1780
Defining right ventricular energy metabolism in patients with pulmonary arterial hypertension using hyperpolarized [1-13C]pyruvate1Advanced Imaging Research Center, UT Southwestern Medical Center, Dallas, TX, United States, 2Biomedical Engineering, UT Southwestern Medical Center, Dallas, TX, United States, 3Radiology, UT Southwestern Medical Center, Dallas, TX, United States, 4Internal Medicine, UT Southwestern Medical Center, Dallas, TX, United States, 5Pediatrics, UT Southwestern Medical Center, Dallas, TX, United States
Synopsis
Keywords: Heart Failure, Cardiovascular
Motivation: Right ventricular (RV) failure in pulmonary arterial hypertension (PAH) increases mortality risk, yet its metabolic characteristics is largely unknown, primarily due to limitations of imaging the RV.
Goal(s): This study examines the relative contribution of oxidative metabolism versus glycolysis in the failing RV before and after initiation of pulmonary vasodilator therapy for PAH.
Approach: Patients with newly diagnosed PAH are examined by HP [1-13C]pyruvate MRI at baseline and again 4-6 months after initiation of pulmonary vasodilator therapy.
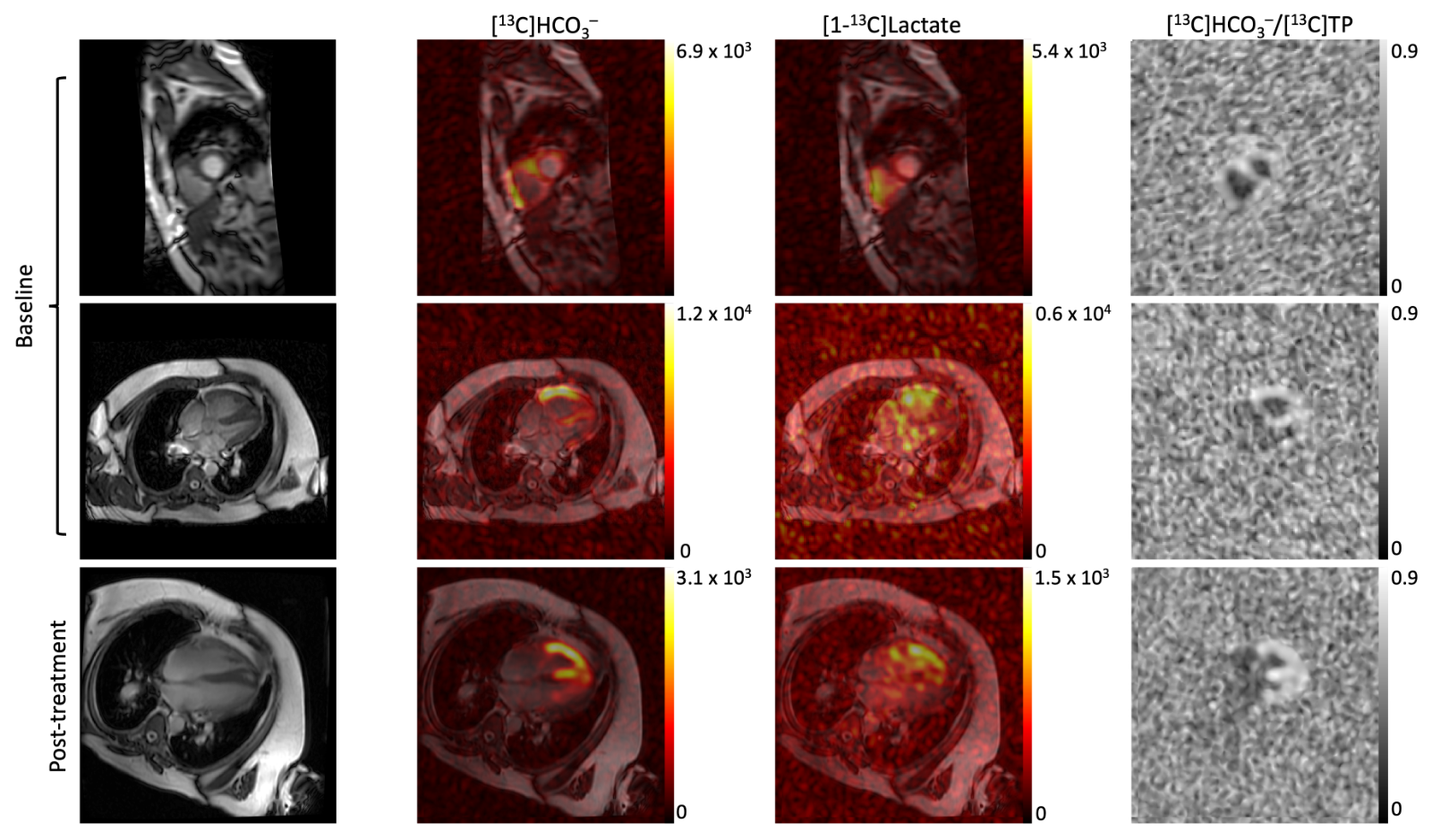
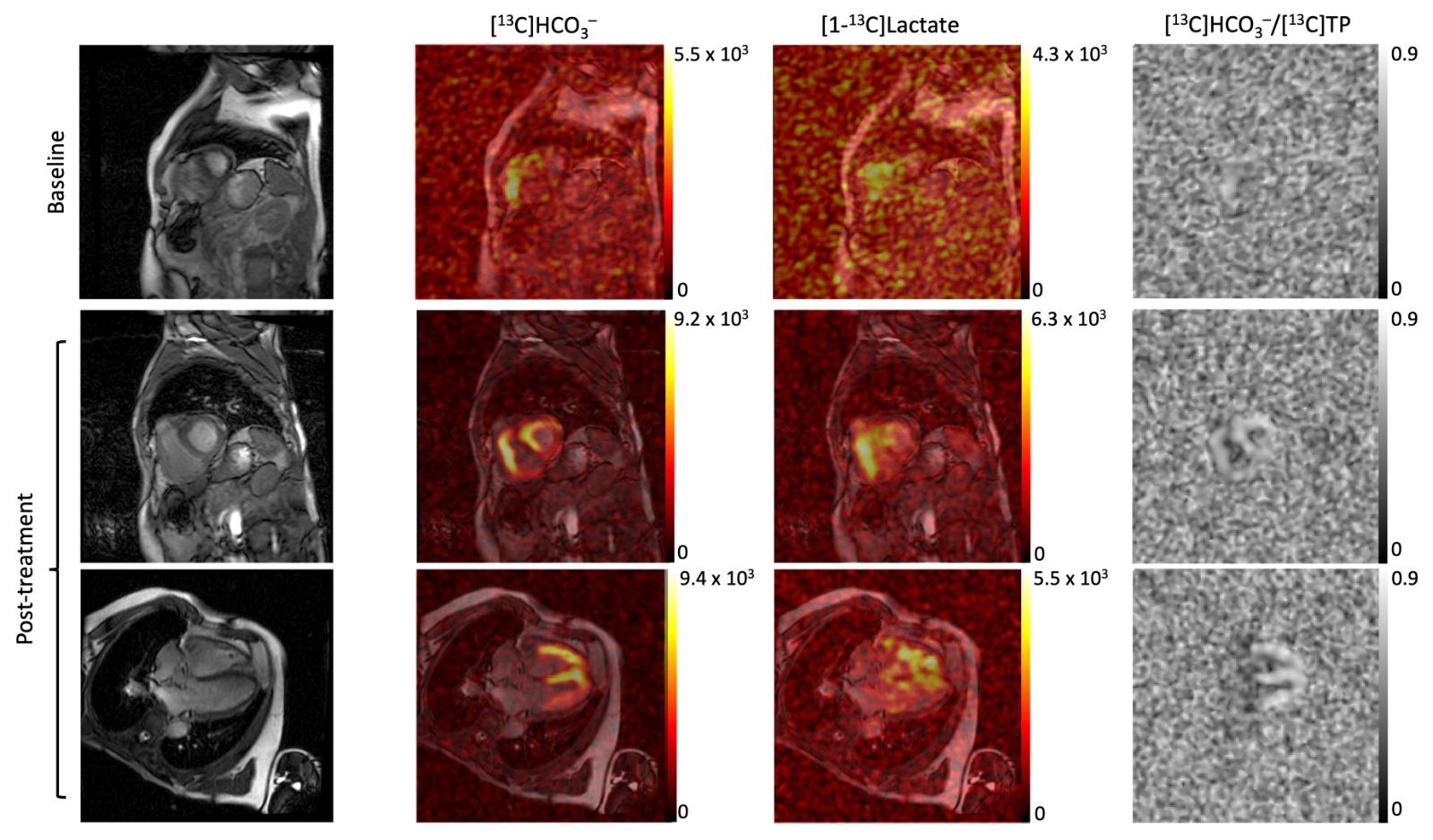
Results: Patients exhibited hyperintense HP bicarbonate signals in RV free wall. After treatment, normalized myocardial [13C]bicarbonate production increased.
