1781
Identification of viable myocardium within infarct scar by high-resolution manganese-enhanced MRI1IHU Liryc, Univ. Bordeaux, CNRS, CRMSB, UMR 5536, Bordeaux, France, 2IHU Liryc, Univ. Bordeaux, INSERM, CRCTB, U1045, Bordeaux, France
Synopsis
Keywords: Myocardium, Contrast Agent, manganese-enhanced MRI
Motivation: Manganese-enhanced MRI (MEMRI) appears to be an interesting alternative to late-gadolinium enhancement (LGE) since manganese ions can enter cardiomyocytes through calcium channels, thus allowing intracellular characterization of living cells.
Goal(s): This study aims to evaluate the sensitivity of 3D-MEMRI for the characterizing MI scars heterogeneity compared to the clinical gold standard LGE.
Approach: Manganese has a long retention time in cardiomyocytes, allowing a longer acquisition time exploited to improve the spatial resolution of 3D MR images (~1 mm3 isotropic).
Results: This study confirms the potential of 3D-MEMRI as a more specific method than the clinical gold standard LGE for characterizing MI scars heterogeneity.
Impact: The ability of high-resolution 3D manganese-enhanced MRI (3D-MEMRI) to produce a finer characterization of the heterogeneity of the scar constitutes an important step forward in the management of myocardial infarction in the context of cardiac arrhythmias
Introduction
Myocardial infarction (MI) scars are heterogeneous and are mainly composed of replacement fibrosis intertwined with viable cardiomyocytes, creating areas of slowed electrical conduction [1], [2]. Late gadolinium-enhancement MRI (LGE) is the gold-standard method in the clinical assessment of MI, allowing a quantifiable assessment of the morphology of fibrous scar [3]. However, gadolinium-based contrast agents, due to their exclusively extracellular nature, do not allow clear delineation of the junction zones between viable myocardial tissue and the infarction scar. Manganese-enhanced MRI (MEMRI) may be an interesting alternative since manganese ions can enter cardiomyocytes through calcium channels, allowing intracellular characterization of living cells. This study aims to evaluate the sensitivity of 3D-MEMRI for the characterizing MI scars heterogeneity compared to the clinical gold standard LGE.Methods
MI was induced in sheep (n=3) by placing a micro-coil in the left anterior descending artery to reduce perfusion and create a heterogeneous scar in the left ventricle.MRI acquisitions (1.5 Tesla, MAGNETOM Aera, Siemens) were performed at 6-7 weeks post-infarction. MEMRI and LGE ideally require two separate examinations to avoid overlapping T1 contrast changes associated with each contrast agent. However, we evaluated whether the two injections could be considered in a single session by comparing 3D-LGE images obtained with/without manganese infusion:
At 6 weeks, 3D-MEMRI after intravenous infusion of manganese chloride (5 μmol/kg) followed one hour later by 3D-LGE after bolus injection of gadoterate meglumine (0.1mmol/kg, half dose), in order to compare images at the same time.
At 7 weeks, 3D-LGE only after bolus injection of gadoterate meglumine (0.2mmol/ kg) to acquire images using the reference clinical technique.
Sequence parameters are summarized in Fig.1. The MOLLI-MoCo sequence was acquired before and after administration of contrast agents to obtain T1maps of ventricles. IR GRE sequences were performed to obtain 3D images of the whole heart. An inversion time (TI) scout sequence was acquired to determine the optimal TI to visualize the scar in hyposignal for MEMRI and in hypersignal for LGE. Images were analyzed on manufacturer’s console (SyngoVia, Siemens).
After heart explant, a portion of the left ventricle surrounding the infarct was perfused to quantify epi- and endocardial electrical conduction properties by high-resolution optical mapping [4]. Left ventricular preparations were fixed with formalin and then studied by ex vivo MRI at 1.5T and by histology.
