1746
Enhancing Real-Time Cardiac MRI with Image-Domain Diffusion Model for Arrhythmia Patient1University of Pennsylvania, Philadelphia, PA, United States, 2Ohio State University, Columbus, OH, United States
Synopsis
Keywords: AI Diffusion Models, Arrhythmia, Non-cartesian sampling, radial
Motivation: Persistent premature ventricular obscure left ventricle (LV) function assessment. Current imaging lacks temporal resolution and methods for effective differentiation of beat morphologies.
Goal(s): To enhance real-time MRI scans of arrhythmia patients, targeting high temporal resolution for discerning arrhythmia beats.
Approach: We trained an image-domain diffusion model on a public database, optimizing transferability to arrhythmia scans. The model employs prior images during the reverse sampling to impose image-domain constraints.
Results: Achieved a 62% increase in LV signal-to-noise ratio and a 150% increase in LV-to-myocardium contrast-to-noise ratio across 10 real-time scans. Also facilitated direct beat morphology analysis, paving the way for PVC-induced cardiomyopathy studies.
Impact: The trajectory-agnostic diffusion model offers clinicians and patients clearer visualization of real-time arrhythmia scans, potentially assisting the early detection and study of PVC-induced cardiomyopathies. Future research may explore its applicability to other rapid-cycle cardiac phenomena.
Introduction
Cardiac MRI is pivotal for heart function assessment, but arrhythmias like premature ventricular contractions (PVC) cause motion inconsistencies, undermining image quality. While cine MRI with gating excels in stable sinus rhythms, it fails on arrhythmia patients due to its dependence on periodicities [1]. While high temporal resolution is essential for capturing cardiac dynamics, traditional acceleration methods such as parallel imaging and compressed sensing often yield additional artifacts from undersampling [2]. Deep learning methods show promise in reconstructing severely undersampled data, with studies adapting iterative reconstruction algorithms to incorporate priors learned by neural networks [3]. However, these models lack flexibility, requiring retraining for different sampling patterns, and are not feasible for arrhythmia patients due to the absence of multi-shot ground truth data.To solve this problem, we introduce a diffusion-based model to reconstruct undersampled real-time radial MRI scans. Our approach overcomes the constraints of previous techniques and deep learning's reliance on exte nsive ground truth datasets. Our model enhances image quality and offers insights into arrhythmia, and has the potential to improve clinical workflows.
Methods
In this study, we leveraged the Automated Cardiac Diagnosis Challenge (ACDC) dataset for training our diffusion model [4]. The ACDC dataset comprises multi-shot SSFP short-axis cardiac scans from 100 patients, with gating during breath-holds. Each patient's dataset contains 28 to 40 images spanning the cardiac cycle. For uniformity and computational efficiency, these images were preprocessed by padding and downsampling to a resolution of 128x128 pixels. The unsupervised training of our model was conducted following a standard Langevin dynamics process [5,6].For testing, 10 patients with PVC were enrolled under informed consent. Their cine cardiac magnetic resonance (CMR) data was acquired in free-breathing conditions using a multi-slice 2D golden-angle balanced SSFP sequence. Each slice contains 4500 spokes with repetition time of 2.7ms. Model performance was evaluated on a mid-ventricular slice.
Images were initially reconstructed from k-space the Berkeley Advanced Reconstruction Toolbox (BART), employing ESPIRiT for sensitivity map estimation and an L1-wavelet reconstruction (λ = 0.001) [7]. The reconstruction setup achieved a temporal resolution of approximately 19 frames per second using 20 radial spokes per image.
