1786
Sensitivity of cardiac 31P MRSI in prone and supine positions using an integrated 31P whole-body transmit coil at 7T1Center for image Sciences, University Medical Center Utrecht, Utrecht, Netherlands
Synopsis
Keywords: Myocardium, Spectroscopy, RF Coils, Metabolism
Motivation: Cardiac 31P MRS is limited by the low sensitivity of commonly used transmit-receive surface coils at larger distances from the coil. Therefore, with transmit-receive surface coils, data is often acquired in prone position, which brings the heart closer to the coil.
Goal(s): Determine the sensitivity of cardiac 3D 31P MRSI in prone and supine positions using an integrated 31P whole-body birdcage transmit coil at 7T.
Approach: A male and female subject were scanned in prone and supine position.
Results: 3D 31P MRSI data were obtained with good sensitivity throughout the whole heart, regardless of the position of the subject.
Impact: With an integrated 31P whole-body transmit coil at 7T, cardiac 31P MRS can be performed in the more comfortable supine position, with good sensitivity also in the posterior cardiac wall.
Introduction
Metabolic stress can impair myocardial energy balance, affecting cardiac performance and contributing to cardiomyopathy. Phosphorus-31 magnetic resonance spectroscopy (31P MRS) allows non-invasive assessment of cardiac energy status by detecting adenosine triphosphate (ATP) and phosphocreatine (PCr).1 While clinical field strengths of 1.5T and 3T are preferred for myocardial structure and function assessment, precise quantification of cardiac PCr and ATP by 31P MRS benefits from the increased signal-to-noise ratio (SNR) and spectral resolution at 7T.2,3 Moreover, clinical applications of cardiac 31P MRS are limited by the low sensitivity of commonly used transmit-receive surface radiofrequency coils at larger distances from the coil.4 To address the latter, cardiac 31P MRS studies are often performed in prone position, which brings the heart closer to the coil but which can be less comfortable.Here we show the application of an integrated 31P whole-body birdcage transmit coil, with homogeneous excitation over a large field-of-view (FOV),5 in combination with a 16-channel 31P body receive array for cardiac 31P MRSI at a field strength of 7T. The aim of the study was to compare the sensitivity of cardiac 3D 31P MRSI in prone and supine positions using this setup.
Methods
Measurements were performed on a 7T whole-body MR system (Philips Healthcare, Best, the Netherlands), equipped with a shielded 31P whole-body birdcage transmit coil with a diameter of 60cm and a length of 40cm, embedded in the outside of the patient tube.4 31P signals were received with a local body array, containing 16 31P loop coils and 8 fractionated 1H dipole antennas.6,7A 31P B1+ map was acquired on a body size phantom containing 3g/L NaCl and 43mM KH2PO4, using the actual flip angle imaging (AFI) method8 (3D gradient echo: FOV=480×300×300mm3, resolution=20×20×20mm3, TE=1.75ms, TR1=50ms, TR2=950ms, nominal flip angle=60°, reference B1+=10µT, NSA=64). B1+ maps were reconstructed using QMRITools.9
Two healthy volunteers (one male with BMI 21.0kg/m2, one female with BMI 24.6kg/m2) were scanned in prone and supine position. Image-based B0 shimming was performed during a breath hold and transversal and coronal anatomical images were acquired with a T1-FFE sequence. 31P spectra were acquired with a 3D FID-MRSI sequence with Hamming weighted k-space sampling without respiratory gating or cardiac triggering, using a block pulse for excitation (carrier frequency set to PCr, B1+=10μT). The following parameters were used: FOV=500(LR)×280(AP)×360(FH)mm3, nominal resolution=20mm isotropic, TR=60ms, acquisition delay=0.50ms, BW=5000Hz, NSA=20, acquisition time=22:37min. 31P MRSI data were reconstructed in MATLAB (The MathWorks Inc., Natick, MA) using whitened singular value decomposition (WSVD)10 and PCA-based denoising.11 SNR was calculated based on the intensity of the α-ATP signal in the spectral domain by dividing the signal intensity of the α-ATP peak by the standard deviation of the noise (10-20 ppm). Nine metabolite signals were fitted with AMARES12 using OXSA13, from which PCr/γ-ATP ratios (not corrected for saturation or blood contamination) were determined.