Results
Fig.2A shows typical 2D T1maps obtained in sheep with chronic MI. A decreased myocardial T1 is observed 15 minutes after MnCl2 infusion and maintained until 60 minutes post-infusion. T1 LGE post-MEMRI was compared to T1 LGE without prior manganese infusion, and both show similar T1 values of blood and myocardium (Fig.2B), indicating the ability to perform MEMRI and LGE acquisitions during a single examination, using a half dose of gadolinium.Fig.3 shows representative 3D-MEMRI and 3D-LGE obtained in the same sheep. In 3D-MEMRI, hyposignal areas seem to indicate necrotic tissue in the epicardium and in the mid-wall (Fig.3A). In 3D-MEMRI iso, the thin strip of viable tissue in mid-wall, in-between the two necrotic areas, appears sharper than in 3D-MEMRI (Fig.3B). However, in the 3D-LGE post-MEMRI, fibrotic scar appears in hypersignal and located prominently on the endocardium (Fig.3C). In order to avoid the overlap in the T1 contrast, a separated 3D-LGE was acquired 1 week later (Fig.3D). Compared to 3D-LGE post-MEMRI, a stronger contrast can be observed between infarct and myocardium, attributed to manganese long retention in the former acquisition. Nevertheless, a similar hyper intensity located more prominently in the endocardium is observed.
Fig.4A shows 3D-MEMRI and 3D-LGE images positioned on the same infarcted area. Using ex vivo optical mapping techniques, electrically functional cells were found on the endocardium attesting viability of the cells, yet functional signals were absent when mapping the epicardial surface (Fig.4B). The localization of the infarcted area was validated by ex vivo MRI (Fig.4C) and histological analysis (Fig.4D). It showed a scar positioned more prominently on the epicardium and heterogeneous contrast from mid-wall to endocardium, which is consistent with MEMRI but not with the gold standard LGE.
Conclusion
This study confirms the potential of manganese as a more specific contrast agent than gadolinium to identify conduction pathways associated with viable cells within the peri- and intra-scar areas. The long retention time of manganese ions in the cardiomyocytes allows longer acquisition time and thereby result in images with a higher spatial resolution (~1 mm3 isotropic). The ability of MEMRI to produce a finer characterization of the heterogeneity of the scar constitutes an important step forward in the management of MI in the context of potentially fatal cardiac arrhythmias.Acknowledgements
This study received financial support from the French Government as part of the “Investments of the Future” program managed by the National Research Agency (ANR), Grant reference ANR-10-IAHU-04. This project also received financial support from the French Federation of Cardiology (FFC), Grant reference FFC Impulsion 2023.References
[1] T. P. Nguyen, Z. Qu, et J. N. Weiss, « Cardiac fibrosis and arrhythmogenesis: The road to repair is paved with perils », J. Mol. Cell. Cardiol., vol. 70, p. 83‑91, mai 2014, doi: 10.1016/j.yjmcc.2013.10.018.
[2] B. Gorenek et al., « Cardiac arrhythmias in acute coronary syndromes: position paper from the joint EHRA, ACCA, and EAPCI task force », EP Eur., vol. 16, no 11, p. 1655‑1673, nov. 2014, doi: 10.1093/europace/euu208.
[3] A. S. Kanderian, R. Renapurkar, et S. D. Flamm, « Myocardial Viability and Revascularization », Heart Fail. Clin., vol. 5, no 3, p. 333‑348, juill. 2009, doi: 10.1016/j.hfc.2009.02.008.
[4] K. Kulkarni, N. Pallares-Lupon, A. A. Armoundas, P. Pasdois, O. Bernus, et R. D. Walton, « Investigating Electrophysiological Markers of Arrhythmogenesis in a Chronic Myocardial Infarction Ovine Model », Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. IEEE Eng. Med. Biol. Soc. Annu. Int. Conf., vol. 2022, p. 657‑661, juill. 2022, doi: 10.1109/EMBC48229.2022.9871496.
