1788
Radiomics feature based discrimination between aortic flow profiles in HFpEF and healthy controls using 2D Flow MRI1Deutsches Herzzentrum der Charité, Berlin, Germany, 2Partner Site Berlin, - DZHK (German Center for Cardiovascular Research), Berlin, Germany, 3Partner Site Berlin, DZHK (German Center for Cardiovascular Research), Berlin, Germany, 4DZHK (German Center for Cardiovascular Research), Berlin, Germany, 5Fraunhofer MEVIS, Berlin, Germany
Synopsis
Keywords: Flow, Heart, Heart failure, ejection fraction, radiomics
Motivation: HFpEF (heart failure with preserved ejection fraction) patients show similar diagnostic parameter values to healthy subjects in the quantitative evaluation of cardiac magnetic resonance imaging (CMR). Improving the performance of CMR-based HF characterization is desirable.
Goal(s): Evaluation of radiomics features from 2D flow MRI of the aorta for the classification into healthy, HFpEF, HFmrEF (mildly reduced) and HFrEF (reduced).
Approach: Training and evaluation of a decision tree classifier using 70 CMR datasets with conventional diagnostic parameters and 2D flow radiomics features to find relevant flow descriptors.
Results: The classifier achieved excellent results, considering the local flow homogeneity during diastole.
Impact: We evaluate adding 2D flow MRI radiomics to standard EF measurements for the classification of heart failure subtypes. This would enable the diagnosis of the subtypes with one imaging modality without the need for stress testing.
Challenges in the diagnosis of heart failure with preserved ejection fraction
The diagnosis or heart failure with preserved ejection fraction (HFpEF) according to current guidelines is challenging and requires a combined evaluation of laboratory and echocardiography-based parameters [1]. MRI has been suggested as a secondary tool for the analysis of left ventricular systolic function to confirm left atrial enlargement and left ventricular hypertrophy [2]. Tanacli et al. found that MRI-based strain analysis can further improve the diagnosis of HFpEF [3]. Previous study found an association between aortic stiffness and the development of HFpEF in patients with asymptomatic diastolic dysfunction [4]. Therefore, we evaluate the potential of dynamic shape and texture analysis of 2D Flow MRI of the ascending aorta for the discrimination between HFpEF, heart failure with mildly reduced (HFmrEF) and reduced (HFrEF ) ejection fraction and healthy controls.Methods
We analyzed 70 datasets from the EMPATHY-HF trial (https://drks.de/search/en/trial/DRKS00015615) consisting of 18 healthy controls (9 female, age [48,77], av. EF 64), and 52 HF patients: 22 HFpEF (11 female, age [54,88], av. EF 60), 16 HFmrEF (3 female , age [46,79], av. EF 44), 14 HFrEF (3 female , age [47,75], av. EF 32).Images were acquired with a Philips Achieva 1.5T scanner:
- Short axis cine sequences: repetition time 2.54, echo time: 1.27, slice thickness: 10mm, flip angle: 60, inplane resolution: 1.63mm², 25 timeframes/heartcycle
- Flow sequences: repetition time 3.69, echo time: 2.21, slice thickness: 10mm, flip angle: 15, inplane resolution: 1.37mm², 35 timeframes/heartcycle, velocity encoding>= 250cm/s
For normalization, velocities in the range of [-600 cm/s, 600 cm/s] were rescaled to [-2047, 2048] for quantization for the pyradiomics (v3.0.1) library [5]. Features were extracted for the systolic timeframe (max. netflow) and the end-diastolic timeframe (last before increase of netflow). We trained a decision tree classifier using the ejection fraction (EF) from cine MRI and the flow radiomics features for systole and end- diastole to detect the four classes.
