1776
Cardiac protocol including 1H 3T MRI and 31P MRSI 7T with a dipole array coil1University of Cambridge, Cambridge, United Kingdom, 2Department of Cardiovascular Medicine, University of Cambridge, Cambridge, United Kingdom, 3Royal Papworth Hospital, Cambridge, United Kingdom, 4Department of Radiology, University of Cambridge, Cambridge, United Kingdom, 5UMC Utrecht, Utrecht, United Kingdom
Synopsis
Keywords: Heart Failure, Cardiomyopathy
Motivation: 31P heart applications can be used to monitor cardiac energetics, treatment response in vivo and metabolic inflexibility, a key feature of the failing heart.
Goal(s): We present here a 7T and 3T protocol for 31P heart application, including the validation of a dipole array coil design.
Approach: We evaluated the performance of the coil at 7T with B1 maps and through in vivo scans of 8 healthy with a long 31P CSI protocol, and tested the 3T protocol on 5.
Results: Results show spectra of excellent quality. PCr/gATP ratios lie within the expected range and B1+ maps show good uniformity.
Impact: This coil design has the potential of lifting the current limitations associated with the wider use of 31P cardiac MRSI to study the heart energetics. It can also help the diagnosis and the design of new drugs in the future.
Introduction
Metabolic inflexibility is a key feature of the failing heart, with myocardial metabolism a promising therapeutic target in heart failure.Phosphorus (31P) MRSI monitors cardiac energetics in vivo. Previous studies have shown that the PCr/ATP ratio predicts mortality [1], however widespread use in clinical trials has been hampered so far by relatively low sensitivity and spatial resolution.
We set out to solve these limitations by applying our dipole array coil for ultra-high field (7T) 31P-MRSI. We aim to correlate the 7T 31P metabolic information with 3T volume and ejection fraction analysis on the same heart failure patients.
We show here the performance of such an array on phantoms and 8 healthy volunteers, and the 3T protocol tested on 5 volunteers, ahead of a forthcoming study in heart failure patients.
Methods
The full study protocol consists of 7T 31P -MRSI to assess cardiac energetics, and a 3T-MRI scan to quantify cardiac volumes and ejection fractions. The protocols are detailed in Figure 1.7T protocol:
We previously described the construction of our novel transmit/receive dipole array with 8Tx/24Rx for 31P and 8 Tx/Rx for 1H [2]. For this study, we transmitted with the four central 31P dipoles which cover the heart (Fig. 3b)).
A total of 8 volunteers consented to an in vivo 7T Terra MRI (Siemens) scan (5 males, 3 females, 24-55 y/o) with a 28-min 31P-CSI scan as previously described [3,4], (1s TR, 16x16x8 3D matrix, 35x35x30 cm3 FOV). We used a 450V shaped excitation pulse [5] (Fig. 4f).
A 31P fiducial containing phenylphosphonic acid (PPA) dissolved in ethanol with Cr(acac)3 to reduce T1 was mounted inside the coil housing (Fig. 2). The B1 calibration scans consisted of inversion-recovery and voltage sweep FID sequences centred on the PPA frequency to evaluate the T1, the B1+ at the fiducial position, and the reproducibility across scans.
To evaluate experimentally the flip angle at heart depth, B1+ maps were acquired on a phantom containing 26 litres of distilled water, 78g NaCl, and 150g H2KPO4 (Fig. 3a). Maps were fitted to a series of nine 3D CSI scans (32x32x8 matrix, 45x45x30 cm3 FOV, 4ms block pulse,1s TR). Additionally, a 50mL tube with 0.5M (PPA) solution (f at 17ppm from H2KPO4 frequency) was placed in the centre of this shaft to enable for a single point B1+ value with an acquisition frequency centred on PPA (5ms block pulse FID acquisitions at 50-350 V, 1s TR), and with the fiducial temporarily dismounted from the coil housing.
Data were processed in Matlab using an extended version of OXSA [6]. The mid-septal voxel was selected and its spectrum was fitted with AMARES to compute metabolite SNRs and the corrected PCR/γATP ratio for blood contamination or partial saturation. We also re-processed data from a previously published study using a 16-element loop array using our new analysis pipeline for comparison [4].
