1777
IRON-HEART: Cardiac and skeletal muscle energetics in chronic heart failure and iron deficiency1University of Oxford, Oxford, United Kingdom, Oxford, United Kingdom, 2Oxford Centre for Clinical Magnetic Resonance Research (OCMR), University of Oxford, Oxford, United Kingdom, Oxford, United Kingdom
Synopsis
Keywords: Heart Failure, Spectroscopy, Cardiac 31P-MRS, Iron deficiency
Motivation: Determining the impact of iron repletion on muscle energetics in non-ischaemic cardiomyopathy with reduced ejection fraction (EF).
Goal(s): Use cardiac and skeletal muscle 31P MRS to assess cardiac and skeletal muscle energetics pre and post iron repletion therapy.
Approach: Participants and ID underwent CMR to assess cardiac function, MRS to assess Phosphocreatine to Adenosine triphosphate (PCr/ATP) ratio in cardiomyocyte and relation to skeletal muscle PCr consumption, end-exercise intracellular pH and PCr recovery rate before and after Ferric carboxymaltose (FCM).
Results: FCM improves ejection fraction, 6-minute-walk-distance. It didn’t change in myocardial resting or dynamic energetics or skeletal muscle oxidative metabolism.
Impact: Iron infusion didn’t change PCr/ATP, however increased left ventricular ejection fraction, therefor increase ATP requirement. We hypothesise that iron replacement resulted in increase in energy efficiency, or improved flux through Creatine Kinase, which was not assessed during this study.
Background
Iron deficiency (ID) remains a hot topic in heart failure (HF). Recent trials have shown iron replacement achieves benefit in exercise capacity and symptoms in patients with HF and ID. The underlying mechanism is poorly understood, but skeletal muscle metabolism is a key determinant of exercise capacity. We therefore investigated the impact of ID and replacement in HF, using magnetic resonance (MR) to examine dynamic metabolism in cardiac and skeletal muscle.Methods
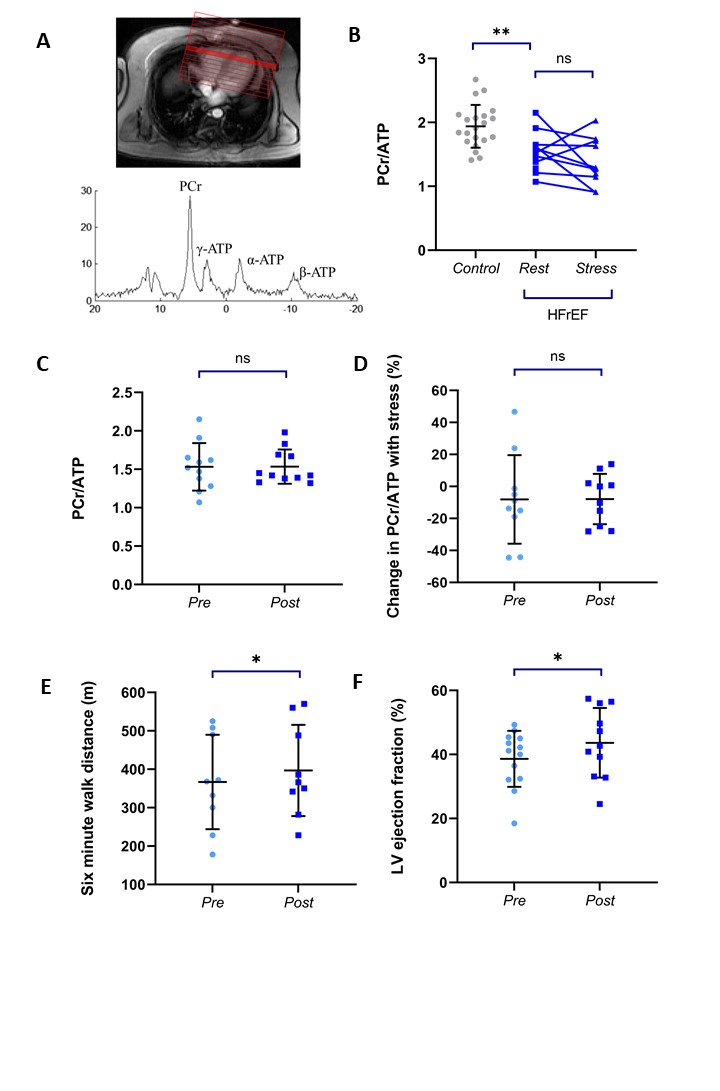
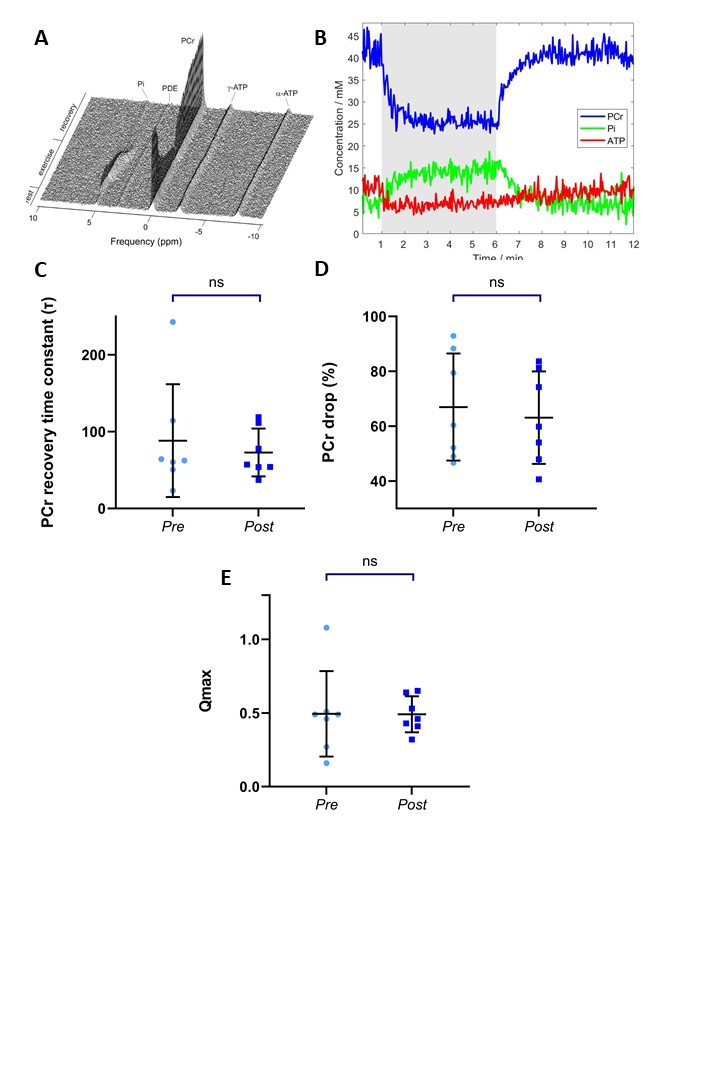
