1787
Deep learning based reconstruction 3D ZTE-MRI for calcium deposit using computed tomography as reference1GE Healthcare, Guangzhou, China, 2Department of Radiology, Renmin Hospital of Wuhan University, Wuhan, China, 3Renmin Hospital of Wuhan University, Wuhan, China
Synopsis
Keywords: Atherosclerosis, Kidney, chronic kidney disease, zero echo time, deep learning
Motivation: Screening opportunity might increase detection of calcium presence in cardiac tissues. Calcium deposit in cardiac tissues especially vessels alter flow hemodynamics. A non-invasive zero echo time magnetic resonance imaging (ZTE-MRI) may offer additional information when patients receive routine cardiac magnetic resonance imaging (CMR).
Goal(s): To propose a three-minute, high-resolution, high-SNR free-breathing ZTE-MRI in detection of coronary artery calcification.
Approach: To subjectively and objectively evaluation of ZTE-MRI respectively using conventional and deep learning reconstruction using CT as reference.
Results: DLR ZTE-MRI had superior image quality to noDLR ZTE-MRI and showed fair to good performance on calcium deposit by visual observation.
Impact: DLR ZTE-MRI with the featurs of fee-radiation, silence, and comfort (free-breathing) during scan can provide extra information – calcium deposite, for whoever, especially a CKD patient, plans to receive a physical examination especially CMR examinaition.
Introduction
The incidence of atherosclerosis, a common and frequently-occurring cardiovascular diseases (CVD), is observed in younger patients, especially in the CKD population, possibly attributing to systemic calcium/phosphate imbalance, vascular endothelial injury, inflammation, and uremic toxicity. Calcium area and volume are positively associated with atherosclerotic plaque area and volume. [16, 54]. Coronary artery calcium (CAC) can be detected by computed tomography (CT) and multi-detector computed tomography (MDCT) and is potentially helpful to identify asymptomatic individuals at increased risk for cardiovascular events [1–4]. A novel sequence zero echo time (ZTE) MRI can acquire inherent short-T2 bone and lung signal that cannot be acquired by conventional MRI sequences and provide CT-like image for diagnosis [5-9]. Opportunistic screening is of importance, and to implant an essential even not a routine imaging in clinical practices may help for early detection of calcium that greatly affect prognosis of aorta, coronary artery and all other vessels. This study aimed to explore the feasibility of a rapid and high-resolution ZTE-MRI scan in detection of calcium deposit.Methods
15 CKD patients underwent a free-breathing 3D radial ZTE sequence on a 3.0T (Signa Architect, GE Healthcare) using the following parameters: FOV = 32 cm, frequency = 320, spokes per segment = 256, slice thickness = 1 mm, number of excitations = 2, scan time = 3 minutes 53 second). Acquired k-space data was reconstructed by conventional method and DLR, respectively. The overall image quality was independently evaluated by two radiologists with more than 5 years of experience in the diagnosis of cardiovascular diseases using the Likert five-point scale (5, Excellent: no motion-related artifacts or image distortion; 4. Good: slight motion-related artifacts or image distortion; 3. Qualified for diagnostic requirements: moderate motion-related artifacts or image distortion, but sufficient for diagnosis; 2. fair: there are obvious motion-related artifacts or image distortion, but some can be diagnosed; 1. Unable to diagnose: can not meet the clinical diagnosis requirements) Images with scores between 2 and 5 are considered to meet diagnostic requirements. Manually drawn region-of-interests (ROIs) were positioned on calcium, muscle and background on the slice of the most obvious calcium. Based on a previous study [7], signal-to-noise ratio (SNR) was calculated as mean signal intensity of calcium to standard deviation of background signal intensity whereas contrast-to-noise (CNR) was calculated as difference of mean signal intensity of calcium and muscle to standard deviation of muscle signal intensity.Results
