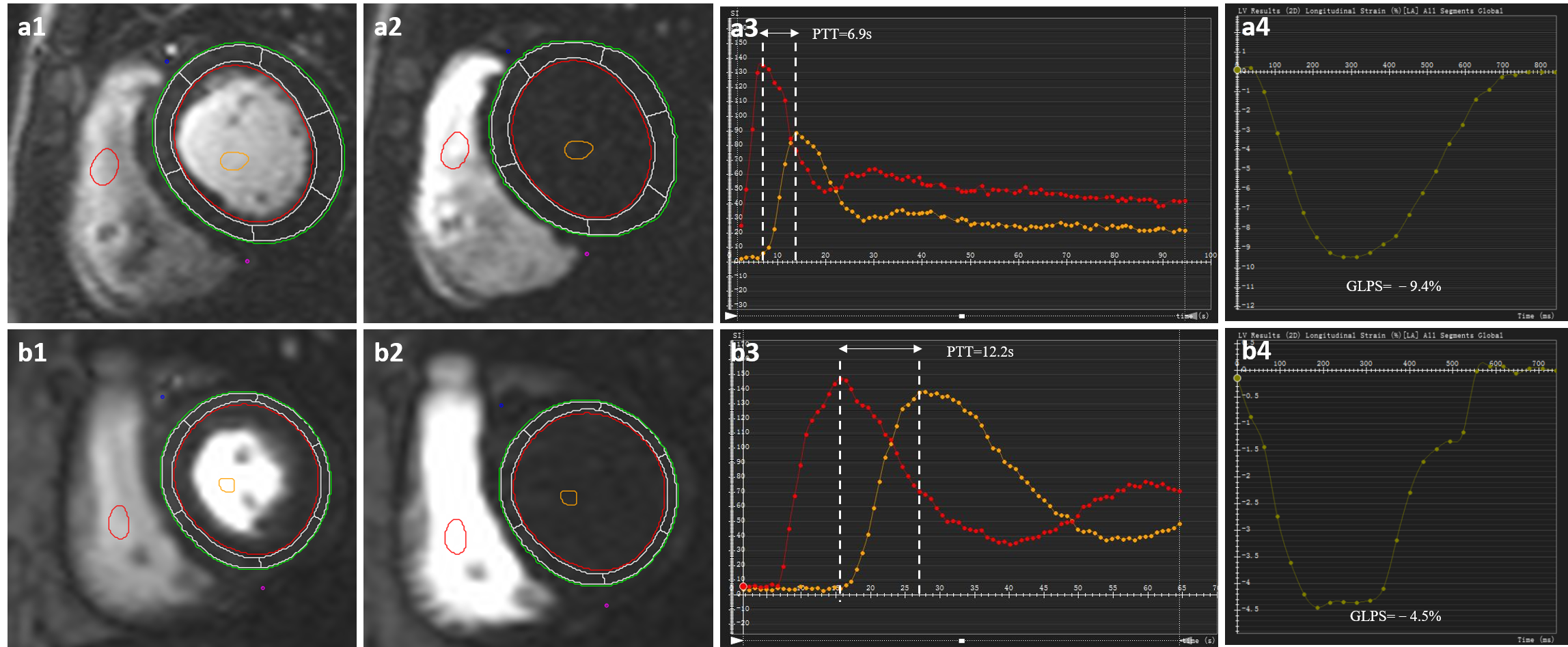
Approach: The images of first-pass perfusion were acquired to assess PTT which was normalized to heart rate. PBVi was measured by the product of PTT and RVSV and indexed to BSA.
Results: PTT showed independent association with LVEF and LVMVR, as well as with LV GCPS and GLPS; PBVi was an independent association of LVMI and LV GRPS.
Impact: PTTc and PBVi as the non-invasive marker of cardiopulmonary hemodynamics in patients with RCM, and reflects progression of diastolic dysfunction, and impaired LV global deformation. PTT and PBVI may provide additional information for prognostic management and clinical decision making.
RCM patients have a stiff LV with impaired diastolic filling and high filling pressures, which commonly induce pulmonary hypertension and tend to exacerbate heart failure (HF). For RCM patients the cardiopulmonary circulation usually presents hemodynamic congestion. Pulmonary transit time (PTT) and pulmonary blood volume index (PBVi) are physiological parameters reflective of cardiopulmonary hemodynamics status and have been considered to be related to cardiac dysfunction, pulmonary hypertension, and heart failure in previous studies. However, the relationship between PTT and PBVi and diastolic dysfunction in RCM remains unclear. In this study, we aimed to assess the PTT and PBVi in RCM patients, to determine whether PTT and PBVi reflect diastolic dysfunction and evaluated the association with LV function and deformation.
