1775
Measuring Glycolysis and Glucose Oxidation Coupling in Hypertrophic Cardiomyopathy Patients using Hyperpolarized [1-13C]-Pyruvate MRI1UCSF, San Francisco, CA, United States, 2Vista.ai, Palo Alto, CA, United States, 3University of Colorado School of Medicine, Boulder, CO, United States, 4University of Pennsylvania, Philadelphia, PA, United States, 5University of Washington, Seattle, WA, United States
Synopsis
Keywords: Myocardium, Cardiomyopathy
Motivation: Alterations in cardiac metabolism are implicated in numerous heart diseases, including cardiomyopathies, heart failure, and ischemic disease. Patients with hypertrophic cardiomyopathy (HCM) have known dysregulation of cardiac metabolism and energetics, and studies group aim to provide non-invasive measurements of dysregulation to allow for earlier diagnoses as well as monitoring of treatments.
Goal(s): In this project, we aim to translate HP 13C-MRI into human studies of cardiac metabolism.
Approach: This project will include studies of healthy subjects for normative values as well patients with HCM.
Results: Preliminary results show clear abnormalities in metabolic imaging but no one metabolic phenotype across all five HCM patients
Impact: In this project, we aim to translate HP 13C-MRI into human studies of cardiac metabolism. Alterations in cardiac metabolism are implicated in numerous heart diseases, including cardiomyopathies, heart failure, and ischemic disease.
Introduction
Hyperpolarized (HP) 13C-pyruvate MRI is a promising new tool for non-invasive quantification of myocardial glycolytic and TCA cycle metabolism1,2. Patients with hypertrophic cardiomyopathy (HCM) exhibit a range of metabolic phenotypes and genotypes3. While standard-of-care cardiac magnetic resonance (CMR) provides information on physical form and function, it does not offer metabolic information on tissue, but such information would aid in diagnosis and translation of metabolic therapies. This abstract shares HCM patient studies with HP [1-13C] pyruvate to study TCA metabolism and metabolic flexibility in HCM patients, with comparisons to normal values from healthy volunteers.Methods
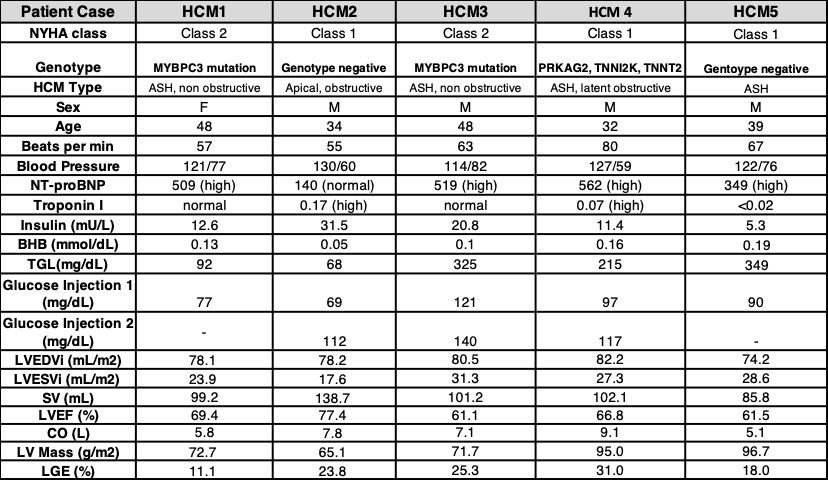
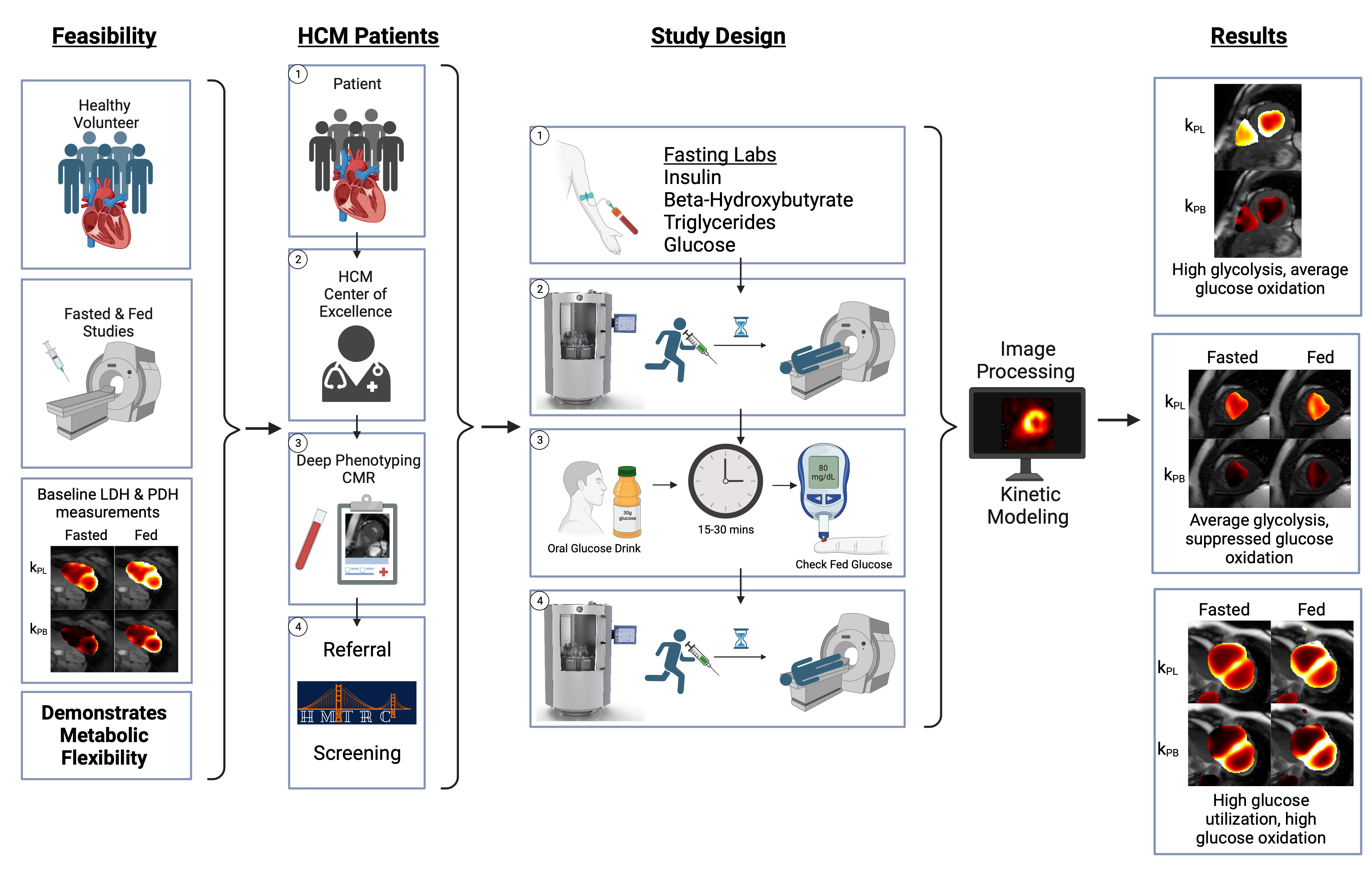
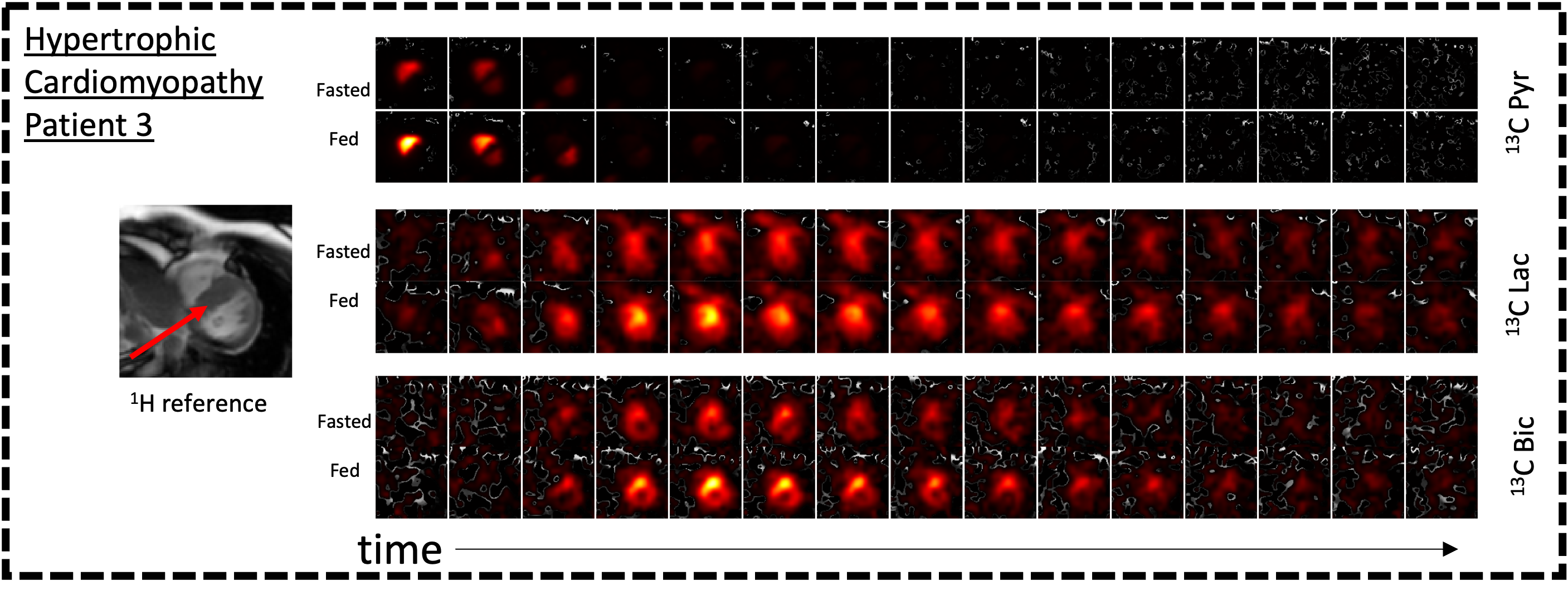