Results
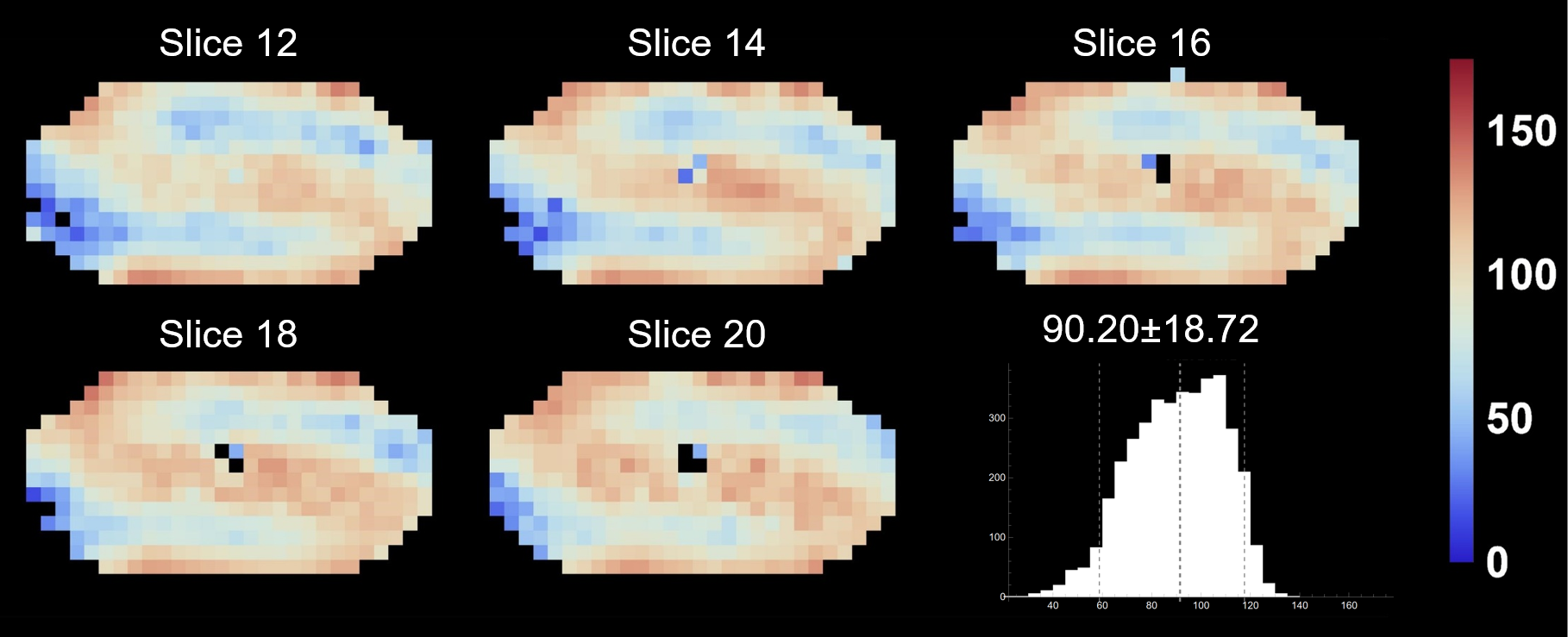
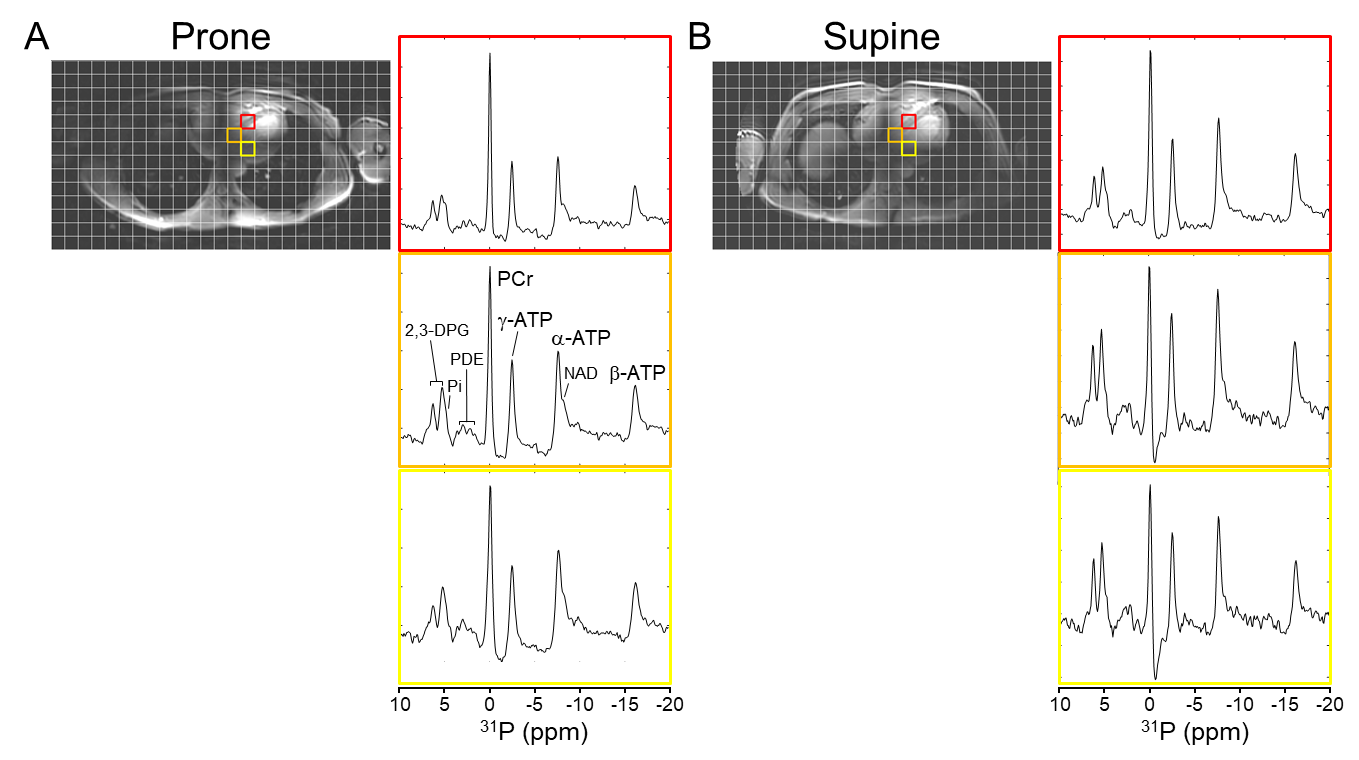
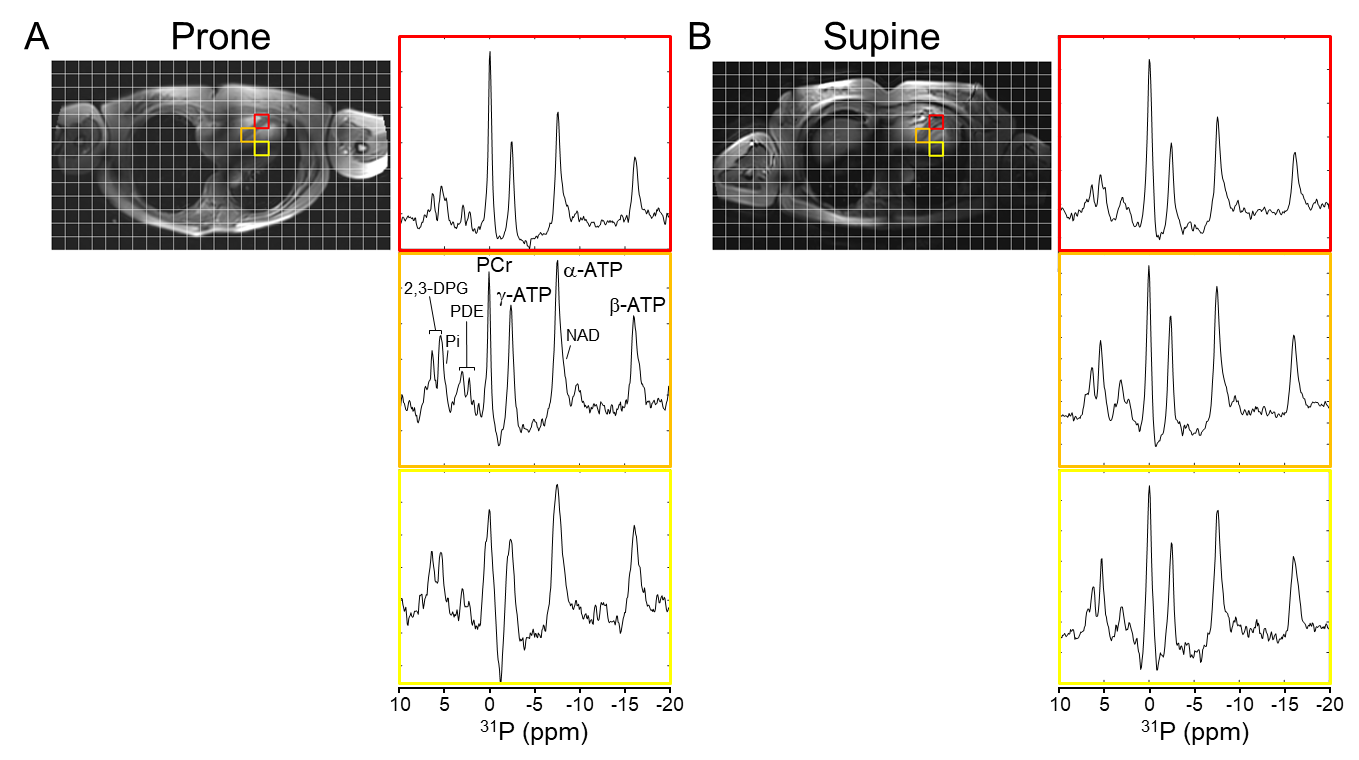
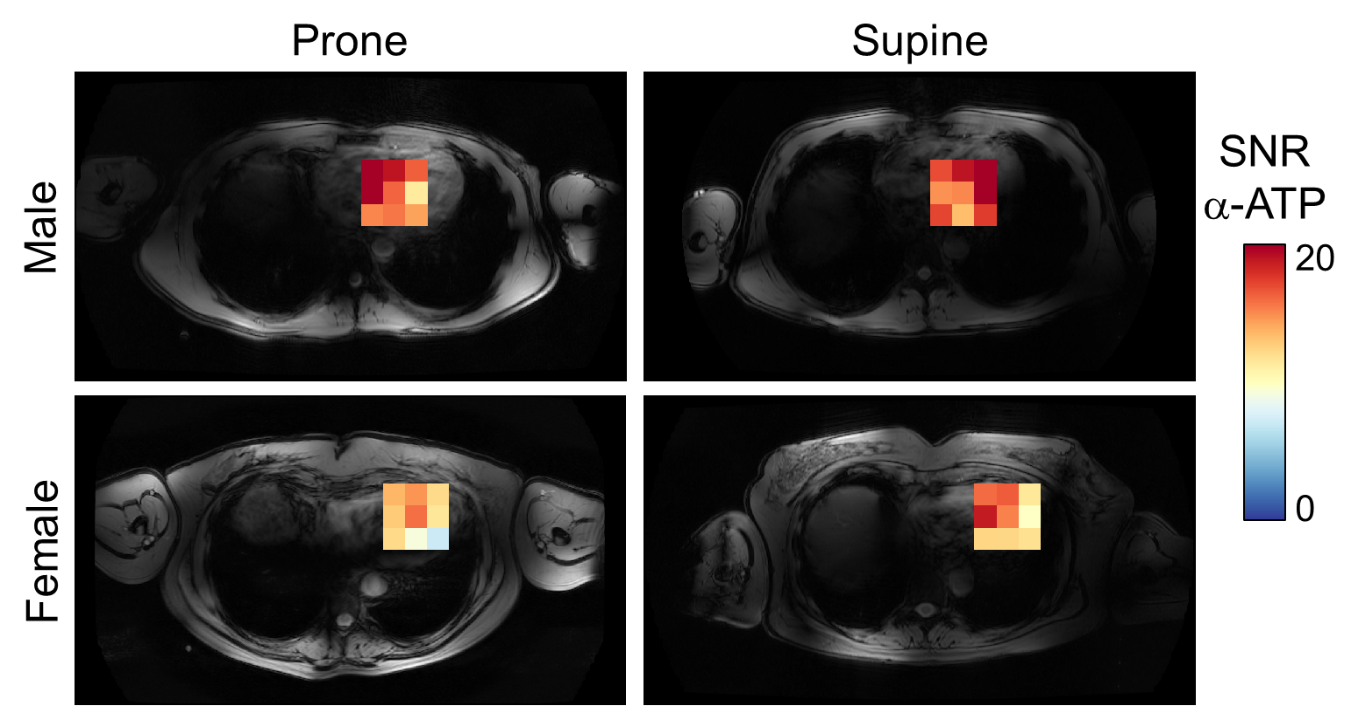
Figure 1 shows B1+ maps of the 31P whole-body birdcage transmit coil. Over the whole phantom, the variation of B1+ (coefficient of variation=SD/mean) was 21%.Figures 2 and 3 show 31P MRS spectra from three voxels in the myocardial wall, at different depths, from the datasets recorded in prone and supine position, in the male and female volunteer, respectively. Spectral quality was similar for prone and supine positions, but SNR decreased slightly when going from the most anterior (red) to the most posterior (yellow) voxel for both positions, for both subjects. The slight SNR drop in the anterior-posterior direction (factor 1.2-1.4) is also apparent from the cardiac α-ATP SNR maps (Figure 4) and reflects the sensitivity profile of the 31P receive array.