3T protocol:
Five healthy volunteers were scanned (3 females, 2 males, 24-55 y/o) with a 3T Prisma MRI (Siemens), an anterior 18-channel surface and a posterior 32-channel spine coils.
Data were processed using the CardioVascular Imaging software (CVI42, Calgary, Canada) to extract the volumes and the left ventricular ejection fraction (LVEF).
Results & Discussion
The B1+ maps show good uniformity around the position of the heart (Fig. 3a), but are 65 % less efficient compared to the simulations [2], which is probably due to the loss from hardware and cables. The B1 was fitted from the PPA tube in the center, which is at about heart depth (Fig. 3c). We believe to reach a flip angle of around 25o.Spectra from the dipole array coil are of excellent quality (Fig.4b-c-d-e). The αATP resonance has a phase shift due to the shaped excitation pulse. The dipole array coil has improved coverage for 1H-MRI (Fig 4a).
Comparing to the loop array: PCr linewidths were 35 ± 5 Hz for the dipole coil vs 40 ± 20 Hz previously[4]. The dipole array coil shows significantly increased SNR/mL for both metabolites (Fig. 5a, p=0.03 PCr, p=0.007 ATP). The corrected PCr/γATP ratio is consistent (p=0.99) and lies in the expected range [1,3-5]. 3T data analysis (Fig. 5a-b) shows that the LVEF of the healthy volunteers are within the normal range.
The T1 of the fiducial were 0.143 ± 0.013 ms and the B1+ of the fiducial were 0.47 ± 0.046 deg/V, making it very reproducible.
Conclusion
Dipole array coils present a promising new approach for human cardiac 31P -MRSI at 7T. Their improved SNR may increase the power of clinical trials measuring energetics by 31P -MRSI at 7T.Acknowledgements
Jabrane Karkouri was supported by the EU Horizon 2020 program under grant agreement #801075 “NICI” and by Innovate UK (10032205) under the Guarantee Scheme relating to the EU Horizon Europe project MITI (101058229). This research was supported by the NIHR Cambridge Biomedical Research Centre (BRC-1215-20014). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care. Will Watson is funded by a University of Cambridge lectureship.References
1. Neubauer S, Horn M, Cramer M, Harre K, Newell JB, Peters W, Pabst T, Ertl G, Hahn D, Ingwall JS, Kochsiek K. Myocardial phosphocreatine-to-ATP ratio is a predictor of mortality in patients with dilated cardiomyopathy. Circulation. 1997 Oct 7;96(7):2190-6. doi: 10.1161/01.cir.96.7.2190. PMID: 9337189.
2. Ria Forner, Jabrane Karkouri et. al., B1 efficiency of a dipole array coil for body application. In: Proceedings of the 2022 Joint Annual Meeting ISMRM-ESMRMB & ISMRT 31st Annual Meeting. ; 2022:2291.
3. Rodgers CT, Clarke WT, Snyder C, Vaughan JT, Neubauer S, Robson MD. Human cardiac 31P magnetic resonance spectroscopy at 7 Tesla. Magn Reson Med. 2014 Aug;72(2):304-15. doi: 10.1002/mrm.24922. Epub 2013 Sep 4. PMID: 24006267; PMCID: PMC4106879.
4. Ellis J, Valkovič L, Purvis LAB, Clarke WT, Rodgers CT. Reproducibility of human cardiac phosphorus MRS (31 P-MRS) at 7 T. NMR Biomed. 2019 Jun;32(6):e4095. doi: 10.1002/nbm.4095. Epub 2019 Mar 29. PMID: 30924566; PMCID: PMC6546607.