Impact: Importance of metabolic flexibility in RV heart failure is underexplored. A better understanding of how the RV myocardium remodels in RV failure from PAH and in response to therapy may allow for development of RV-targeted therapies to maintain RV function.
INTRODUCTION
Right ventricular (RV) failure in pulmonary arterial hypertension (PAH) significantly increases mortality risk1. Preclinical studies suggest this is accompanied by an increasing rate of RV myocardial glucose utilization, particularly glycolysis, though this has been difficult to quantify in humans due to limitations of imaging the RV2-4. 13C MRI using hyperpolarized (HP) [1-13C]pyruvate is a novel modality to track the metabolic fate of pyruvate by assessing its products such as [1-13C]lactate (glycolysis) and [13C]bicarbonate (HCO3-, glucose oxidation) that may provide novel insights into the failing RV5.METHODS
The protocol of the human study is approved by the local Institutional Review Board (STU-2020-1351). In this proof-of-concept pilot study (NCT04968210), three participants with newly diagnosed group 1 PAH will complete HP 13C-pyruvate MRI at baseline and again 4-6 months after initiation of pulmonary vasodilator therapy. At each visit, HP [1-13C]pyruvate, prepared using a 5T SPINlab DNP polarizer (GE Healthcare), is administered intravenously up to twice (one short-axis view, one long-axis 4-chamber view), separated by 30 minutes, during a 13C/1H-integrated MRI session. Following multiphase 1H MRI and B0 shimming using the body coil at a 3T wide-bore MRI scanner (GE Healthcare 750w Discovery), metabolite-interleaved 13C MRI is acquired using a dual-loop 13C RF coil (Pulseteq) with a bolus injection of 250-mM HP [1-13C]pyruvate (5mL/s). Metabolite maps of HP [13C]bicarbonate, [1-13C]lactate, and [1-13C]pyruvate are dynamically acquired every cardiac cycle in an interleaved manner by exciting one metabolite at a time with a spectral-spatial RF pulse6. Subjects are instructed to hold their breath in expiration for ~20 s, followed by a shallow breathing to minimize the respiratory motion. The center frequency is calculated from the water resonance6. For comparison between the baseline and post-treatment, time-averaged [13C]bicarbonate is normalized to the time-averaged total HP product (bicarbonate + lactate).RESULTS and DISCUSSION
To date, two patients with PAH have completed the study after informed written consents. Intense HP [13C]bicarbonate signals were detected from RV wall from both patients and remained strong post-treatment, Figure 1. After initiation of oral vasodilators, cardiac function and hemodynamics improved significantly for Patient #1 (62-year-old male): mean pulmonary arterial pressure (mPAP) 56 to 45 mmHg, cardiac index 2.2 to 3.0 L/min/m2, pulmonary vascular resistance (PVR) 11.9 to 7.1 Wood units. Pyruvate oxidation, measured from the four-chamber view, increased by 7.8% in RV free wall, 11.1% in left ventricular (LV) free wall, and 9.7% in septum, Figure 2. Patient#2 (59-year-old male) had 62 mmHg of mPAP, 12.1 Wood units of PVR with cardiac index 1.9 before treatment. He has not completed cardiac catheterization for follow-up yet. Pyruvate oxidation, measured from the short axis view, increased by 1.8 % in RV free wall, Figure 3. Post-treatment bicarbonate production in LV free wall and septum were enhanced, but the percent changes were not calculated due to low baseline signals.CONCLUSION
The failing RV can be metabolically imaged using HP 13C MRI. RV bicarbonate increased post-treatment. How RV metabolism modulates RV function merits further study. Surprisingly, LV pyruvate oxidation seems to robustly respond as well. Since the subject is not exposed to ionizing radiation, this approach is ideal for studies of response to interventions.Acknowledgements
This study was supported by United Therapeutics through the JENESIS Innovative Clinical Research Award and the National Institutes of Health of the United States (P41 EB015908, S10 OD018468).References
1. Campo A, Mathai SC, Le Pavec J, Zaiman AL, Hummers LK, Boyce D, Housten T, Lechtzin N, Chami H, Girgis RE, Hassoun PM. Outcomes of hospitalisation for right heart failure in pulmonary arterial hypertension. Eur Respir J. 2011;38(2):359-367.
2. Oikawa M, Kagaya Y, Otani H, Sakuma M, Demachi J, Suzuki J, Takahashi T, Nawata J, Ido T, Watanabe J, Shirato K. Increased [18F]fluorodeoxyglucose accumulation in right ventricular free wall in patients with pulmonary hypertension and the effect of epoprostenol. J Am Coll Cardiol. 2005; 45:1849–1855.