In this ongoing study, 5 HCM patients (40 ± 8 yrs) and 7 healthy volunteers (34 ± 8 yrs) were injected with HP [1-13C] pyruvate and scanned at 3T. The HCM patients were referred to the study from the UCSF HCM Center of Excellence, where deep clinical phenotyping and clinical CMR are performed (Fig 1). Three patients participated in a fed/fasted protocol where they were asked to fast for a minimum of 4 hours prior to the first injection, and were given an oral glucose solution (30g glucose) prior to the second injection. One patient fasted for 4 hours prior to a single injection, and one patient was uncontrolled. The HP [1-13C] pyruvate scan used an autonomous scanning protocol including metabolite-specific imaging using a spectral-spatial pulse and spiral readout to acquire 2D short-axis images, 13C-bicarbonate and [1-13C] lactate in-plane resolution: 12x12mm, [1-13C] pyruvate in-plane resolution: 6x6mm, slice thickness: 21mm, temporal resolution: 3 heartbeats (~3.6s), FA: 20° (pyruvate), 30°(lactate and bicarbonate) (Fig 2)4,5,6,9. We performed pharmacokinetic modeling using in-house MATLAB code to assess the conversion of pyruvate-to-lactate (kPL) and pyruvate-to-bicarbonate (kPB) in manually drawn ROIS7,8,9. Representative dynamic images of each metabolite in the fasted and fed state are shown (Fig 3).Results
