1790
Cardiac magnetic resonance in subclinical primary cardiac involvement in systemic sclerosis1The First Medical Center of PLA General Hospital, Beijing, China, 2Philips Healthcare, Beijing, China
Synopsis
Keywords: Myocardium, Cardiovascular, SSc primary heart involvement, cardiovascular magnetic resonance,extracellular-volume fraction, modified Rodnan skin score
Motivation: Cardiac involvement is a significant cause of mortality in SSc. There are, however, no effective methods for detecting cardiac involvement in a general, asymptomatic SSc cohort.
Goal(s): We aimed to characterize and identify subclinical SSc-pHI by CMR.
Approach: 48 Patients underwent CMR, including cine imaging, LGE, T2 mapping, and native and post-contrast T1 mapping for ECV quantification.
Results: 56.25% of SSc-pHI patients had LGE, and 79.16% and 54.17% had native T1 and ECV above normal values. In addition, patients with dcSSc had worse contractility than patients with lcSSc, and contractile function is closely related to presence of RP, dcSSc, and ANA positive.
Impact: Cardiac magnetic resonance imaging provides a reliable method for detecting sub-clinical cardiac involvement in SSC patients. Patients with dcSSc had worse contractility than patients with lcSSc, and contractile function is closely related to presence of RP, dcSSc, and ANA positive.
Introduction
Subclinical systemic sclerosis (SSc) is a heterogeneous immune-mediated rheumatic disease characterized by progressive fibrosis of the skin and visceral organs and excessive extracellular matrix deposition1. The previous research has been demonstrated that the prevalence of SSc-primary heart involvement (SSc-pHI) between 15% and 35%2, which is associated with poor prognostic. However, effective means of early detection of cardiac involvement in a general, asymptomatic SSc cohort are lacking. Currently, advancements in cardiac magnetic resonance (CMR) technology, such as feature tracking technology, have enabled the objectively and quantitatively evaluation of myocardial deformation. T1 mapping based on cardiovascular magnetic resonance (CMR) is a novel technique, which can calculate extracellular-volume fraction (ECV) by measuring the T1 of myocardium before