1782
REACT-MIX for simultaneous non-contrast-enhanced MR angiography and vascular calcification imaging with modified PSIR framework1Philips Japan, Tokyo, Japan, 2Department of Radiology, Eastern Chiba Medical Center, Chiba, Japan, 3Philips GmbH Market DACH, Hamburg, Germany, 4Philips Healthcare, Best, Netherlands, 5Philips Healthcare, Rochester, MN, United States, 6Diagnostic Radiology and Radiation Oncology, Graduate School of Medicine, Chiba University, Chiba, Japan
Synopsis
Keywords: Vascular, Vessels, MRA
Motivation: Visualizing vascular calcifications is crucial for atherosclerosis assessment, guiding interventions, and predicting risks. Existing MRI techniques fall short in this regard, necessitating additional time-consuming scans or resorting to CTA.
Goal(s): To develop a new non-contrast, single-scan solution to simultaneously acquire MR angiography (MRA) and calcification-weighted images (CWI).
Approach: We redesigned and extended the existing Relaxation-Enhanced Angiography without ContrasT (REACT) framework with different pre-pulses, termed REACT-MIX. Volunteers were used for feasibility testing, comparisons with existing techniques, and subsequent patient evaluations to assess vascular lesions.
Results: Initial findings indicated good feasibility of simultaneous MRA and CWI, encouraging further clinical evaluation.
Impact: REACT-MIX introduces a new approach enabling simultaneous non-contrast MR angiography and calcification-weighted imaging across a wide FOV in a single scan. It offers promise for clinical assessments of systemic atherosclerosis. Further studies are warranted to confirm its full potential.
INTRODUCTION
