1761
Unsupervised Neural Network for Super-Resolving Non-Contrast-Enhanced Whole-Heart MRI Using REACT1Pediatrics, University of Texas Southwestern Medical Center, Dallas, TX, United States
Synopsis
Keywords: Other AI/ML, Machine Learning/Artificial Intelligence, Super-resolution, Heart
Motivation: Three-dimensional (3D) whole-heart MRI requires long scan times and the sequence used to acquire such scans is susceptible to banding artifacts.
Goal(s): The goal of this study was to develop an unsupervised super-resolution neural network for 3D whole-heart MRI.
Approach: The data used in this study was acquired using a modified Relaxation-Enhanced Angiography without Contrast and Triggering (REACT) sequence. A neural network referred to hereafter as the Super-resolution Neural Network (SRNN) was developed to super-resolve 3D MRI data.
Results: The SRNN allows us to acquire lower-resolution scans, thus decreasing scan time, and provides improved image quality after performing super-resolution.
Impact: The results of this study show that super-resolution offers a viable option to decrease scan time and improve overall image quality in 3D whole-heart MRI.
Background
The reliable and accurate tool used to check cardiac anatomy and pathology for congenital or acquired heart disease is 3D whole-heart MRI1. This technique offers a few benefits, but there are some weaknesses as well. One, is that this technique requires a long scan time1. Another, is that sequence used in the technique, balanced Steady-State Free Procession (bSSFP), is susceptible to banding artifacts2. The application of the SRNN together with the modified REACT sequence offers the potential to mitigate these issues. By using the SRNN we can acquire low-resolution (LR) scans, which decreases the scan time. Furthermore, the neural network upon which the SRNN is based implements denoising within the neural network, thus in the process of super-resolving an image it also eliminates noise and suppresses artifacts.Methods
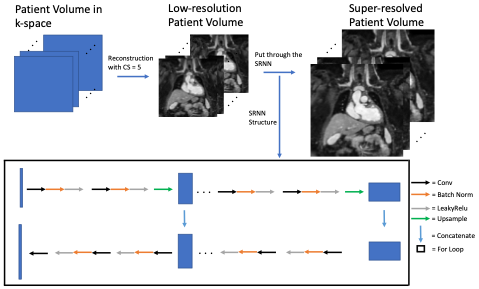
All the data was acquired on a 1.5 T scanner (Philips Healthcare, Best, Netherlands). We employ a 3D magnetization-prepared non-balanced dual-echo Dixon technique, combined with cardiac triggering and respiratory navigation. The process initiates with magnetization preparation, which involves a four-pulse adiabatic-based T2-preparation module followed by a non-volume-selective short tau inversion recovery (STIR) pre-pulse with brief inversion time (TI). Following this, we implement a 3D modified two-point chemical-shift water-fat separation turbo-field echo pulse sequence, known as mDIXON TFE. Specific sequence parameters for our data acquisition include: TE1 / TE2 / TR = 2.0 ms / 4.7 ms / 7.2 ms; Flip angle = 15o ; Compressed sensing factor = 5; Slice orientation is set as Coronal; TFE shot interval is dependent on patients' heart rate.In this work, we adopted the DIP3 framework for 3D whole-heart imaging super-resolution. In the acquisition of low-resolution MR images, high spatial resolution is maintained in the kz direction, which corresponds to the axial slice orientation. Conversely, the coronal and sagittal directions are captured with low spatial resolution. Consequently, in the simulation data used for this study, we only down-sample the coronal and sagittal directions. As the axial direction retains high spatial resolution, we employ a slice-by-slice super-resolution approach, applying super-resolution exclusively to the coronal and sagittal directions. To achieve this, we employ a neural network featuring skip connections3 to generate high-resolution images from low-resolution whole-heart images. This network accepts low-resolution images as inputs and produces high-resolution images as outputs. The illustration of this process is shown in Figure 2.
There were 6 patients that were downsampled by a factor of 4 (4X) and 6 patients that were downsampled by a factor of 2 (2X). Furthermore, each of the patient MRI volumes were super-resolved using bilinear interpolation as well as nearest interpolation. The HR MRI volumes resulting from the interpolation methods were then compared to the SRNN HR MRI volumes visually and quantitatively using signal-to-noise ratio (SNR), peak signal-to-noise ratio (PSNR), and structural similarity index measurement (SSIM).
Results
Both quantitative and qualitative comparisons were used to demonstrate the ability of the SRNN to perform the super-resolution task. Quantitatively the SRNN output was compared with the output of nearest and bilinear interpolation using SNR, PSNR, and SIMM. It was also compared with the ground truth HR MRI volumes using SNR. Qualitatively a visual comparison of the output from the SRNN, nearest interpolation, bilinear interpolation, and the ground truth HR patient volume was performed.The results of the quantitative analysis can be seen in Figure 1. Figure 1b shows the results of the SNR calculations. It is observed that the SRNN provides the greatest SNR for every patient. This is especially important to note for Figure 1a where the PSNR and SSIM comparisons are included. Because the ground truth HR images are noisy the lowest PSNR and SSIM may indicate the image with the highest quality.
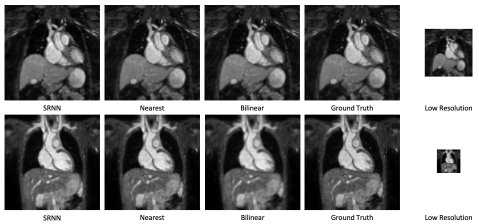
The qualitative comparison can be seen in Figure 3. Figure 3 clearly shows the visual superiority of the SRNN. As an example, in the bottom row of Figure 3 (a 4X patient) the SRNN image is less pixelated than the nearest interpolation image, clearer than the bilinear interpolation image, and less noisy than the ground truth HR image.