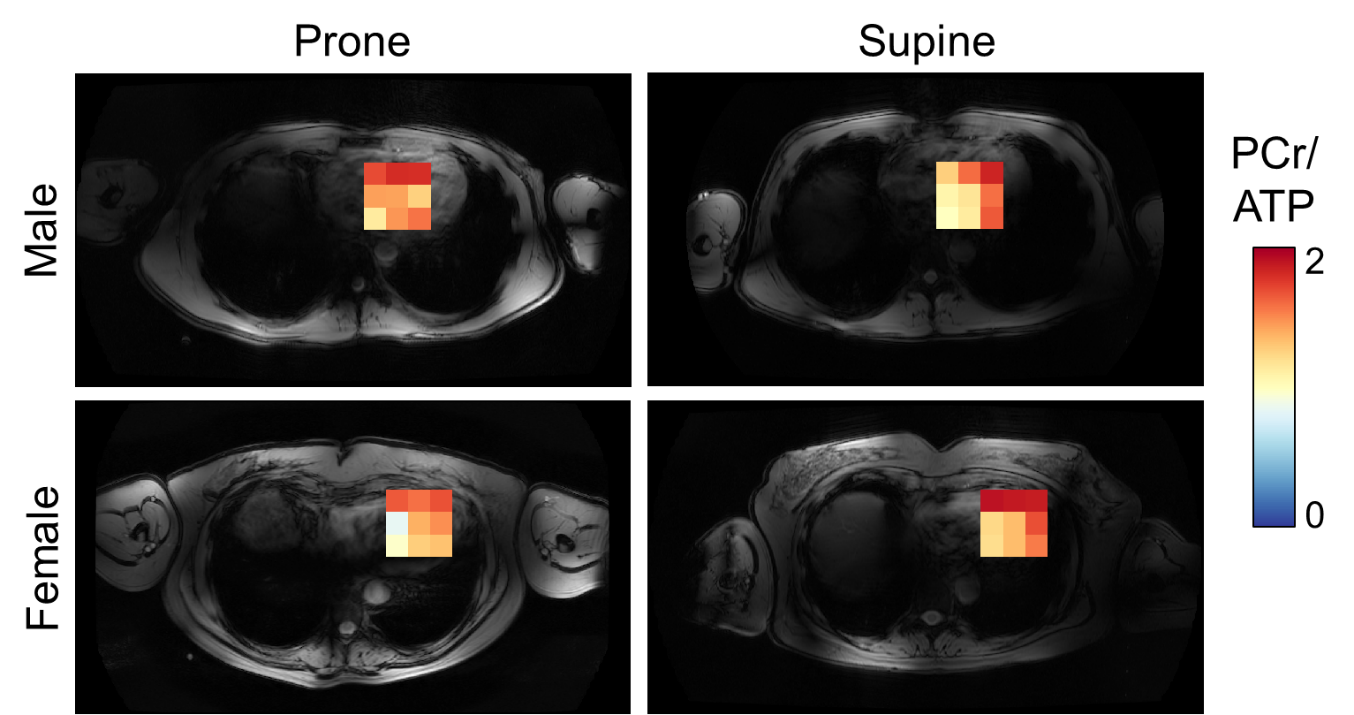
Cardiac PCr/ATP ratio maps are shown in Figure 5. PCr/ATP ratios were noticeably higher in the most anterior row, closest to the chest muscles. Average PCr/ATP ratios in the male subject were 1.52±0.23 and 1.37±0.31 in prone and supine positions, respectively, and in the female subject 1.36±0.29 and 1.56±0.29, respectively.