Figures
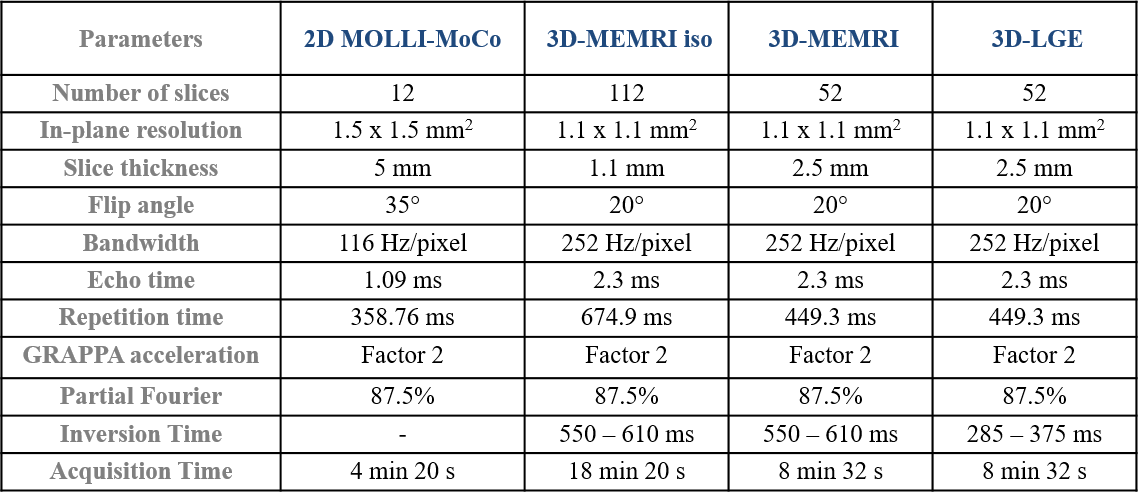
Figure 1: Sequence parameters of the modified 2D Look-Locker Inversion Recovery with motion correction (MOLLI-MoCo) and the 3D high-resolution inversion-recovery gradient echo (3D HR IR GRE) after intravenous infusion of manganese chloride (MEMRI) and/or bolus injection of gadoterate meglumine (LGE).
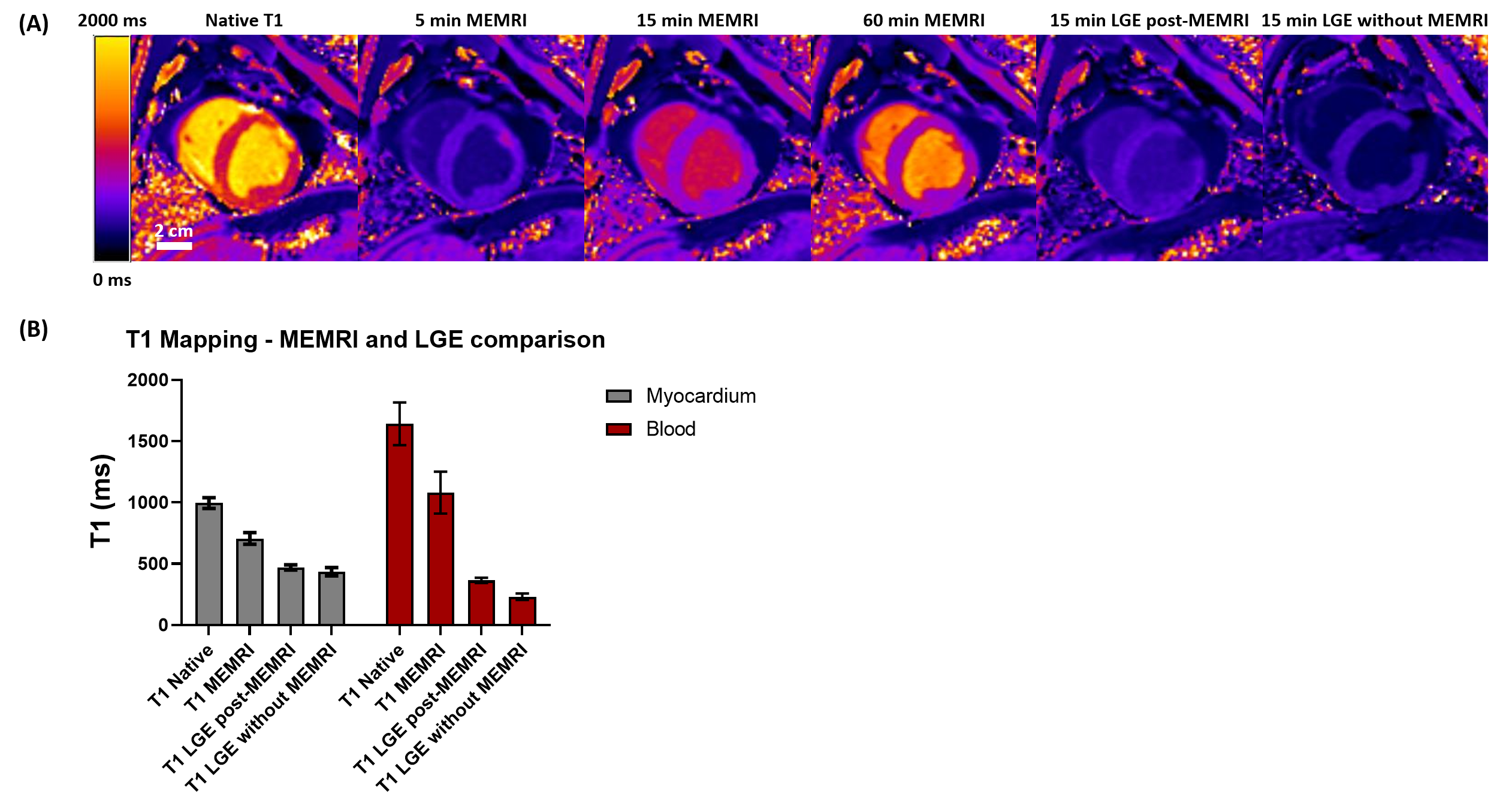