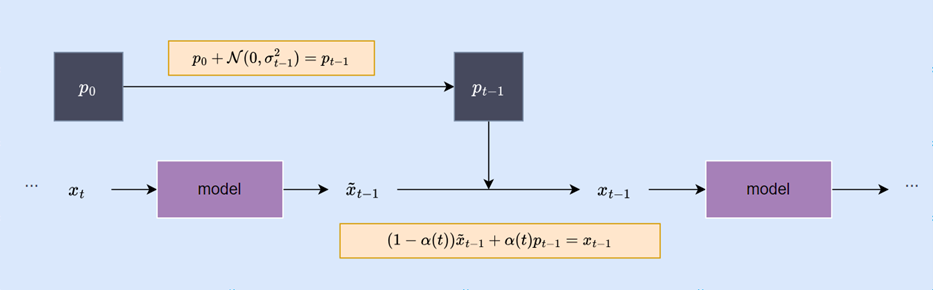
During image sampling, the L1-reconstructed images were introduced as prior to the diffusion model (figure 1). To ensure motion consistency between time frames in the latent space, 5% of the preceding frame was blended into the current frame as preprocessing. At each step of reverse sampling, we sum the noised prior $$$p_{t-1}$$$ with the image latent $$$x_t$$$. The weighting of this sum decreases linearly relative to the timestep, steering the model's output $$$\tilde{x}_{t-1}$$$ towards an image that structurally resembles the prior but has an appearance consistent with the distribution of multi-shot training images $$$p_0$$$. This approach aims to reconcile the differences in data domains, enabling effective application of the trained model to unseen experimental data.
Results
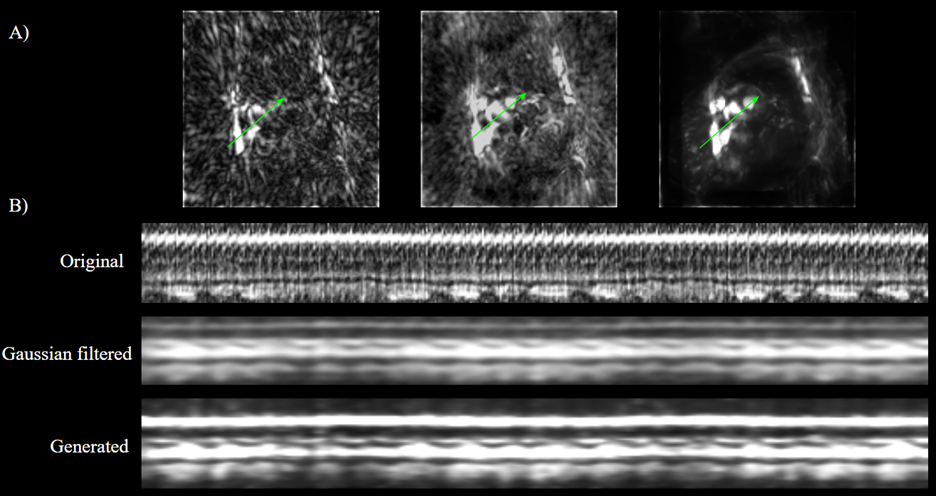
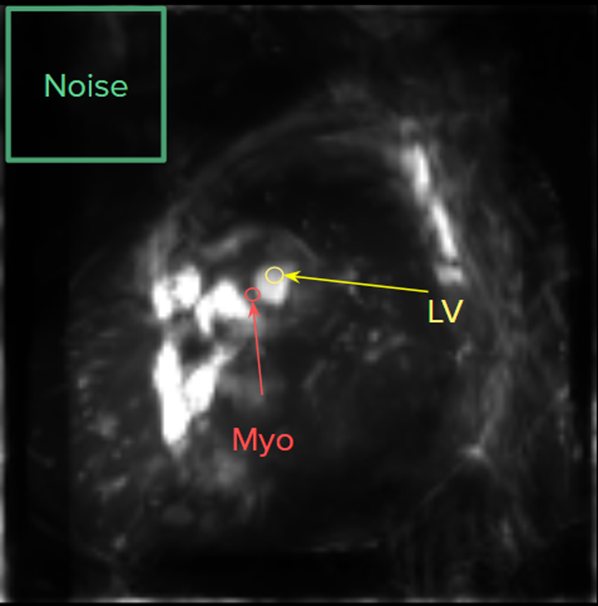
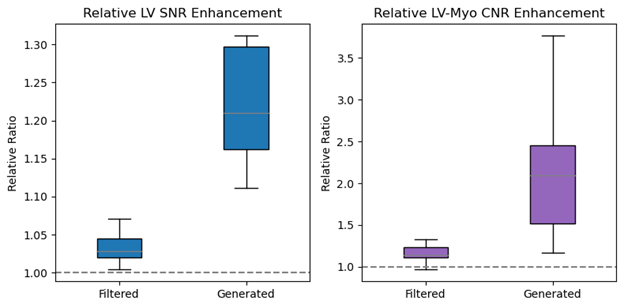
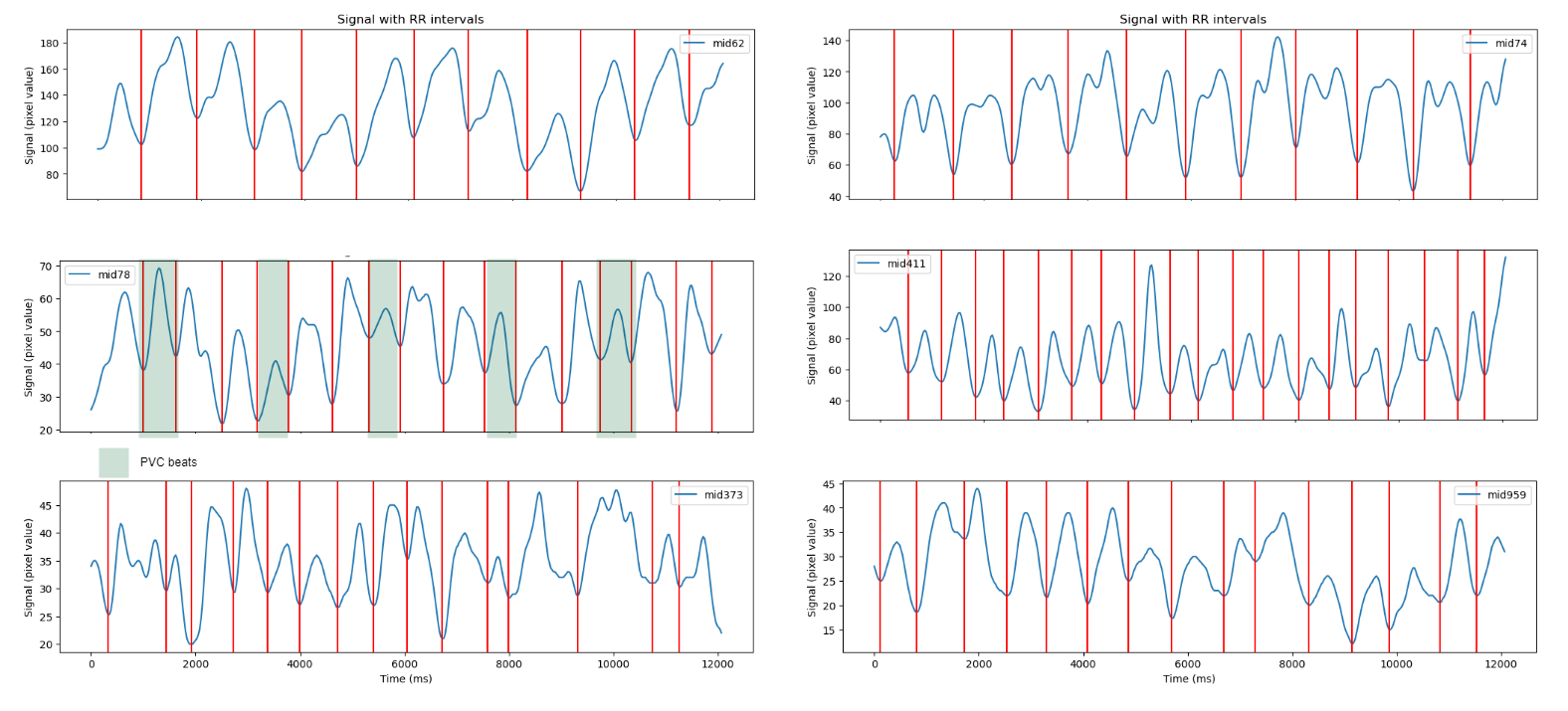
Model effectiveness was quantitatively evaluated by measuring the signal-to-noise ratio (SNR) of the LV and the contrast-to-noise ratio (CNR) between the LV and myocardium. We compared model-generated images to the original L1-reconstructed images. To ensure that enhancements were not solely due to temporal filtering, we also applied a Gaussian temporal filter ($$$\sigma=3$$$) to the L1 images as a control (figure 2). Our model achieved a 62% increase in SNR and a 150% increase in CNR, (figures 3 and 4). Statistical validation through a t-test yielded p-values of 0.060 for SNR and 0.061 for CNR, indicating a marked improvement.Moreover, motion analysis of the diffusion-reconstructed images allowed us to delineate beating intervals, extracting beat morphology information comparable to that from conventional LV segmentation methods (figure 5). This suggests that images reconstructed with our diffusion model may render separate auto-segmentation models for LV redundant, potentially simplifying and accelerating the workflow in arrhythmia research and diagnostics.