3. Nagaya N, Goto Y, Satoh T, Uematsu M, Hamada S, Kuribayashi S, Okano Y, Kyotani S, Shimotsu Y, Fukuchi K, Nakanishi N, Takamiya M, Ishida Y. Impaired regional fatty acid uptake and systolic dysfunction in hypertrophied right ventricle. J Nucl Med. 1998; 39:1676–1680.
4. Piao L, Fang YH, Cadete VJJ, Wietholt C, Urboniene D, Toth PT, Marsboom G, Zhang HJ, Haber I, Rehman J, Lopaschuk GD, Archer SL. The inhibition of pyruvate dehydrogenase kinase improves impaired cardiac function and electrical remodeling in two models of right ventricular hypertrophy: resuscitating the hibernating right ventricle. J Mol Med. 2010; 88:47–60.
5. Golman K, Petersson JS, Magnusson P, Johansson E, Akeson P, Chai CM, Hansson G, Månsson S. Cardiac metabolism measured noninvasively by hyperpolarized 13C MRI. Magn Reson Med. 2008;59(5):1005-1013.
6. Ma J, Chen J, Reed GD, Hackett EP, Harrison CE, Ratnakar J, Schulte RF, Zaha VG, Malloy CR, Park JM. Cardiac T2∗ measurement of hyperpolarized 13C metabolites using metabolite-selective multi-echo spiral imaging. Magn Reson Med. 2021;86(3):1494-1504.
Figures
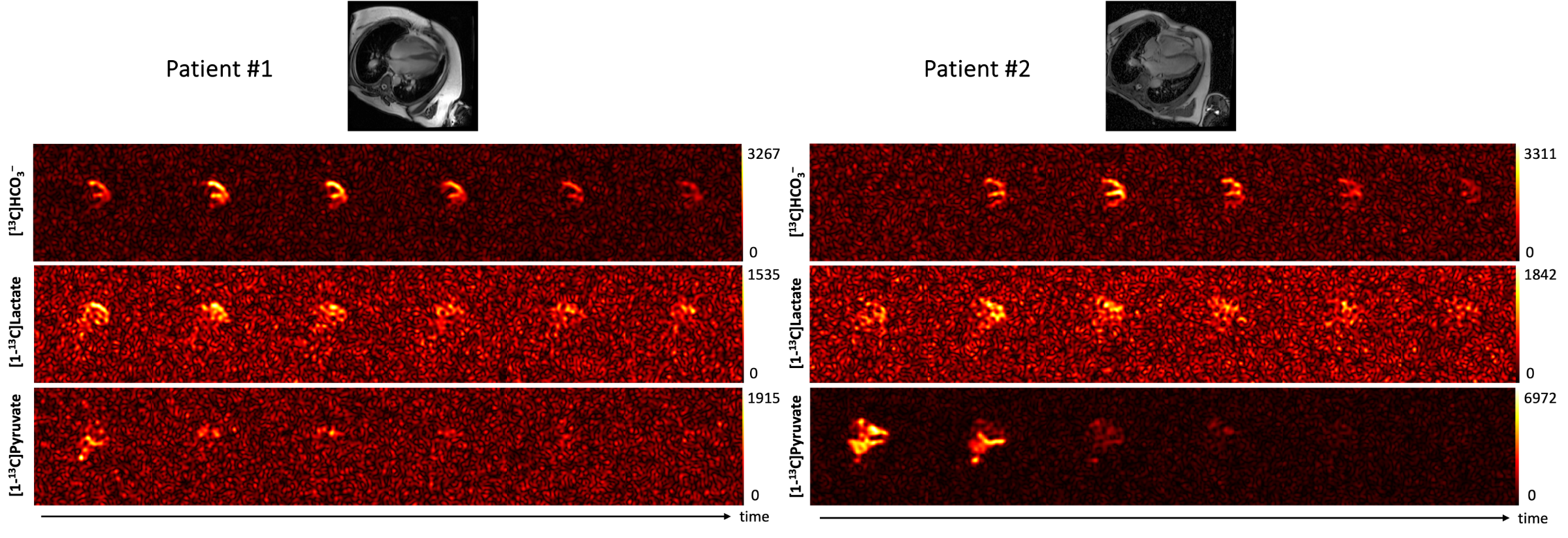
Figure 1. Post-treatment dynamic cardiac HP 13C MRI acquired from patients with PAH. Intense HP [13C]bicarbonate signals were detected from RV wall from both patients and remained strong post-treatment.