Conclusion
In the study, we propose the use of an unsupervised neural network, the SRNN, for the purpose of performing super-resolution in 3D whole-heart MRI. The implementation of the SRNN allows us to decrease scan time and improve image quality.Acknowledgements
No acknowledgement found.References
1. Greil G, Tandon A (Aashoo), Vieira MS, Hussain T. 3D whole heart imaging for congenital heart disease. Front Pediatr. 2017;5(February):1-10. doi:10.3389/fped.2017.00036
2. Balaban RS, Peters DC. Basic Principles of Cardiovascular Magnetic Resonance.; 2018. doi:10.1016/B978-0-323-41561-3.00001-X
3. Ulyanov D, Vedaldi A, Lempitsky V. Deep Image Prior. Int J Comput Vis. 2020;128(7):1867-1888. doi:10.1007/s11263-020-01303-4
Figures
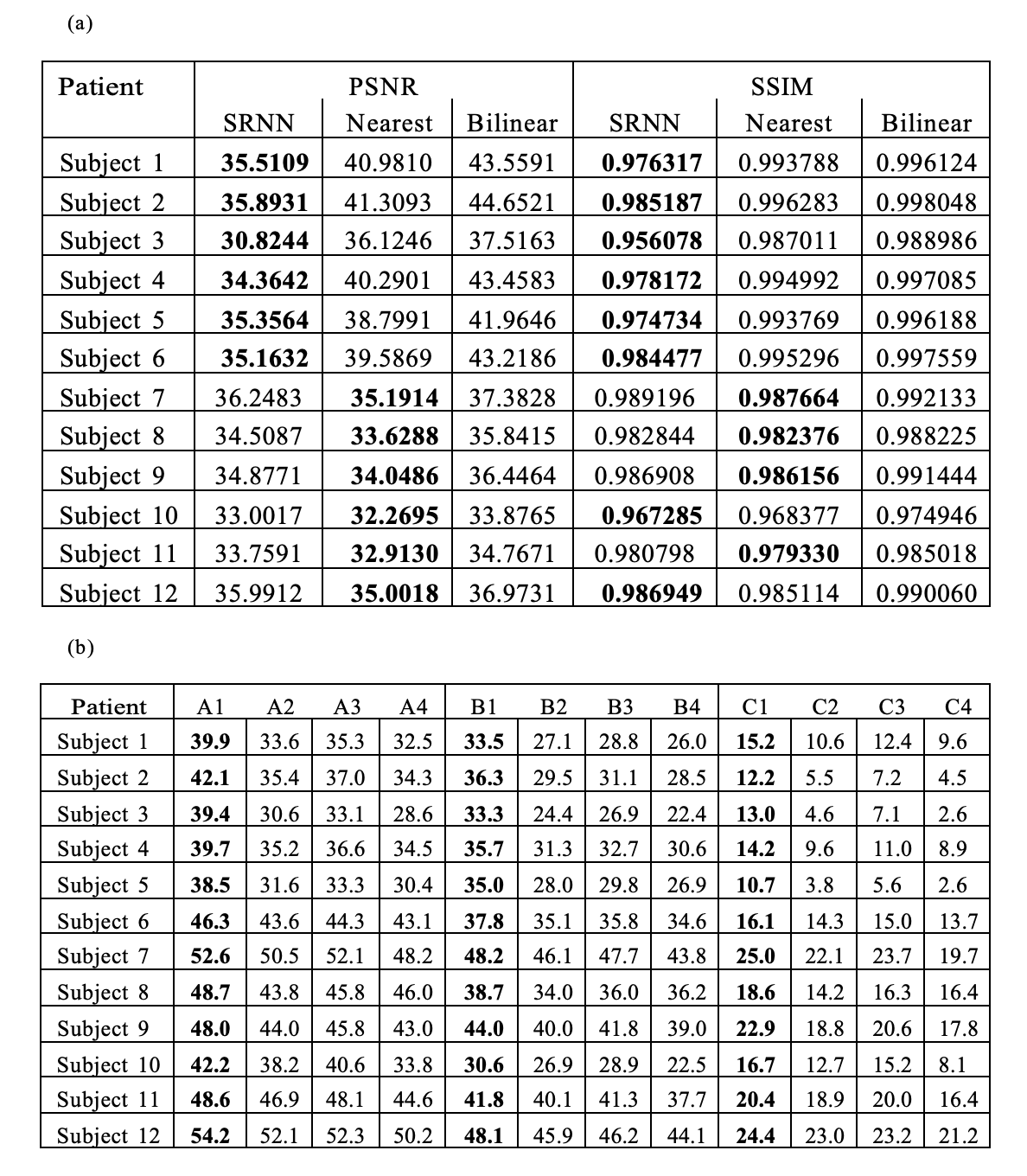
Figure 1:
a: Comparison of PSNR and SSIM for simulation cases. The bold numbers show the lowest PSNR and SSIM for each subject. Due to the noise in the “ground truth” images, low values may indicate higher image quality.
b: Comparison of SNR for simulation cases and the ground truth for the heart, liver, and lung region for each patient. The bold numbers show the largest SNR for that patient and organ.
A = Heart, B = Liver, C = Lung
1 = SRNN, 2 = Nearest, 3 = Bilinear, 4 = Ground Truth