Discussion
The diffusion model enhances cardiac MRI quality, but variability and occasional artifacts were noted, particularly when radial streak artifacts overlapped with cardiac structures. This suggests potential challenges in consistently interpreting myocardial morphology. To improve uniformity and model assessment, future research could focus on normalizing input contrast and employing ground truth comparisons. By reconstructing images from healthy subjects and contrasting them with multi-shot sequences, we could establish a reliable benchmark for model accuracy and reliability, a necessary step before applying it to clinical cardiac imaging [8].Conclusion
The diffusion model-based method introduced here is unique in cardiac MRI; it delivers enhanced image clarity for arrhythmia patients under real-time conditions, without domain-specific training. This technique not only boosts SNR and CNR metrics substantially but also simplifies the diagnostic process by potentially eliminating the need for complex segmentation models.Acknowledgements
No acknowledgement found.References
1.Winkelmann, S., Schaeffter, T., Koehler, T., Eggers, H., & Doessel, O. (2007). An optimal radial profile order based on the golden ratio for time-resolved MRI. IEEE Transactions on Medical Imaging, 26(1), 68–76. https://doi.org/10.1109/tmi.2006.885337
2. Lustig, M., Donoho, D., & Pauly, J. M. (2007). Sparse MRI: The application of compressed sensing for rapid MR Imaging. Magnetic Resonance in Medicine, 58(6), 1182–1195. https://doi.org/10.1002/mrm.21391
3. Wang, S., Su, Z., Ying, L., Peng, X., Zhu, S., Liang, F., Feng, D., & Liang, D. (2016). Accelerating magnetic resonance imaging via deep learning. 2016 IEEE 13th International Symposium on Biomedical Imaging (ISBI). https://doi.org/10.1109/isbi.2016.7493320
4. Bernard, O., et al (2018). Deep learning techniques for automatic MRI cardiac multi-structures segmentation and diagnosis: Is the problem solved? IEEE Transactions on Medical Imaging, 37(11), 2514–2525. https://doi.org/10.1109/tmi.2018.2837502
5. Song, Yang, et al (2020). "Score-based generative modeling through stochastic differential equations." arXiv preprint arXiv:2011.13456
6. Karras, Tero, et al (2022). "Elucidating the design space of diffusion-based generative models." Advances in Neural Information Processing Systems 35: 26565-26577.
7. Uecker, M., Ong, F., Tamir, J. I., et al. (2015). Berkeley advanced reconstruction toolbox. In Proceedings of the International Society for Magnetic Resonance in Medicine (Vol. 23, p. 2486). Toronto.
8. Luo, G., Blumenthal, M., Heide, M., & Uecker, M. (2023). Bayesian MRI reconstruction with joint uncertainty estimation using Diffusion Models. Magnetic Resonance in Medicine, 90(1), 295–311. https://doi.org/10.1002/mrm.29624
Figures