Vascular calcification is a clinical marker of atherosclerosis1. Demonstration of vascular calcifications is desirable for several reasons, including guidance of percutaneous access for interventional vascular procedures and as a biomarker for future cardiovascular adverse events. Vascular calcifications are poorly visualized using standard MRI/MRA techniques. Only CTA is able to reliably detect vascular calcifications and display them in a large field-of-view (FOV) projection2,3.Recently, several studies suggested that optimized 3D gradient echo sequences could visualize the calcifications2,3 and/or bony structures4,5 on MRI. However, these sequences need separate scans in addition to MRA images, this results in long exam times and image misalignments due to possible motion between the scans.
A non-contrast-enhanced, relaxation-based, flow-independent MRA method, called Relaxation-Enhanced Angiography without ContrasT (REACT) has recently been proposed for vascular imaging in various body parts with large anatomical coverage6. Since REACT is also based on 3D gradient echo sequence, we hypothesized that it can be extended to simultaneously obtain MRA images and calcification weighted images (CWI) in one single scan.
In this study, we attempted to develop simultaneous non-contrast MRA and CWI by extending the technique with combination of different pre-pulses. The new REACT-MIX method was tested in volunteers for feasibility, compared with the original techniques, and subsequently applied in patients for assessment of vascular lesions.
METHODS
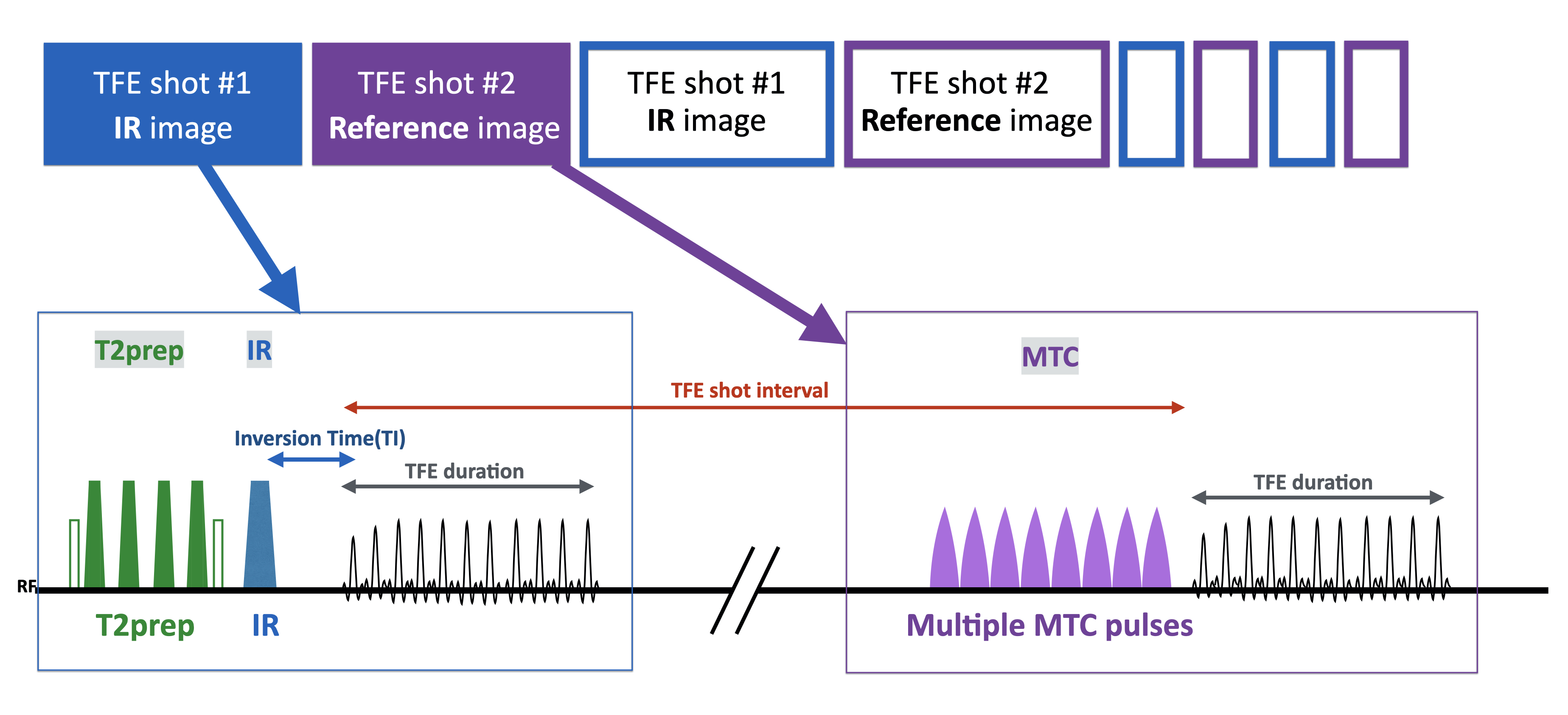
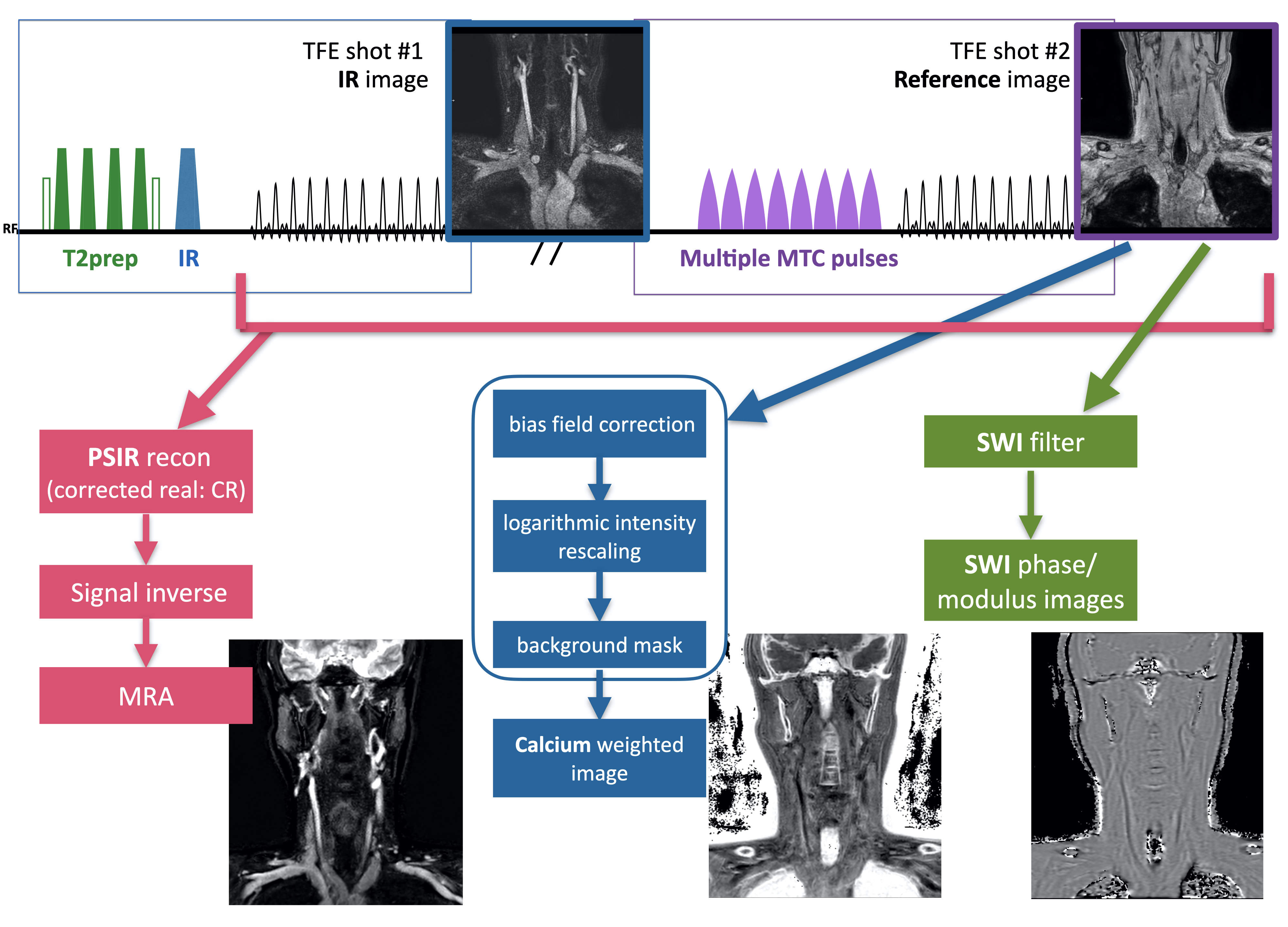
A schematic overview of the REACT-MIX sequence is shown in Figure 1. It is based on phase-sensitive inversion recovery (PSIR)7 framework, consisting of two signal acquisition modules. Each module contains different pre-pulses. First module is similar to the originally REACT with 3D turbo field-echo (TFE) readout preceded by a T2prep pulse and a non-selective IR pulse. These magnetization preparation pulses help to suppress signal from tissues such as