Classifier performance and feature relevance
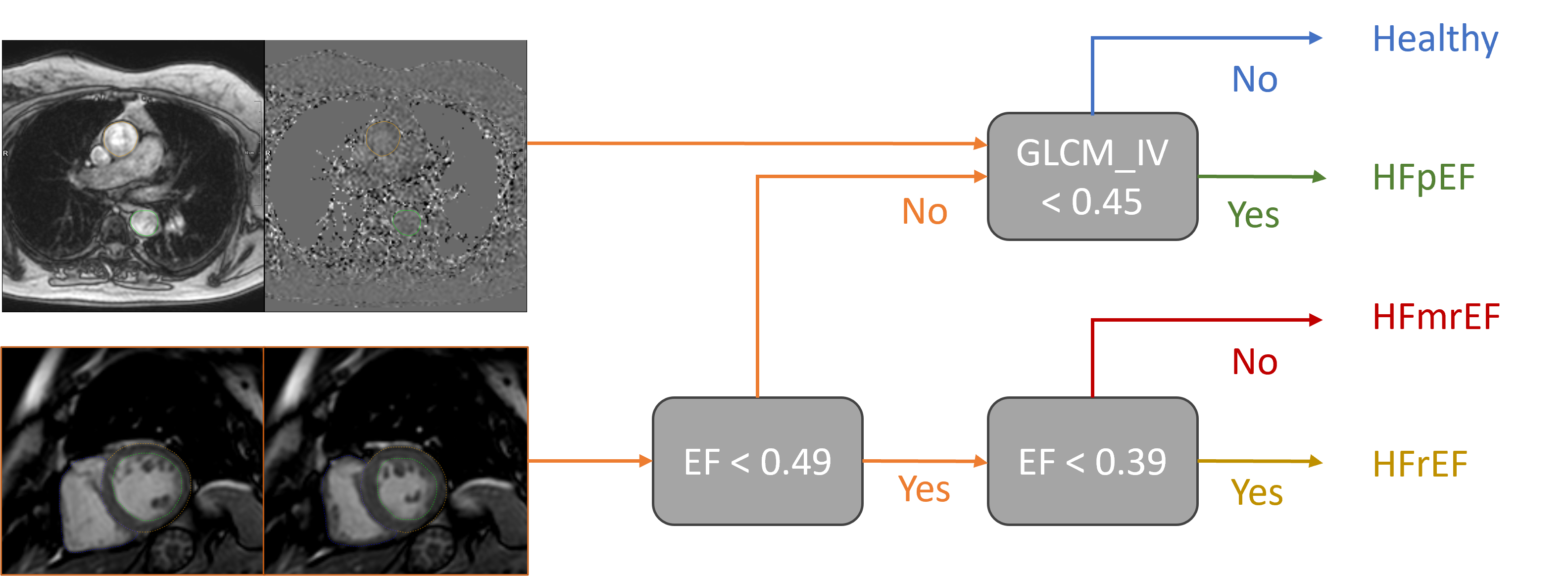
10-fold cross validation of the classifier achieves the following mean performance measures: accuracy 0.93, AUC 0.95, recall 0.93, precision 0.89, F1 0.91, kappa 0.90, Matthews correlation coefficient (mcc) 0.92. The SHAP feature importance analysis showed that the EF and the inverse variance of the grey level co-occurrence matrix (GLCM_IV) contribute most to the classification.$$GLCM_{IV}= \sum_{v_{diff}=1}^{maxdiff}\frac{p_{v1-v2}(v_{diff})}{v^2_{diff}}$$
The value of $$$p_{v1-v2}(v_{diff})$$$ represents the number of co-occurrences of neighboring voxels with a velocity difference of $$$v_{diff}$$$. The corresponding decision tree is shown in Figure 1.
Discussion
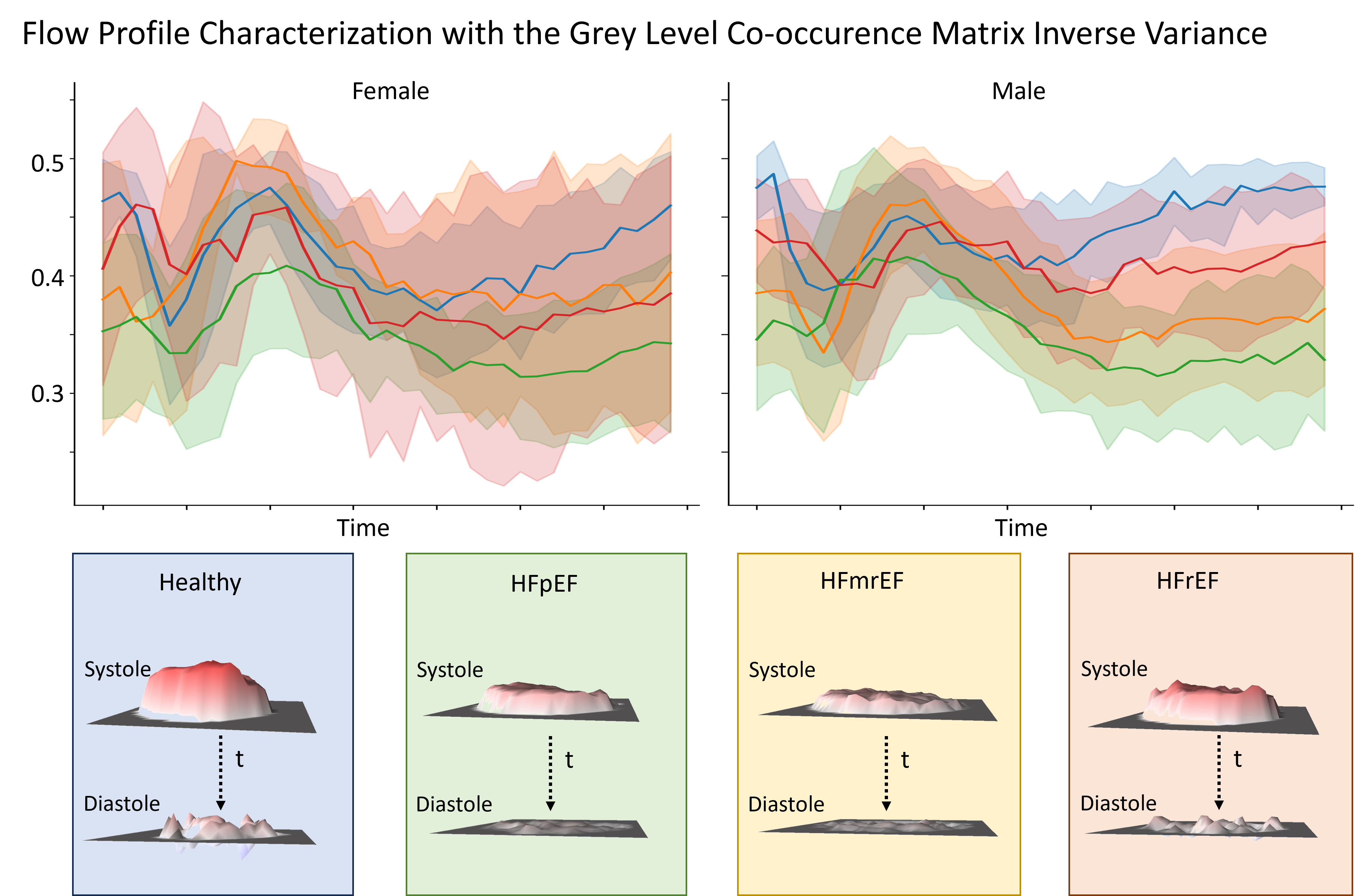
The classes Healthy, HFmrEF and HFrEF are defined via the EF, and the classifier learns the expected threshold configuration. Figure 2 shows the average feature curves and value ranges for the grey level co-occurrence matrix inverse variance (GLCM_IV) feature for all timeframes. There is a minimal overlap between the diastolic values of healthy subjects and HFpEF patients in women. For men, the corresponding value ranges show no overlap.The exemplary flow profiles illustrate the meaning of the feature values. GLCM_IV quantifies the local flow homogeneity which clearly differs between the healthy profile and the HFpEF examples
Conclusion