and after contrast quantifying early, slight. and invisible myocardial fibrosis in SSc patients. In addition, CMR T2 mapping also could quantify diffuse myocardial edema by measuring the T2 of the myocardium. We aim to characterize SSc-pHI through multi-parameters CMR and explore the relationship between SSc-pHI and clinical parameters.Method
48 Patients were recruited to this study fulfilled the 2013 ACR/ EULAR criteria for SSc3 and were classified as local SSc (lcSSc) or diffuse SSc (dcSSc) according to LeRoy classification 4. Patients were excluded if they had any prior diagnosis of ischaemic heart disease (IHD) (or clinically overt SSc-pHI), diabetes, or more than two traditional CV risk factors. A rheumatologist with more than ten years of work experience blinded to CMR data scored the patient's skin involvement by mRSS. Patients underwent CMR on a 3 Tesla CMR (Ingenia, Philips Healthcare, best, the Netherlands), including cine imaging for left ventricle (LV) function estimation, Late gadolinium enhancement (LGE), T2 mapping, and native and post-contrast T1 mapping for ECV quantification, which enabled quantitative assessment of myocardial fibrosis. 50 patients with complete CMR function assessment, LGE, T1, ECV, and T2 mapping available were recruited finally. The LGE (presence or absence) was identified by a consensus agreement among 2 radiologists who were experienced in CMR and blinded to clinical outcome. According to the departmental reference ranges, an ECV >29% and native T1 > 1240 (ms) were classed as abnormal5,6.Results
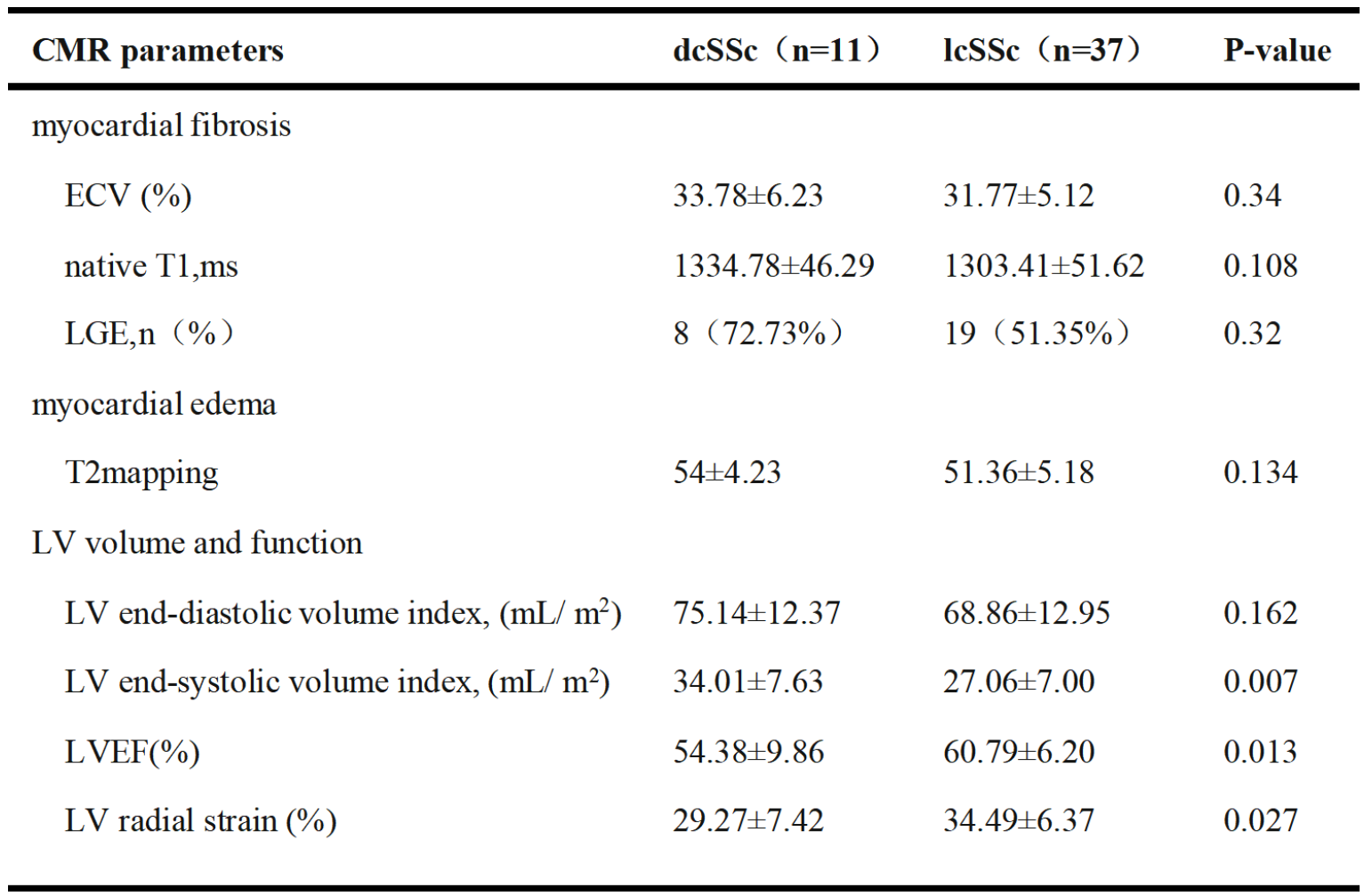
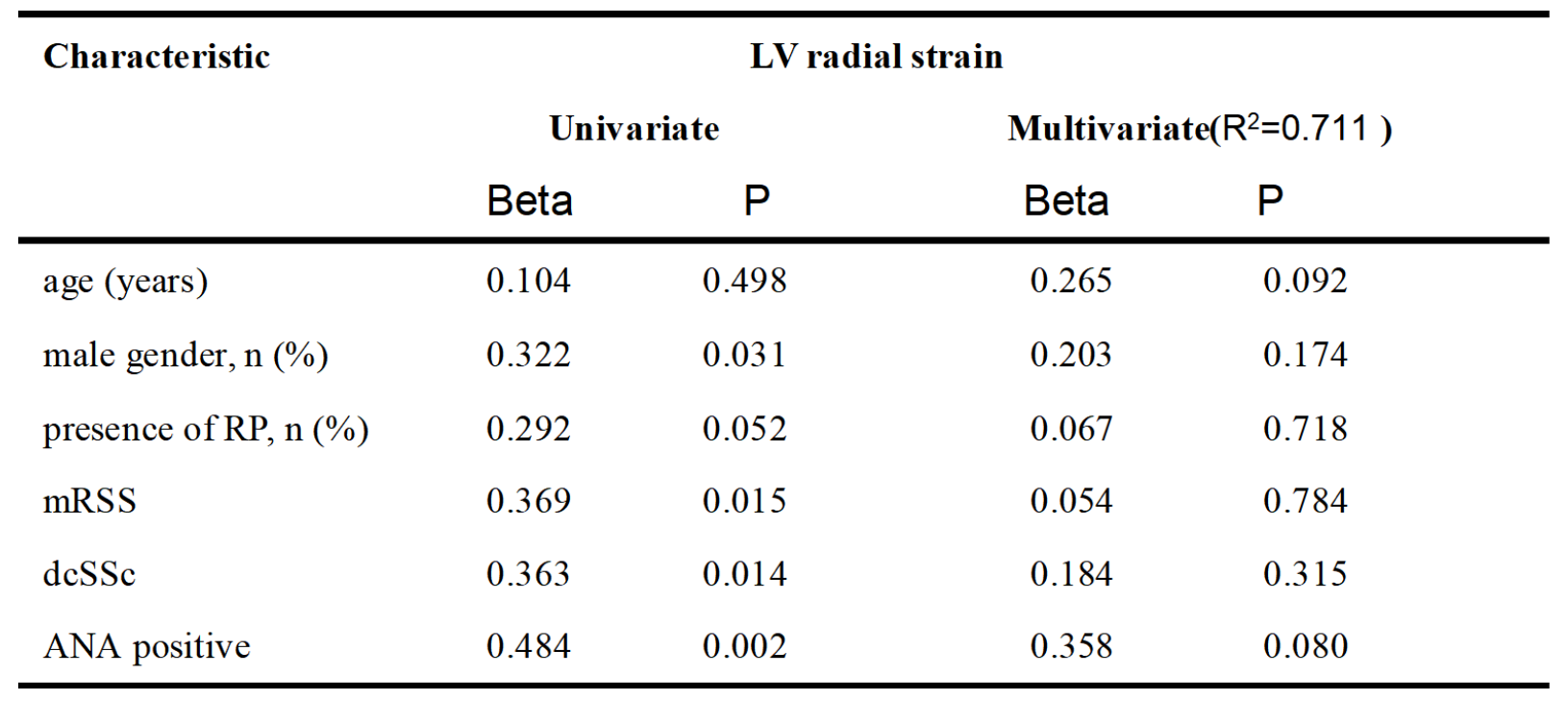
In total, 48 consecutive patients were recruited and 22.9% had diffuse SSc. And patients with dsSSc had significantly higher mRSS compared with lcSSc [median (IQR) 16 (6–35) vs. 3 (3–6), P < 0.001]. For LGE, a total of 27 (56.25%) SSc patients had focal LGE fibrosis in a non-ischaemic pattern. And, a total of 38 (79.16%) and 26 (54.17%) SSc patients, respectively, had native T1 and ECV above normal values. In patients with dcSSc, there was a significantly higher LV end-systolic volume index (ESVI) (34.01±7.63 mL/m2 vs 27.06±7.00 mL/m2; P =.007) compared to those with