Patients with stable non-ischaemic HF (ejection fraction (EF)<45%) and ID (ferritin<100 mcg/dl, or 100-299 mcg/dl with transferrin saturation (Tsats)<20%) underwent cardiovascular magnetic resonance (MR) assessment on a 3T magnetic resonance imaging scanner (Magneton Prisma: Siemens Healthineers). All participants were scanned in a fasted state (at least 6 hours fast) before study assessments. Cardiac structure and function were assessed with a 13-channel body coil (Body 13, Siemens). Image analysis for ventricular volumes and function was performed offline using a semiautomated system (cmr42 Version 5.10.1; Circle Cardiovascular Imaging, Inc). Cardiac and skeletal muscle Phosphorus MR spectroscopy (31P-MRS) was performed using a Surface 1H/31P flex coil (Rapid Biomedical). A Depth Resolved MR spectroscopy (DRESS) acquisition was used. For Cardiac 31P-MRS was performed by positioning the voxel in the interventricular septum parallel to the coil. Three saturation bands were used to suppress signals from adjacent skeletal muscle and liver. Cardiac 31P-MRS was performed at rest and during dobutamine stress (65% maximum heart rate). For skeletal muscle 31P-MRS, the voxel was positioned over the gastrocnemius medialis and DRESS calibration and acquisition was performed at rest (1 minute), 4mins exercise (25% maximum voluntary contraction, MVC) and 7 minutes recovery to quantify the time constant of phosphocreatine (PCr) recovery rate (τPCr). Spectral analysis was performed offline using OXSA. The following parameters were analysed using MATLAB: skeletal muscle PCr consumption, end-exercise intracellular pH, and PCr recovery rate (τPCr). A 6 minute-walk-test (6WMT) and symptom assessment (Kansas City Cardiomyopathy questionnaire, KCCQ) were also performed. All studies were repeated 6 weeks post intravenous ferric carboxymaltose (FCM) administration (dose dependent on Haemoglobin and weight). The study was approved by the local research ethics committee and conforms to the principles of the Declaration of Helsinki and Good Clinical Practice. All participants gave written informed consent prior to inclusion. Statistical analyses were performed with IBM SPSS Statistics, Version 28 and GraphPad Prism (Version 9.0.2 for Windows; GraphPad Software, San Diego, CA).Results
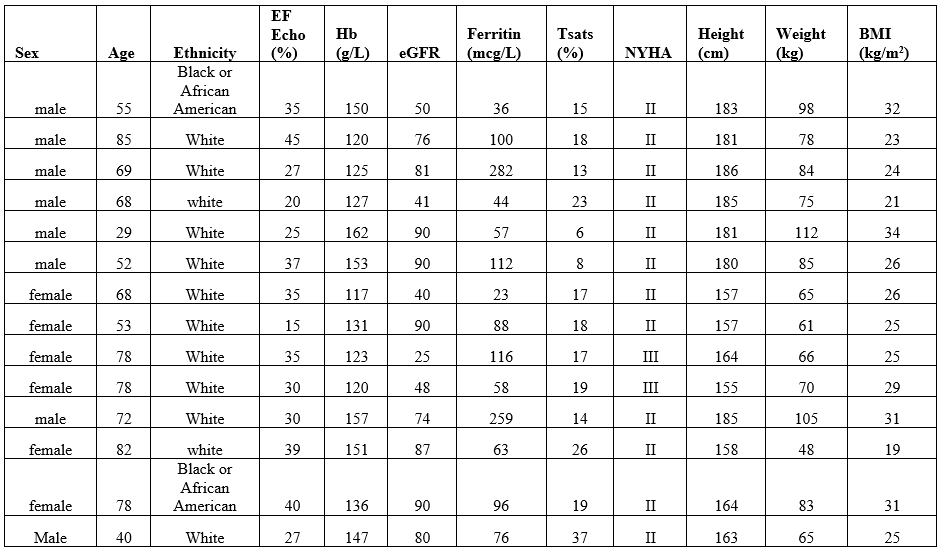