muscles, nerves and fat. After signal recovery, the second signal acquisition was carried out with 3D TFE readout preceded by multiple (eight in this work) off-resonance magnetization transfer contrast (MTC) pre-pulses to obtain CWI images.An image reconstruction overview of the REACT-MIX sequence is shown in Figure 2. MRA images are generated by PSIR reconstruction. CWI are generated by shot #2 readout with bone imaging processing, which is frequently used for UTE-based bone imaging8. In addition, susceptibility weighted imaging (SWI) can be reconstructed from the shot #2 readout. SWI might also be useful for calcification detection9. Consequently, REACT-MIX provides MRA, CWI and SWI images in one single scan. As all datasets are inherently spatially aligned, no post-processing for misalignment is needed.
A total of 5 volunteers and 5 patients were examined on a 3.0T whole-body clinical system (Ingenia CX, Philips Healthcare, Netherlands). The study was approved by the local IRB, and written informed consent was obtained from all subjects.
REACT-MIX images were compared with conventional REACT and bone weighted imaging (Fast field echo resembling a CT using restricted echo-spacing: FRACTURE)4,5 for image quality, especially for the overall SNR and the presence of artifacts. To quantitatively compare the image contrast, we measured the contrast-ratio (CR) between the common carotid arteries and sternocleidomastoid muscles for MRA, between the cervical spine vertebrae and sternocleidomastoid muscles for CWI.
For the clinical atherosclerotic cases, REACT-MIX images were compared with CT imaging.
Imaging parameters for REACT-MIX were; Coronal, voxel size=1.00x1.00 x2.00mm3, TFE shot-interval=2500ms, TR=3.8ms, TE=2.3ms, flip angle=12° (for both IR and reference images), NSA=1, TFE factor=72, Compressed SENSE-reduction factor=4,6, and total acquisition time=5m50s.