Figure 2: (A) Representative short-axis view of T1maps of a sheep with chronic myocardial infarction obtained during MEMRI acquisitions (5, 15 and 60 min post-infusion) and LGE (15 min post-injection) at 6 and 7 weeks post-infarction, respectively; (B) Quantitative T1 measurements obtained in the myocardium and blood of sheep (n=3) during MEMRI and LGE at 6 and 7 weeks post-infarction.
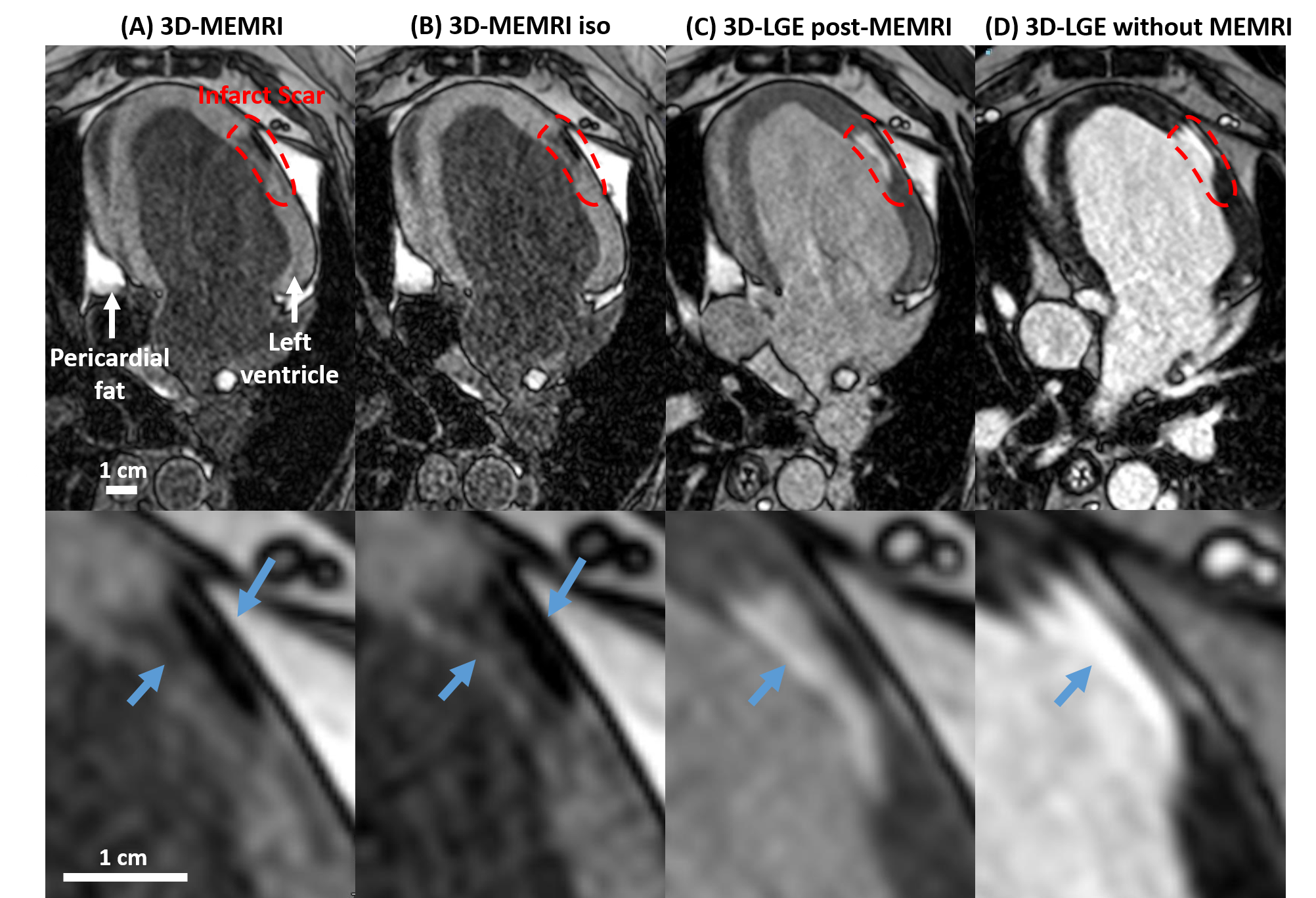
Figure 3: Representative cardiac 3D inversion-recovery gradient echo images: (A-C) 3D-MEMRI and 3D-LGE images acquired 6 weeks post infarction with a resolution for 3D-MEMRI of 1.1x1.1x2.5 mm3; 3D-MEMRI iso of 1.1x1.1x1.1 mm3 and 3D-LGE of 1.1x1.1x2.5 mm3; (D) 3D-LGE acquisition (1 week later and without prior MEMRI) with a resolution of 1.1x1.1x2.5 mm3. Inserts show magnification by 4 centered on the infarct area.