5. Tyler, D.J., Emmanuel, Y., Cochlin, L.E., Hudsmith, L.E., Holloway, C.J., Neubauer, S., Clarke, K. and Robson, M.D. (2009), Reproducibility of 31P cardiac magnetic resonance spectroscopy at 3 T. NMR Biomed., 22: 405-413. https://doi.org/10.1002/nbm.1350
6. Purvis LAB, Clarke WT, Biasiolli L, Valkovič L, Robson MD, et al. (2017) OXSA: An open-source magnetic resonance spectroscopy analysis toolbox in MATLAB. PLOS ONE 12(9): e0185356.Figures
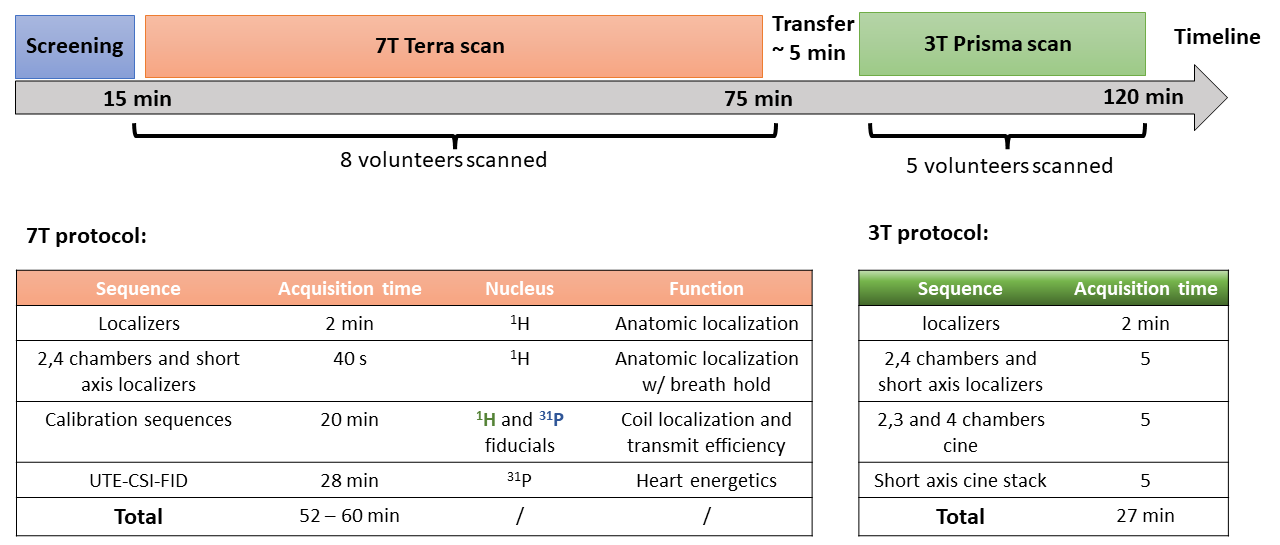
Figure 1: Study protocol timeline including 7T 31P MRSI scans followed by a 3T anatomical scan. The total time of the protocol is around 2h. The 7T and 3T protocols are detailed and enable to study the heart energetics and anatomy.
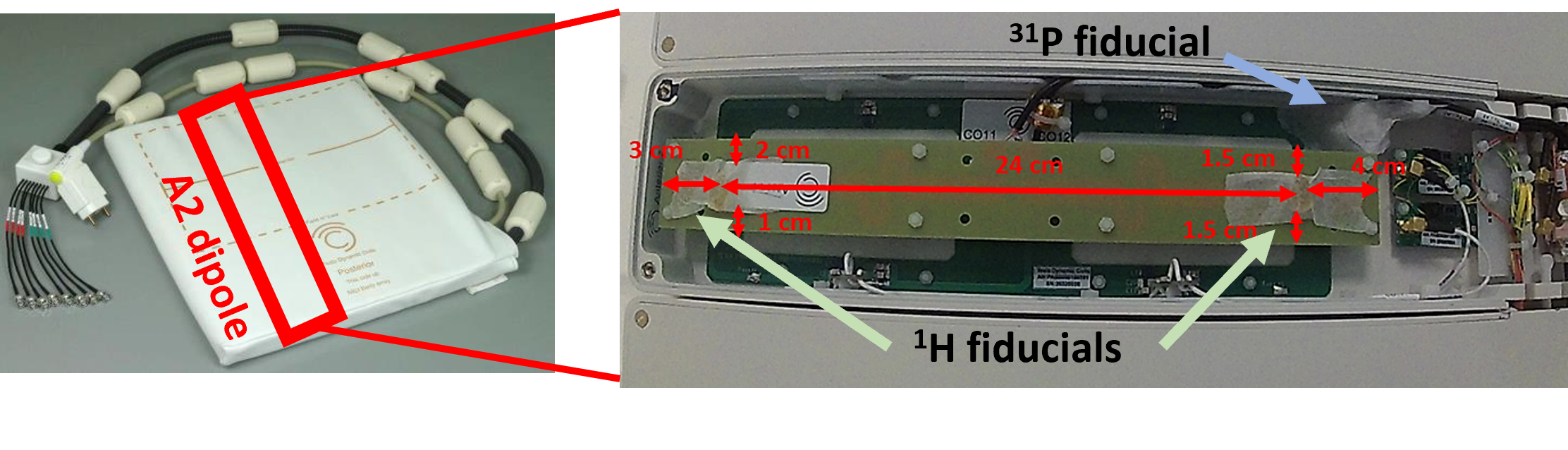
Figure 2: Photograph of the anterior part of the dipole array, as well as the positions of the 1H and 31P fiducials inside the coil housing used for the calibration acquisitions.