Methods:
One hundred thirty-seven RCM patients and 66 control subjects who underwent echocardiography and contrast-enhanced CMR(Trio Tim, Siemens Medical Solutions, Erlangen, Germany) were included. A comprehensive echocardiographic assessment of LV diastolic function. The dynamic images of first-pass perfusion were acquired to assess peak-to-peak PTT which was subsequently normalized to RR interval duration. PBV was measured by the product of PTT and the anterograde RVSV, and indexed to body surface area. The determinant of reduced LV global peak strain for all RCM patients was assessed using multivariable linear regression analyses.
Results:
PTT and PBVi were significantly higher in patients with RCM than in controls (8.85±2.71 vs. 6.03±1.39 sec, P<0.001; 257.91[179.65,340.94] vs. 218±70.63 mL/m2, P<0.001, respectively). PTT showed positive correlation with E/A ratio (r = 0.271, P = 0.00), PTT showed positive correlation with E/e’ ratio, E/A ratio and diastolic stage (r = 0.214, P = 0.012; r = 0.314, P <0.001; r = 0.195, P = 0.022; respectively). In multivariable analysis, PTTc showed independent association with LVEF and LVMVR (β = 0.472, 0.270, p = 0.001), as well as with LV GCPS (β = 0.299, p=0.001) and LV GLPS (β = 0.328, p < 0.001); PBVi was an independent association of LVMI (β = 0.283, p=0.001) and LV GRPS (β = -0.148, p=0.049).
Conclusion:
For patients with RCM, PTTc and PBVi as the non-invasive quantitative surrogate marker, is associated with diastolic dysfunction degree. The increase of PTTc and PBVi likely reflects impaired LV function and deformation, which may provide additional information for prognostic management and clinical decision-making in patients with RCM.
Acknowledgements
Not applicable.References
- Rapezzi C, Aimo A, Barison A, et al.: Restrictive cardiomyopathy: definition and diagnosis. Eur Heart J 2022; 43:4679–4693.
- Galea N, Polizzi G, Gatti M, Cundari G, Figuera M, Faletti R: Cardiovascular magnetic resonance (CMR) in restrictive cardiomyopathies. Radiol med 2020; 125:1072–1086.
- Muchtar E, Blauwet LA, Gertz MA: Restrictive Cardiomyopathy. Circulation Research 2017; 121:819–837. 8. Chintanaphol M, Orgil B-O, Alberson NR, Towbin JA, Purevjav E: Restrictive cardiomyopathy: from genetics and clinical overview to animal modeling. RCM 2022; 23:108.
- Ricci F, Barison A, Todiere G, et al.: Prognostic value of pulmonary blood volume by first-pass contrast-enhanced CMR in heart failure outpatients: the PROVE-HF study. European Heart Journal - Cardiovascular Imaging 2018; 19:896–904.
- Houard L, Amzulescu MS, Colin G, et al.: Prognostic Value of Pulmonary Transit Time by Cardiac Magnetic Resonance on Mortality and Heart Failure Hospitalization in Patients With Advanced Heart Failure and Reduced Ejection Fraction. Circulation: Cardiovascular Imaging 2021; 14:e011680.
- Pamminger M, Reindl M, Kranewitter C, et al.: Prognostic value of pulmonary transit time by cardiac magnetic resonance imaging in ST-elevation myocardial infarction. Eur Radiol 2023; 33:1219–1228. 15. Ait Ali L, Aquaro GD, Peritore G, et al.: Cardiac Magnetic Resonance Evaluation of Pulmonary Transit Time and Blood Volume in Adult Congenital Heart disease. Journal of Magnetic Resonance Imaging 2019; 50:779–786.
- Skrok J, Shehata ML, Mathai S, et al.: Pulmonary Arterial Hypertension: MR Imaging-derived First-Pass Bolus Kinetic Parameters Are Biomarkers for Pulmonary Hemodynamics, Cardiac Function, and Ventricular Remodeling. Radiology 2012; 263:678–687.
- Cao JJ, Nashta NF, Weber J, et al.: Association of pulmonary transit time by cardiac magnetic resonance with heart failure hospitalization in a large prospective cohort with diverse cardiac conditions. J Cardiovasc Magn Reson 2023; 25:57.
- Seraphim A, Knott KD, Menacho K, et al.: Prognostic Value of Pulmonary Transit Time and Pulmonary Blood Volume Estimation Using Myocardial Perfusion CMR. JACC: Cardiovascular Imaging 2021; 14:2107–2119.
Figures