RESULTS and DISCUSSION
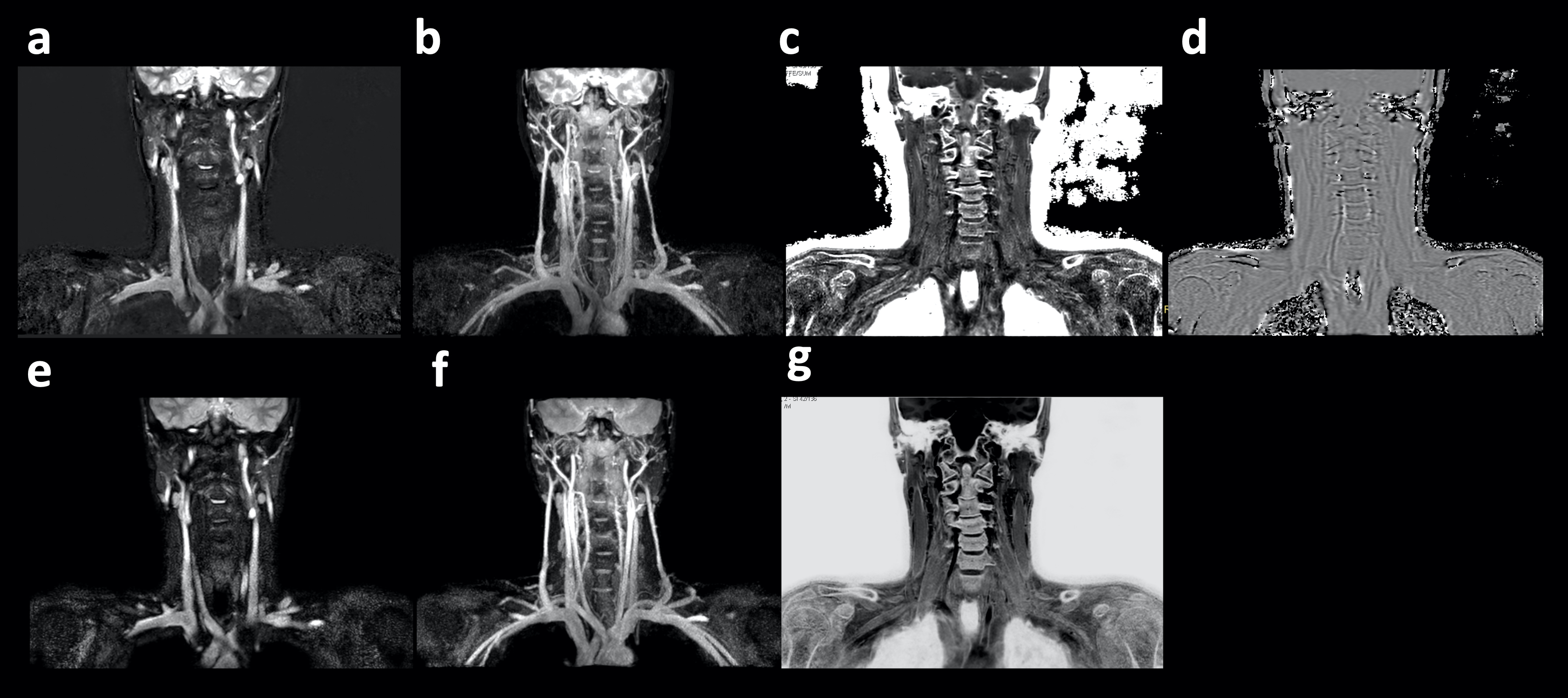
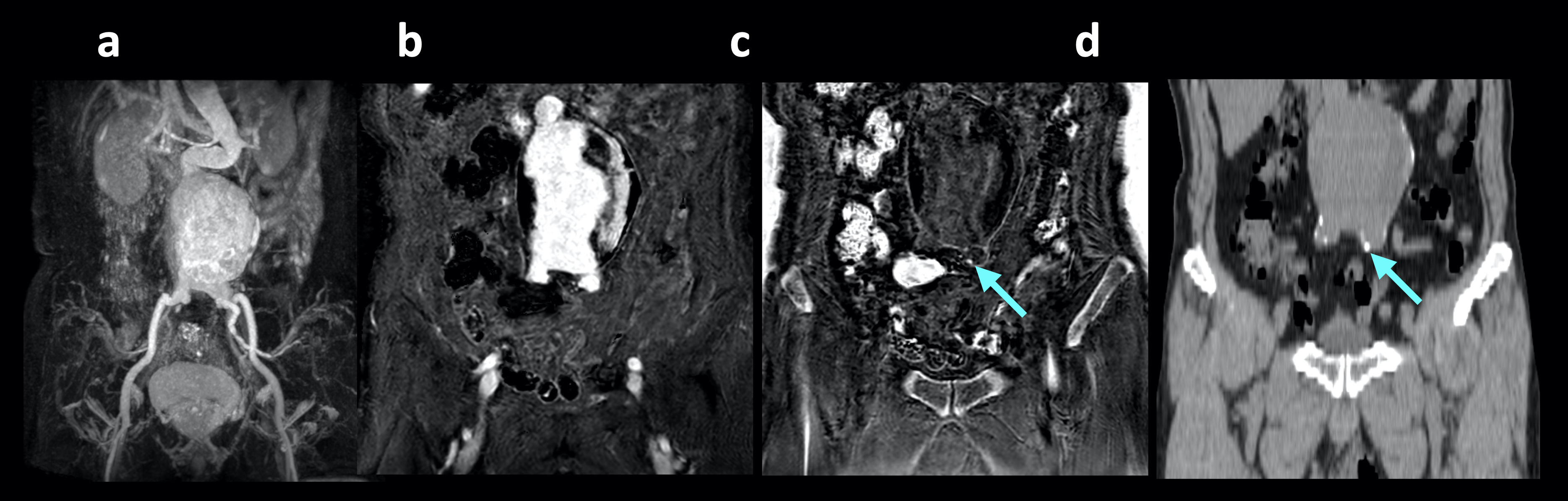
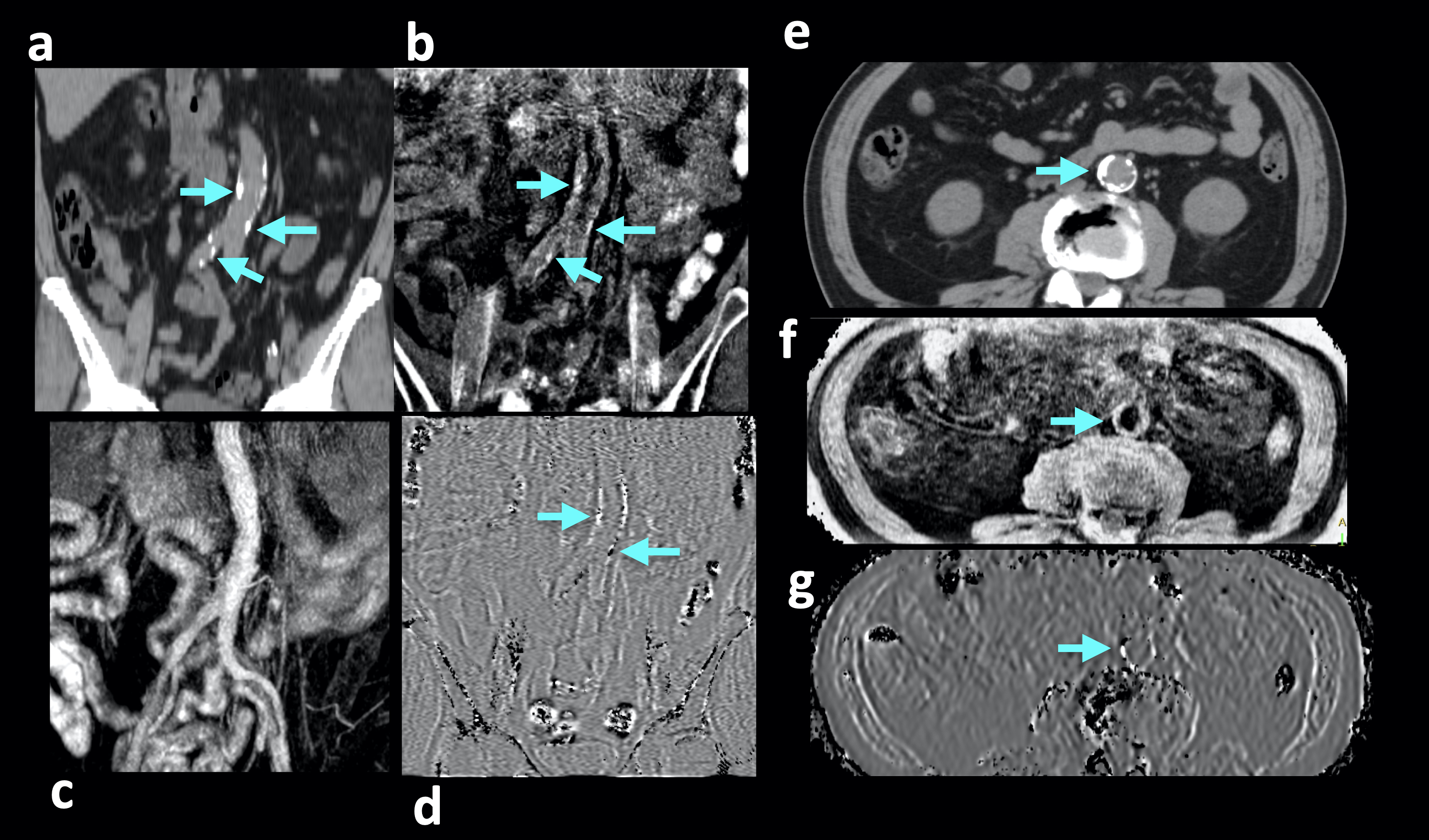
The quality of REACT-MIX MRA and CWI was considered comparable to that of the conventional REACT and FRACTURE, respectively. REACT-MIX MRA indicated higher CR (0.91±0.03) compared with that of the REACT MRA (0.71±0.02), also REACT-MIX CWI showed similar CR (0.34±0.08) to that of the FRACTURE (0.35±0.07). Representative images from all these techniques are shown in Figure 3. It is noteworthy that REACT-MIX provided MRA and CWI in one single scan and allowed for imaging over a large FOV at 3.0T with homogenous background suppression without obvious artifacts.Two clinical cases with patients with abdominal aorta aneurism with calcifications [Fig.4] and atherosclerosis with calcifications [Fig.5] demonstrated that major calcifications may be clearly visualized in REACT-MIX CWI. Visualization of small calcifications, which can be seen on CT images, is still challenging, further improvement and optimization is needed.
REACT-MIX may also be extended for surgical planning fusion imaging of vascular diseases, such as carotid endarterectomy (CEA)10, by using the self-fusion images of angiography and bone/calcification weighted imaging.