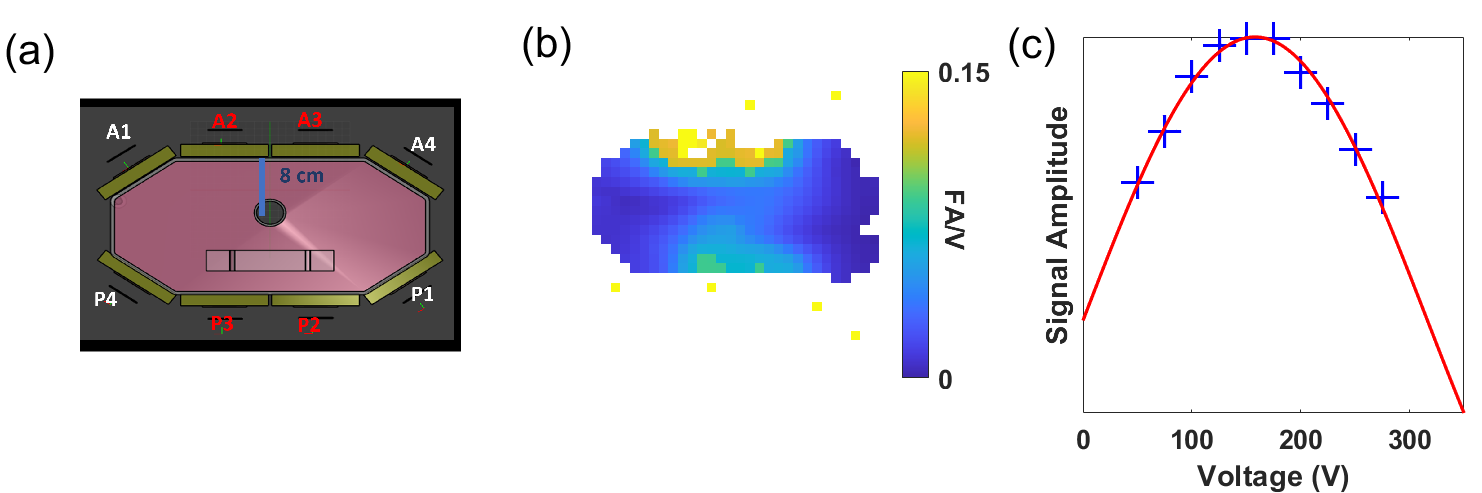
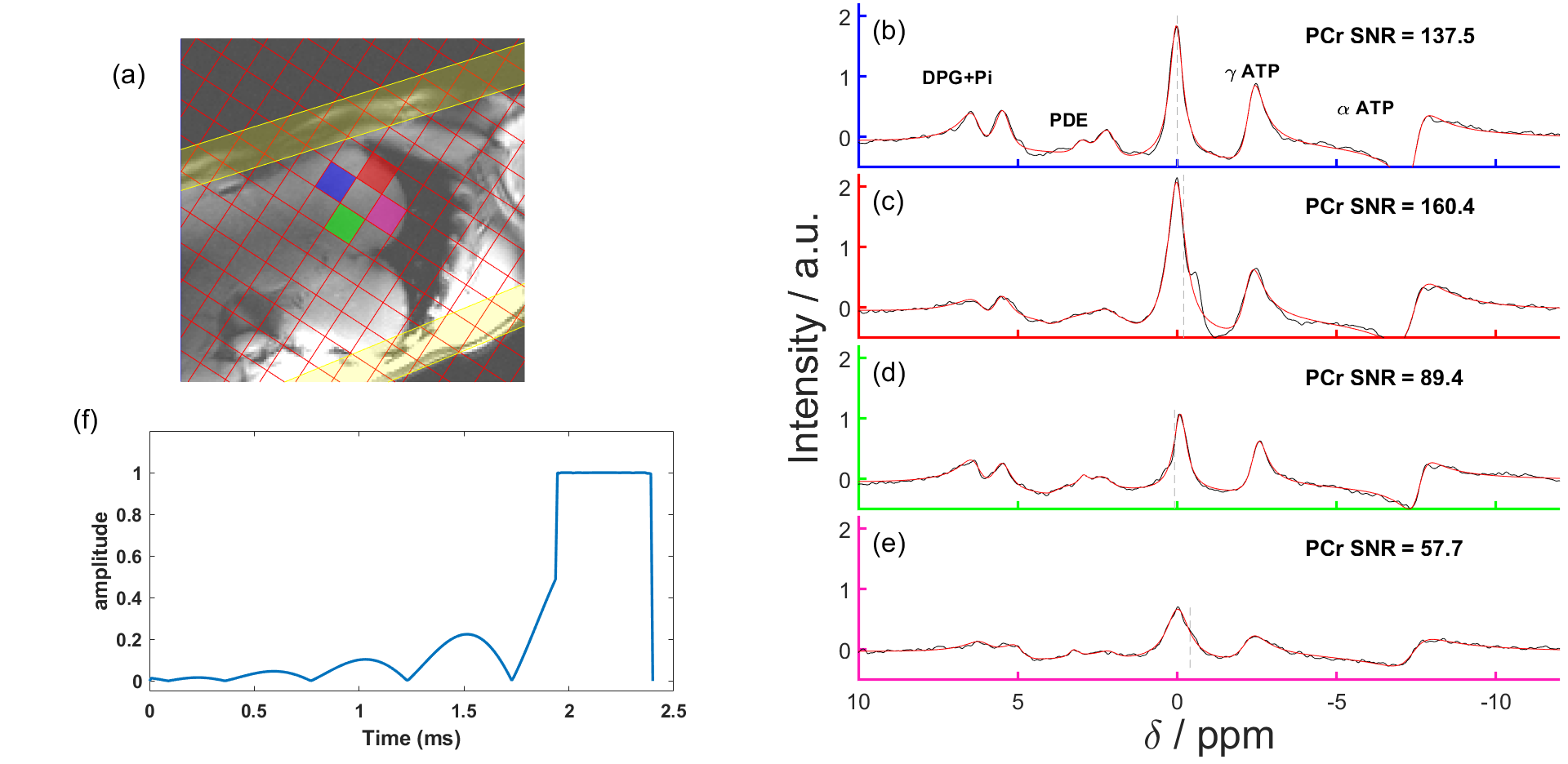
Figure 4: Example data with the dipole array coil. (a) localiser images overlaid with the CSI matrix and with the chosen mid-septal voxels highlighted. (b), (c) and (d) spectrum from the highlighted voxels (in black) and AMARES fit (in red). There is excellent resolution of PCr and γATP. Note that αATP has a phase distortion because it lies outside the bandwidth of our shaped excitation pulse [3,4]. (f) Amplitude of the shaped pulse used for our CSI acquisition.