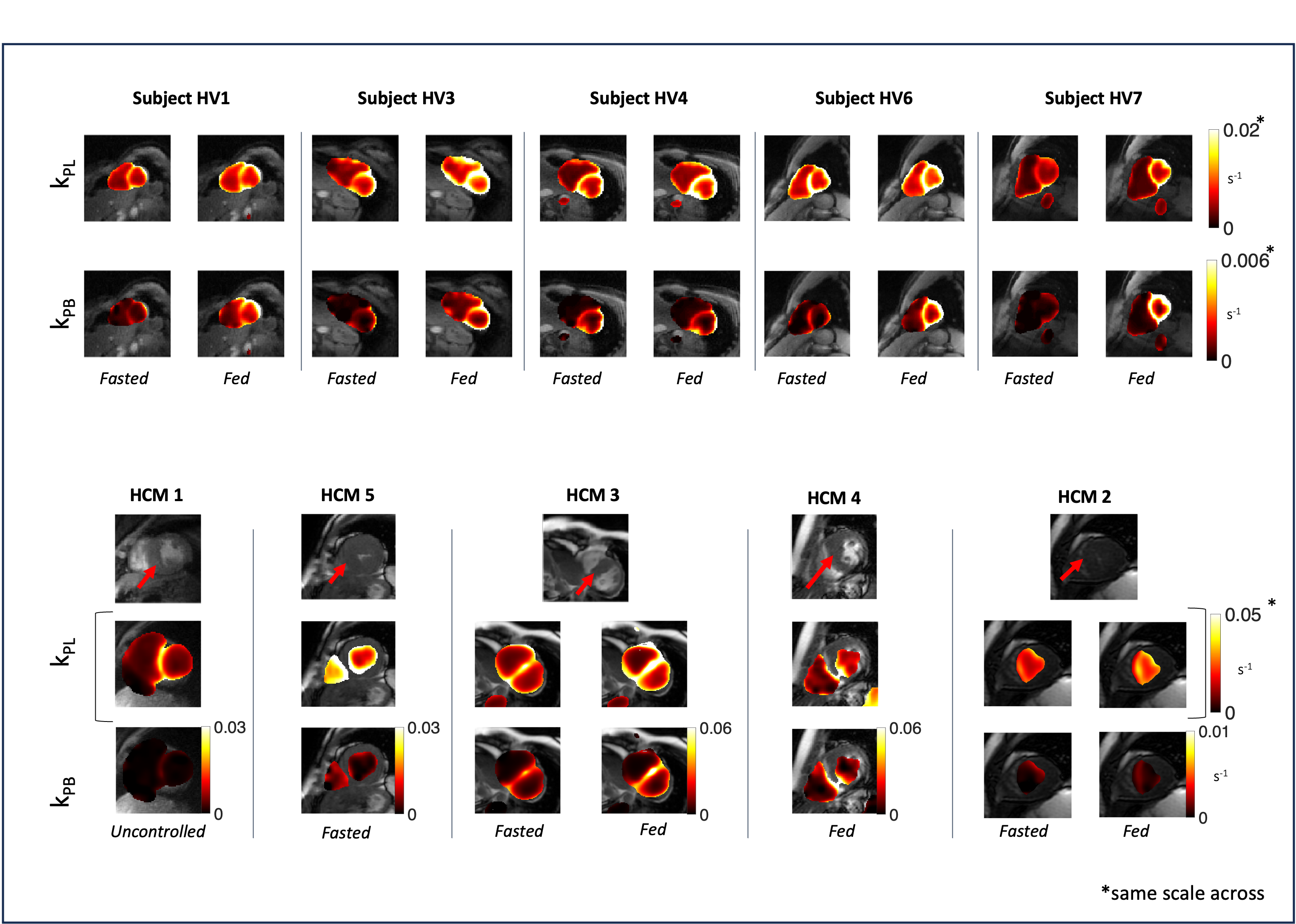
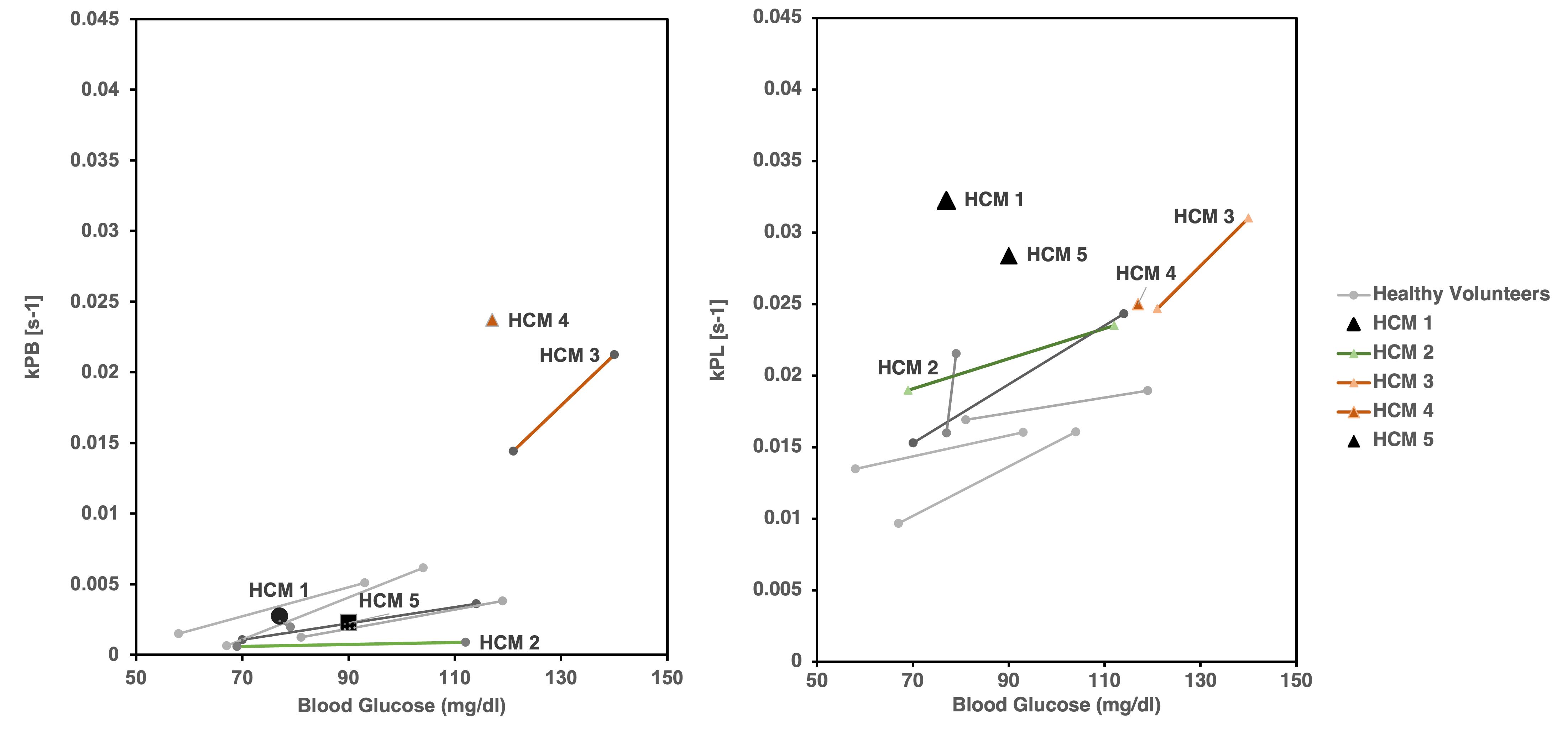
We analyzed metabolism in the myocardium and areas of hypertrophy, the largest differences were seen in areas of hypertrophy. In healthy volunteers, kPB, corresponding to PDH flux, had the highest, statistically significant correlation with blood glucose level, while kPL, corresponding to LDH activity, was modestly correlated with blood glucose measurements. In comparison, 2 HCM patients with one injection each had high kPL and average kPB (Fig 4). Two HCM patients displayed high kPL and kPB in both fasting and fed states. One HCM patient displayed a low kPB with no response to oral glucose, and moderate response in kPL.Discussion
The metabolically flexible heart switches from use of fatty acids in the fasting state to use of glucose in the fed state, observed in the statistically significant kPB increase across healthy volunteers that responded to oral glucose (Fig 5). This represents strong coupling between glycolysis and glucose oxidation: when there is more glucose available and glycolysis increases, the PDH flux indicates increased glucose oxidation. In the hypertrophied segments of the HCM patients, however, we observed glycolysis-glucose oxidation uncoupling. In HCM 1 & 5, elevated kPL and average kPB suggest upregulated GLUT1 & LDHA, promoting insulin-independent glucose uptake and cytosolic lactate production. This is indicative of glycolysis-glucose oxidation uncoupling. At fasting HCM 3 exhibits high insulin levels, yet their fasting kPB indicates high glucose oxidation, surpassing healthy volunteers. In the fed state, HCM 4 has a kPB much higher than healthy volunteers. We hypothesize GLUT1 upregulation of PDH by high energy demands. HCM 2 exhibits low kPB in both fasting and fed states, showing no response to oral glucose solution, potentially indicating suppressed glucose oxidation and uncoupling of glycolysis and glucose oxidation.The HCM patients presented interesting results as there were clear abnormalities in the metabolic imaging but no one metabolic phenotype across all five HCM patients. Further studies are needed to characterize the various genotypes.