We tested the potential of radiomics based flow profile characterization as an additional method for the image-based discrimination of HF subtypes and achieved a good performance with a decision tree classifier. Future work will investigate the 3D flow patterns that cause the observed flow profile patterns with 4D flow MRI, and analyze the relationship with aortic compliance.Acknowledgements
This work was funded by the DFG as part of the Collaborative Research Center 1470 B06 - Imaging structure/function relations in HFpEF – from pathomechanisms to artificial intelligence-based classificationReferences
- Pieske, B., et al., How to diagnose heart failure with preserved ejection fraction: the HFA-PEFF diagnostic algorithm: a consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur Heart J, 2019. 40(40): p. 3297-3317.
- Assadi, H., et al., Cardiac MRI for the prognostication of heart failure with preserved ejection fraction: A systematic review and meta-analysis. Magn Reson Imaging, 2021. 76: p. 116-122.
- Tanacli, R., et al., Multilayer myocardial strain improves the diagnosis of heart failure with preserved ejection fraction. ESC Heart Fail, 2020. 7(5): p. 3240-3245.
- Karagodin, I., et al., Aortic stiffening precedes onset of heart failure with preserved ejection fraction in patients with asymptomatic diastolic dysfunction. BMC Cardiovasc Disord, 2017. 17(1): p. 62.
- van Griethuysen, J.J.M., et al., Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res, 2017. 77(21): p. e104-e107.
Figures