Discussion and Conclusion
Using an integrated 31P whole-body birdcage transmit coil in combination with a 16-channel 31P body receive array at 7T, cardiac 3D 31P MRSI data were obtained with good sensitivity throughout the whole heart, regardless of the position of the subject, i.e., prone or supine. The setup allows for easy patient positioning and large FOV scanning, similar to 1H body imaging at 1.5T or 3T, and enabling simultaneous acquisition of e.g. heart and liver 31P MRSI data. In conclusion, with an integrated 31P whole-body transmit coil at 7T, cardiac 31P MRS can be performed in the more comfortable supine position, with good sensitivity also in the posterior cardiac wall.Acknowledgements
No acknowledgement found.References
1. Abdurrachim D, Prompers JJ. Evaluation of cardiac energetics by non-invasive 31P magnetic resonance spectroscopy. Biochim Biophys Acta Mol Basis Dis. 2018;1864(5 Pt B):1939-1948.
2. Bakermans AJ, Bazil JN, Nederveen AJ, Strijkers GJ, Boekholdt SM, Beard DA, Jeneson JAL. Human cardiac 31P-MR spectroscopy at 3 Tesla cannot detect failing myocardial energy homeostasis during exercise. Front Physiol. 2017;8:939.
3. Stoll VM, Clarke WT, Levelt E, Liu A, Myerson SG, Robson MD, Neubauer S, Rodgers CT. Dilated Cardiomyopathy: Phosphorus 31 MR spectroscopy at 7 T. Radiology. 2016;281(2):409-417.
4. Valkovič L, Dragonu I, Almujayyaz S, Batzakis A, Young LAJ, Purvis LAB, Clarke WT, Wichmann T, Lanz T, Neubauer S, Robson MD, Klomp DWJ, Rodgers CT. Using a whole-body 31P birdcage transmit coil and 16-element receive array for human cardiac metabolic imaging at 7T. PLoS One. 2017;12(10):e0187153.
5. van den Wildenberg L, Gursan A, Seelen LWF, van der Velden TA, Gosselink MWJM, Froeling M, van der Kemp WJM, Klomp DWJ, Prompers JJ. In vivo phosphorus magnetic resonance spectroscopic imaging of the whole human liver at 7 T using a phosphorus whole-body transmit coil and 16-channel receive array: Repeatability and effects of principal component analysis-based denoising. NMR Biomed. 2023;36(5):e4877.
6. van Houtum QQ, Mohamed Hoesein FFAA, Verhoeff JJJC, van Rossum PPSN, van Lindert AASR, van der Velden TTA, van der Kemp WWJM, Klomp DDWJ, Arteaga de Castro CCS. Feasibility of 31 P spectroscopic imaging at 7 T in lung carcinoma patients. NMR Biomed. 2021;34(5):e4204.
7. Raaijmakers AJ, Italiaander M, Voogt IJ, Luijten PR, Hoogduin JM, Klomp DW, van den Berg CA. The fractionated dipole antenna: A new antenna for body imaging at 7 Tesla. Magn Reson Med. 2016;75(3):1366-1374.
8. Yarnykh VL. Actual flip-angle imaging in the pulsed steady state: a method for rapid three-dimensional mapping of the transmitted radiofrequency field. Magn Reson Med. 2007;57(1):192-200.
9. Froeling, M. QMRTools: A Mathematica Toolbox for Quantitative MRI Analysis. J. Open Source Softw. 2019;4(38):1204.
10. Rodgers CT, Robson MD. Receive array magnetic resonance spectroscopy: Whitened singular value decomposition (WSVD) gives optimal Bayesian solution. Magn Reson Med. 2010;63(4):881-891.
11. Veraart J, Novikov DS, Christiaens D, Ades-Aron B, Sijbers J, Fieremans E. Denoising of diffusion MRI using random matrix theory. Neuroimage. 2016;142:394-406.
12. Vanhamme L, van den Boogaart A, Van Huffel S. Improved method for accurate and efficient quantification of MRS data with use of prior knowledge. J Magn Reson. 1997;129(1):35-43.
13. Purvis LAB, Clarke WT, Biasiolli L, Valkovič L, Robson MD, Rodgers CT. OXSA: An open-source magnetic resonance spectroscopy analysis toolbox in MATLAB. PLoS One. 2017;12(9):e0185356.
Figures