Acknowledgements
We would like to acknowledge assistance with hyperpolarized experiments from Kimberly Okamoto, Mary Frost, Heather Daniel, Duy Dang, Yaewon Kim, Andrew Riselli, and Evelyn Escobar. This work was supported by funding from a UCSF Resource Allocation Program Team Science award, Myokardia Inc. Myoseeds program and NIH grants R33HL161816, P41EB013598, and U24CA253377. ND received postdoctoral training funding from the American Heart Association (grant number 20POST35200152)References
[1] Agger, Peter, et al. “Magnetic Resonance Hyperpolarization Imaging Detects Early Myocardial Dysfunction in a Porcine Model of Right Ventricular Heart Failure.” European Heart Journal - Cardiovascular Imaging, vol. 21, no.1, 2019, pp. 93–101., https://doi.org/10.1093/ehjci/jez074.
[2]Timm, Kerstin N., Jack J. Miller, John A. Henry, and Damian J. Tyler. “Cardiac Applications of Hyperpolarised Magnetic Resonance.” Progress in Nuclear Magnetic Resonance Spectroscopy 106–107 (June 1, 2018): 66–87. https://doi.org/10.1016/j.pnmrs.2018.05.002.
[3] Vakrou S, Abraham MR. Hypertrophic cardiomyopathy: a heart in need of an energy bar? Front Physiol. 2014;5:309. PMCID: PMC4137386
[4] Tang S, Milshteyn E, Reed G, Gordon J, Bok R, Zhu X, Zhu Z, Vigneron DB, Larson PEZ. A regional bolus tracking and real-time B1 calibration method for hyperpolarized 13 C MRI. Magn Reson Med. 2019 Feb;81(2):839–851. PMCID: PMC6289616
[5] Cunningham CH, Lau JYC, Chen AP, Geraghty BJ, Perks WJ, Roifman I, Wright GA, Connelly KA. Hyperpolarized 13C Metabolic MRI of the Human HeartNovelty and Significance: Initial Experience. Circ Res. 2016 Nov 11;119(11):1177–1182. PMID: 27635086
[6] Gordon JW, Autry AW, Tang S, Graham JY, Bok RA, Zhu X, Villanueva-Meyer JE, Li Y, Ohliger MA, Abraham MR, Xu D, Vigneron DB, Larson PEZ. A variable resolution approach for improved acquisition of hyperpolarized 13 C metabolic MRI. Magn Reson Med. 2020 Dec;84(6):2943–2952. PMCID: PMC7719570
[7] Larson PEZ, Chen HY, Gordon JW, Korn N, Maidens J, Arcak M, Tang S, Criekinge M, Carvajal L, Mammoli D, Bok R, Aggarwal R, Ferrone M, Slater JB, Nelson SJ, Kurhanewicz J, Vigneron DB. Investigation of analysis methods for hyperpolarized 13C-pyruvate metabolic MRI in prostate cancer patients. NMR Biomed. 2018 Nov;31(11):e3997. PMID: 30230646
[8] Hyperpolarized-MRI-Toolbox [Internet]. Available from: https://github.com/LarsonLab/hyperpolarized-mritoolbox doi: 10.5281/zenodo.1198915
[9] Larson PEZ, Tang S, Liu X, Sinha A, Dwork N, Sivalokanathan S, Liu J, Bok R, Ordovas KG, Slater J, Gordon JW, Abraham MR. Regional quantification of cardiac metabolism with hyperpolarized [1 - 13 C]-pyruvate MRI evaluated in an oral glucose challenge. medRxiv [Preprint]. 2023 Oct 19:2023.10.16.23297052. doi: 10.1101/2023.10.16.23297052. PMID: 37904936; PMCID: PMC10615005.
Figures