CONCLUSION
REACT-MIX enables simultaneous non-contrast MR angiography and calcification weighted imaging over a large FOV in one single scan. It holds promise for assessment of systemic atherosclerosis. Further clinical studies in comparison to the current standard methods are warranted.Acknowledgements
No acknowledgement found.References
1. Shi X, et al. Calcification in Atherosclerotic Plaque Vulnerability: Friend or Foe? Front Physiol. 2020 Feb 5;11:56. doi: 10.3389/fphys.2020.00056.
2. Edelman RR, et al. Projection MR imaging of peripheral arterial calcifications. Magn Reson Med. 2015 May;73(5):1939-45. doi: 10.1002/mrm.25320.
3. Ferreira Botelho MP, et al. MR imaging of iliofemoral peripheral vascular calcifications using proton density-weighted, in-phase three-dimensional stack-of-stars gradient echo. Magn Reson Med. 2017 Jun;77(6):2146-2152. doi: 10.1002/mrm.26295.
4. Johnson B, et al. Fast field echo resembling a CT using restricted echo-spacing (FRACTURE): a novel MRI technique with superior bone contrast. Skeletal Radiol. 2021 Aug;50(8):1705-1713. doi: 10.1007/s00256-020-03659-7.
5. Gascho D, et al. FRACTURE MRI: Optimized 3D multi-echo in-phase sequence for bone damage assessment in craniocerebral gunshot injuries. Diagn Interv Imaging. 2020 Sep;101(9):611-615. doi: 10.1016/j.diii.2020.02.010.
6. Yoneyama M, et al. Free-breathing non-contrast-enhanced flow-independent MR angiography using magnetization-prepared 3D non-balanced dual-echo Dixon method: A feasibility study at 3 Tesla. Magn Reson Imaging. 2019:16;63:137-146.
7. Kellman P, et al. Phase-sensitive inversion recovery for detecting myocardial infarction using gadolinium-delayed hyperenhancement. Magn Reson Med. 2002 Feb;47(2):372-83. doi: 10.1002/mrm.10051.
8. Yoneyama M, et al. Volume isotropic 3D bone Imaging with broadband IR-prepared FLORET UTE and Fibonacci interleaved trajectory ordering. Proc. ISMRM2023 #0632.
9. Adams LC, et al. Detection of vessel wall calcifications in vertebral arteries using susceptibility weighted imaging. Neuroradiology. 2017 Sep;59(9):861-872. doi: 10.1007/s00234-017-1878-z.
10. Kikuchi J, et al. Preoperative Novel Magnetic Resonance Fusion Imaging for Carotid Endarterectomy Patients with Contrast Contraindications: A Pilot Study. World Neurosurg. 2023 Jul;175:e1075-e1088. doi: 10.1016/j.wneu.2023.04.071.
Figures