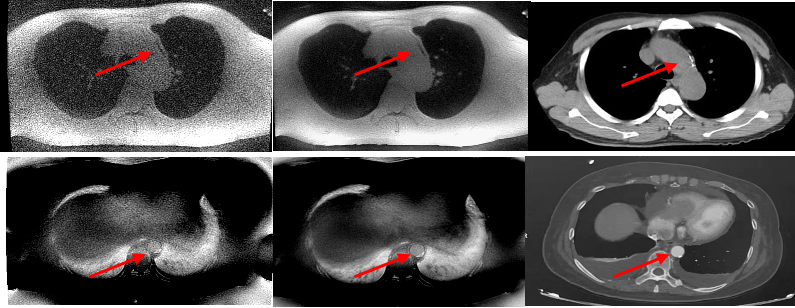
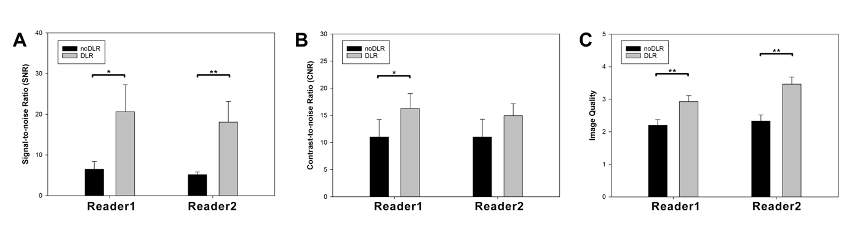
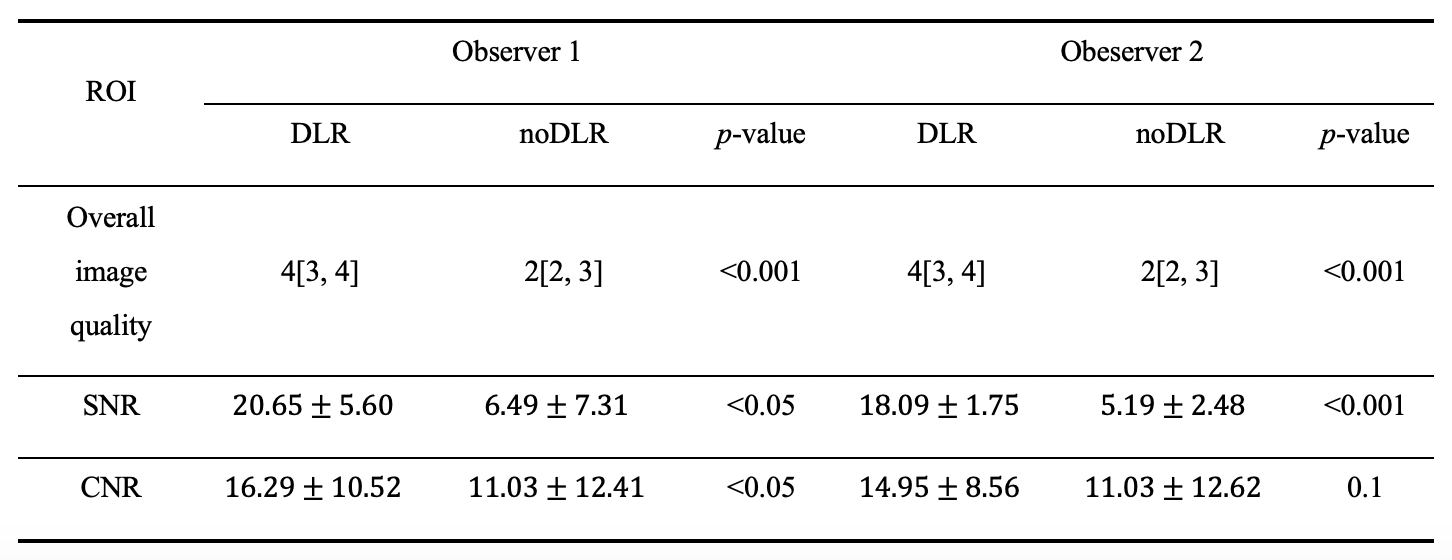
DLR and conventional reconstructed ZTE images of two CKD patient are demonstrated in Figure. 1. Dramatically reduced noise and improved calcium clarity can be see on DLR-ZTE images. For subjective evaluation, overall image quality was statistically improved on DLR-ZTE images, and there was good observer agreement on overall image quality of DLR and noDLR ZTE images (ICC = 0.865 and 0.701, p<0.05). For objective evaluation, significantly increased SNR and CNR values (only one observer 1) of DLR images can be observed in measurements performed by two observers.Discussion
Calcium deposit was clearly visulized on silent and free-breathing DLR-ZTE MRI compared to CT images. For a CKD patients, a comprehensive MRI examination is required for not only financial burden but also whole-body organ deterioration as repeated dialysisA high CAC burden has been associated with atrial fibrillation, extra coronary atherosclerosis, increased risk of cere-brovascular events, and an unfavorable CVD risk profile.[1-2] Our results suggested to undergo one more ZTE-MRI sequence on CKD patients in reflection of the extent of calcium deposit, hinting to both the patients and the clicians being aware of increased risk of CVD. At present, it is know that subclinical atherosclerosis and calcium buildup may provoke platelet activation through various pathways, contributing to higher thrombosis risk. Therefore, ZTE-MRI may give an image evidence to laboratory data especially including platelets, uric acid, calcium, and phosphorus due to a possible relationship between increased vessel calcium burden, platelet activation, and higher thrombotic and atherosclerotic risk.Conclusion
With the help of DLR, ZTE-MRI provide higher image quality and fair detection rate of calcium deposit in CKD patients.Acknowledgements
No acknowledgement found.References
[1] Neeland IJ, Ross R, Després JP, et al. Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: a position statement. Lancet Diabetes Endocrinol. 2019;7(9):715–725.
[2] Shoji T, Abe T, Matsuo H, et al. Chronic kidney disease, dyslipidemia, and atherosclerosis. J Atheroscler Thromb. 2012;19(4):299–315.
[3] Zalba G, Fortuño A, Díez J. Oxidative stress and atherosclerosis in early chronic kidney disease. Nephrol Dial Transplant. 2006;21(10):2686–2690.
[4] Swaminathan S, Shah SV. Novel inflammatory mechanisms of accelerated atherosclerosis in kidney disease. Kidney Int. 2011;80(5):453–463.
[5] Wiesinger F, Sacolick LI, Menini A et al (2016) Zero TE MR bone imaging in the head. Magn Reson Med 75:107-114
[6] Breighner RE, Endo Y, Konin GP, Gulotta LV, Koff MF, Potter HG (2018) Technical Developments: Zero Echo Time Imaging of the Shoulder: Enhanced Osseous Detail by Using MR Imaging. Radiology 286:960-966
[7] Weiger M, Pruessmann KP (2019) Short-T(2) MRI: Principles and recent advances. Prog Nucl Magn Reson Spectrosc 114-115:237-270
[8] Bae, K., et al., Comparison of lung imaging using three-dimensional ultrashort echo time and zero echo time sequences: preliminary study. Eur Radiol, 2019. 29(5): p. 2253-2262.
[9] Meier-Schroers, M., et al., Lung cancer screening with MRI: Evaluation of MRI for lung cancer screening by comparison of LDCT- and MRI-derived Lung-RADS categories in the first two screening rounds. Eur Radiol, 2019. 29(2): p. 898-905.
Figures