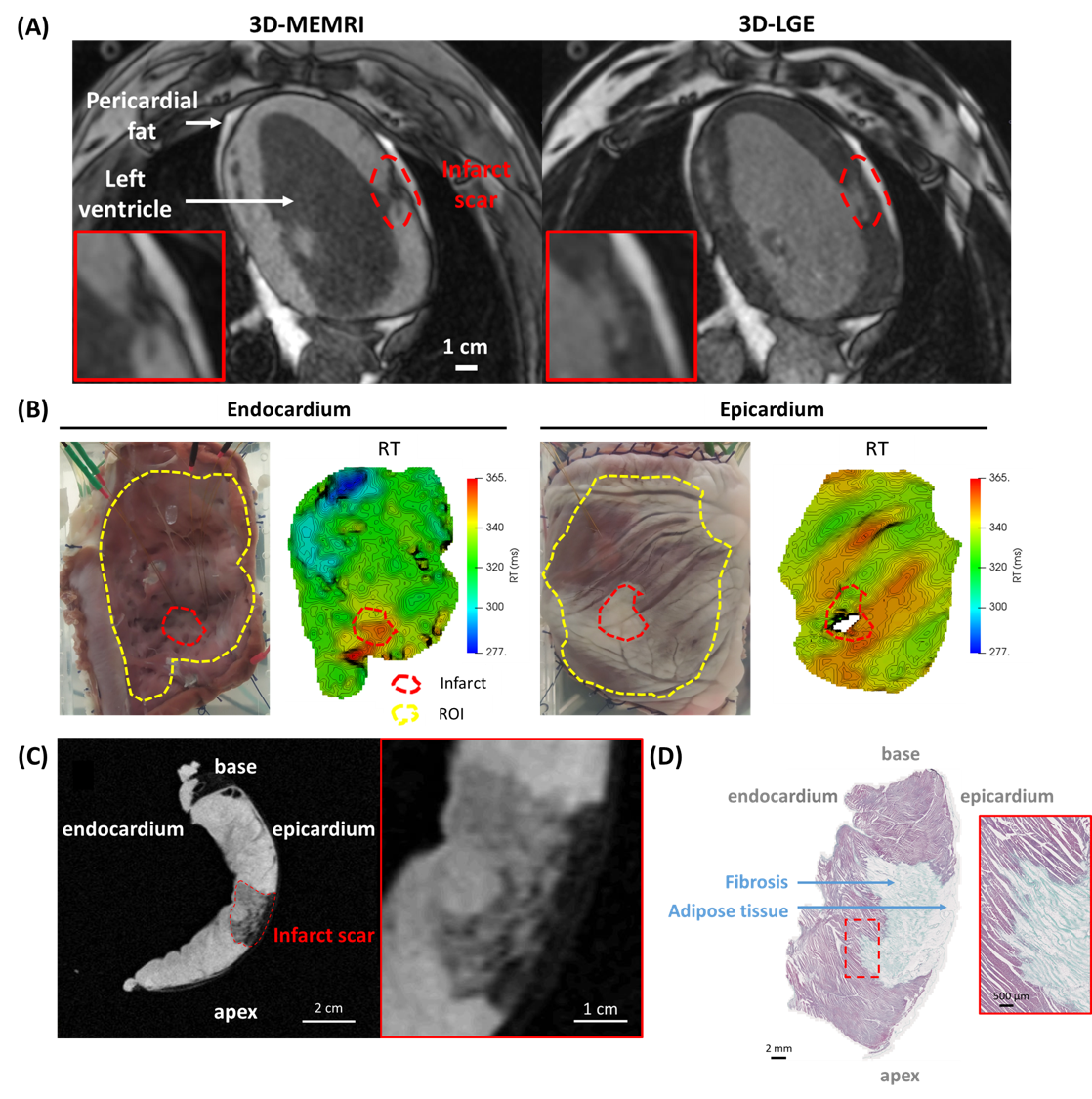
Figure 4: (A) In vivo MEMRI and LGE acquisitions (1.1x1.1x2.5 mm3) at 6 weeks post-infarction; (B) Macroscopic images and repolarization time (RT) at the level of the endocardium and epicardium of the left ventricle; (C) Ex vivo 3D FLASH T1 images obtained at 1.5 Tesla with a resolution of 500 μm3 isotropic; (D) Histological slices of the left ventricle colored with Masson trichrome staining (collagen fiber in green, cardiomyocyte cytoplasm in pink and nuclei in blue-violet).