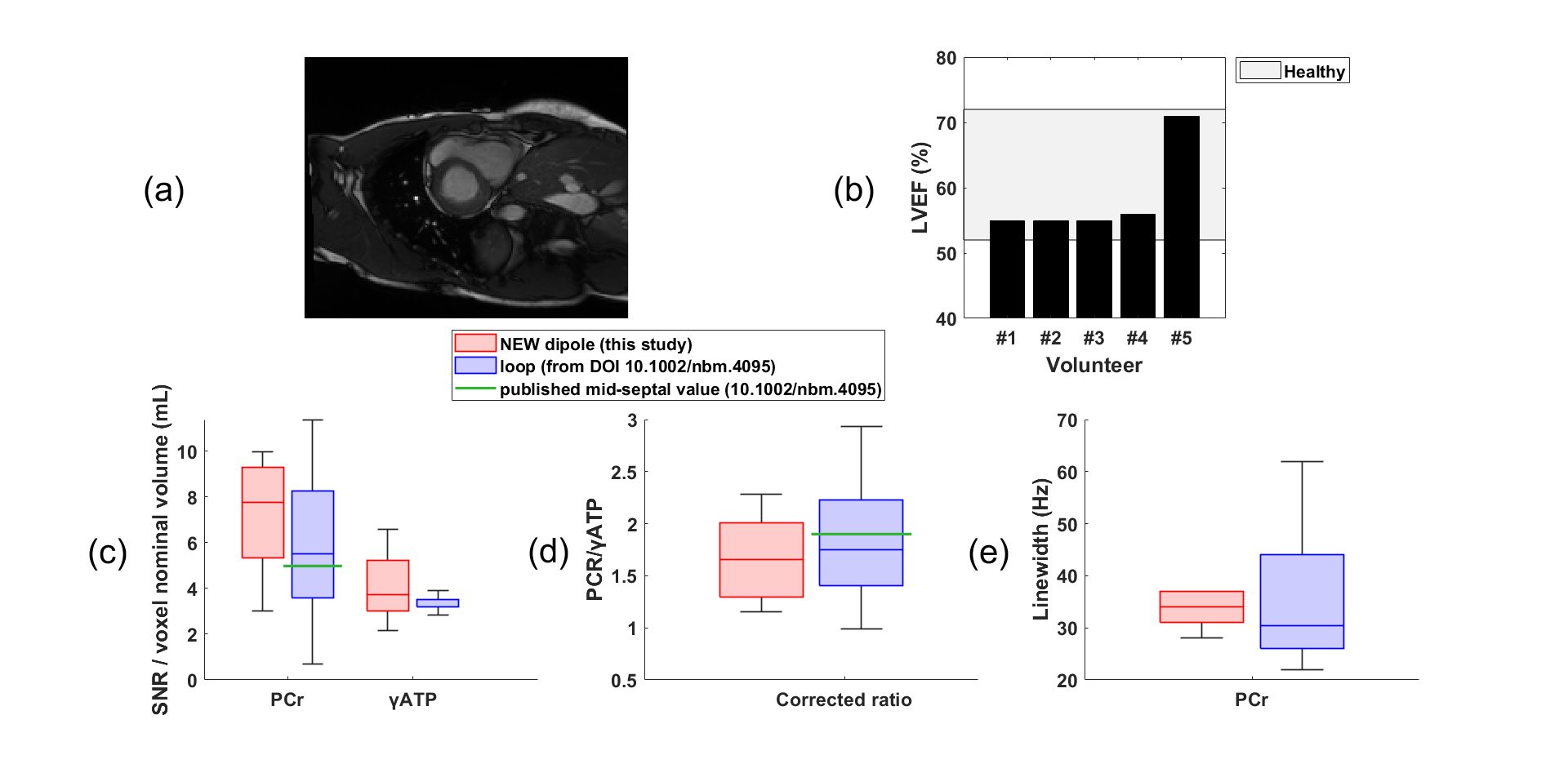
Figure 5: (a) Short-axis image acquired at 3T. (b) shows the Left Ventricular Ejection Fraction (LVEF) range for all the healthy volunteers. Comparison of results from the dipole array coil to those from the loop coil used in Ellis et al [4]. (c) SNR for PCr and ATP is significantly increased for the dipole array coil. The green line shows the published PCr SNR from the Ellis et al study confirming that our new processing pipeline assesses SNR equivalently. (d) Corrected PCr/γATP ratio for blood or partial saturation. (e) PCr linewidth is lower with the dipole array compared to the loop coil.