14 patients (6 female; age 63±17y) were recruited (table 1). EF was 37±9%, ferritin 103±80mcg/L, and Hb 136±16mg/dL. Absolute ID (ferritin <100mcg/L) was present in 9, functional ID (ferritin 100-299 mcg/L and Tsats<20%) in 5 patients. Iron repletion resulted in improvements in left ventricular EF (by 6±6%, p=0.01), and an improvement in 6-minute-walk-distance by a mean of 46m (362±129 m to 408±110 m, p=0.02). There was no significant improvement in short-KCCQ (51 to 55, p=0.161). Myocardial PCr/ATP was low in HF patients (n=12) at rest (1.55±0.3 vs 1.94±0.34 in internal control database- unpublished), with no significant change with stress (-12%, 1.57±0.3 to 1.39±0.39, p=0.9154). There was no significant change in rest or stress myocardial PCr/ATP following iron infusion (follow-up rest -13±69%, p=0.272, follow up stress 17±45%, p=0.397). Following repeated plantar flexion at 25% MVC (n=8), skeletal muscle PCr consumption (baseline 71±20% vs post iron 69±19%, p=0.54), end-exercise intracellular pH (6.77±0.19 vs post iron 6.79±0.19, p=0.74), and PCr recovery rate (τPCr = 96±71s vs 72±29s, p=0.24) were not significantly different after iron repletion.Conclusion
Treatment of symptomatic patients with HF with reduced EF and ID, resulted in a 6% improvement in EF and a significant increase in 6-minute-walk distance. The increase in ejection fraction after FCM will have resulted in an increase in ATP requirement. Despite this there was no change in PCr/ATP. We therefor hypothesise that FCM resulted in either increase in energy efficiency, or improved flux through Creatine Kinase, which was not assessed during this study. Increased exercise capacity as measured by 6MWT may be related to both cardiac and peripheral factors.Acknowledgements
This study was supported by the Oxford BHF Centre of Research Excellence. SB is funded by a BHF programme grant (HSR01480). LV is funded by a Sir Henry Dale Fellowship awarded jointly by the Wellcome Trust and the Royal Society (221805/Z/20/Z) and also acknowledges the support of the Slovak Grant Agencies VEGA (2/0004/23) and APVV (#21–0299).References
No reference found.Figures