lcSSc. Additionally, dcSSc patients exhibited significantly lower LV EF (54.38±9.86% vs 60.79±6.20%; P =.013), and LV RS (29.27±7.42% vs 34.49±6.37%; P =.027). Native T1, ECV, and T2 value of the group with dcSSc were also higher than that of the group with lcSSc but did not reach statistical significance. Male gender, presence of RP, dcSSc, and ANA positive were found to be independently associated with LV radial strain in the univariate analysis.Discussion
CMR enables comprehensive assessment of cardiac morphology, function, and tissue characteristics to detect subclinical SSc-PHI. The study demonstrated that the native T1 and ECV of groups with diffuse SSc had significantly higher than that of groups with lcSSc, indicating interstitial fibrosis is more serious in diffuse SSc. Correspondingly, patients with dcSSc had worse contractility than patients with lcSSc, and contractile function is closely related to presence of RP, dcSSc, and ANA positive.Conclusion
Cardiac magnetic resonance imaging provides a reliable method for detecting sub-clinical cardiac involvement in SSC patients.Acknowledgements
noneReferences
1.Ferri C, Valentini G, Cozzi F et al. Systemic sclerosis: demographic, clinical, and serologic features and survival in 1,012 Italian patients. Medicine 2002;81: 139–532.Tyndall AJ, Bannert B, Vonk M et al. Causes and risk factors for death in systemic sclerosis: a study from the EULAR Scleroderma Trials and Research (EUSTAR) database. Ann Rheum Dis 2010;69:1809–15.3.van den Hoogen F, Khanna D, Fransen J et al. classifification criteria for systemic sclerosis: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann Rheum Dis 2013;72:1747–55. 4.LeRoy EC, Black C, Fleischmajer R et al. Scleroderma (systemic sclerosis): classifification, subsets and pathogenesis. J Rheumatol 1988;15:202–5.5. Dabir D, Child N, Kalra A et al. Reference values for healthy human myocardium using a T1 mapping methodology: results from the International T1 Multicenter cardiovascular magnetic resonance study. J Cardiovasc Magn Reson 2014;16:69. 6. McDiarmid AK, Swoboda PP, Erhayiem B et al. Athletic cardiac adaptation in males is a consequence of elevated myocyte mass. Circ Cardiovasc Imaging 2016; 9:e003579.Figures