1741
Automatic rhythmic pressuring leading to instantly promotes drowsiness at RN12 site.1National Center for Nanoscience and Technology, Beijing, China, 2School of Future Technology, University of Chinese Academy of Sciences, Beijing, China, 3GE Healthcare, Beijing, China
Synopsis
Keywords: Psychiatric Disorders, Treatment, Non-pharmacological therapies; Sleep; Chinese Medicine
Motivation: This study is motivated by the increasing interest in non-pharmacological approaches, like RN12-ARP, to improve sleep quality and address sleep-related problems.
Goal(s): The specific aim is to investigate RN12-ARP's effects on sleepiness, EEG patterns, and brain activity in individuals with insomnia, exploring its potential as a solution for sleep disturbances.
Approach: Seventeen participants undergo RN12-ARP sessions, collecting EEG, sleep diaries, and psychological assessments, analyzed using high-density EEG and MRI.
Results: The study shows that RN12-ARP induces immediate sleepiness, supported by EEG-fMRI. Psychological scales have limited effects, but sleep diaries hint at improved sleep, suggesting potential for insomnia treatment, pending further research.
Impact: The study might pave the way for non-pharmacological interventions like RN12-ARP to address insomnia, improving the well-being of patients with sleep disturbances. Further investigations into the mechanisms behind quick drowsiness are pending, offering hope for alternative approaches to sleep therapy.
INTRODUCTION
Non-pharmaceutical interventions, such as traditional Chinese Medicine, have garnered attention for their role in enhancing the human body's self-healing abilities 1-4. This study delves into the enigmatic ZhongWan acupoint (RN12) and its potential to induce drowsiness through automatic rhythmic pressuring (RN12-ARP). Positioned at the intersection of abdominal fascia and superior rectus abdominis fascia 5, RN12-ARP alters muscle and fascia stretching forces, alongside weak stimulation and breathing actions. While it amplifies the sleepiness scale, the underlying mechanism remains unclear. This research strives to elucidate the connection between RN12-ARP and the autonomic nervous system, offering insights into non-pharmaceutical interventions' potential to address various health concerns and enhance well-being.METHODS
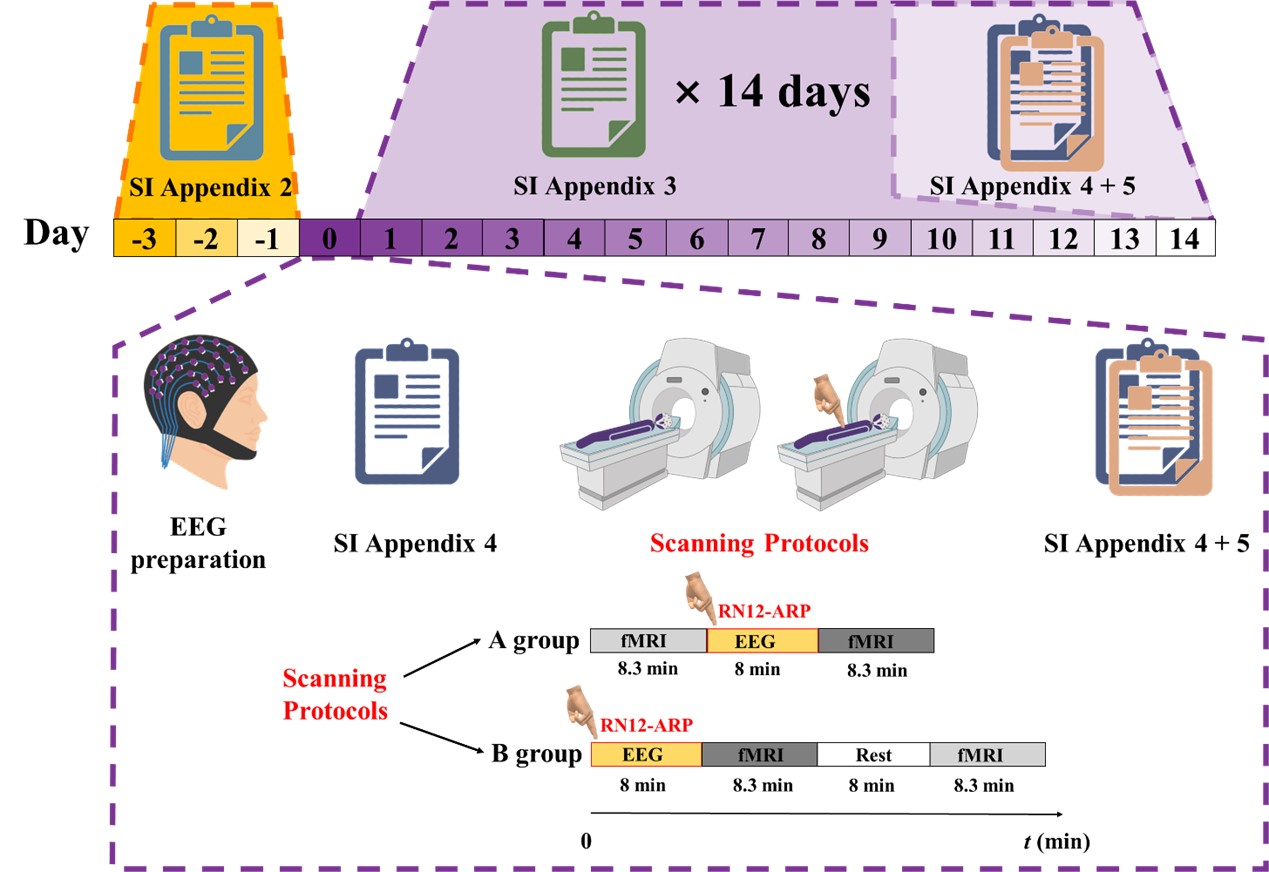
Seventeen healthy native Mandarin speakers from Beijing, aged 22-35, were recruited. Screening ensured they met specific criteria and had no history of insomnia or medical conditions like hypertension. They underwent RN12-ARP adaptation training and completed a 14-day sleep diary (see Figure 1 for experimental details). Participants were instructed to maintain regular sleep schedules and avoid staying up late. None were smokers or alcoholics. For three days before the scan, they recorded sleep data and daily habits. Participants completed ten psychological scales, including the Karolinska Scale 6, before and after compression. Sleep diary data was compared from the day of the intervention with data from two and seven days after the experiment. Parameters included time required to fall asleep, actual sleep time, sleep quality, and daytime alertness. Paired t-tests compared sleep quality and daytime alertness. High-density EEG data was collected using a custom MR-compatible electrode cap (NeuroScan, USA), maintaining stable electrode impedances. EEG signals were collected during RN12-ARP. Structural and functional MRI images were obtained using a 3T MRI scanner (GE Discovery MR750). EEG data were preprocessed, involving resampling, filtering, and removal of artifacts through Independent Component Analysis 7. EEG data were analyzed for power trends in five frequency bands. The fMRI data were preprocessed and analyzed for resting-state function indicators 8-11. The study employed network-based statistics to analyze functional connectivity and accounted for demographic covariates.RESULTS
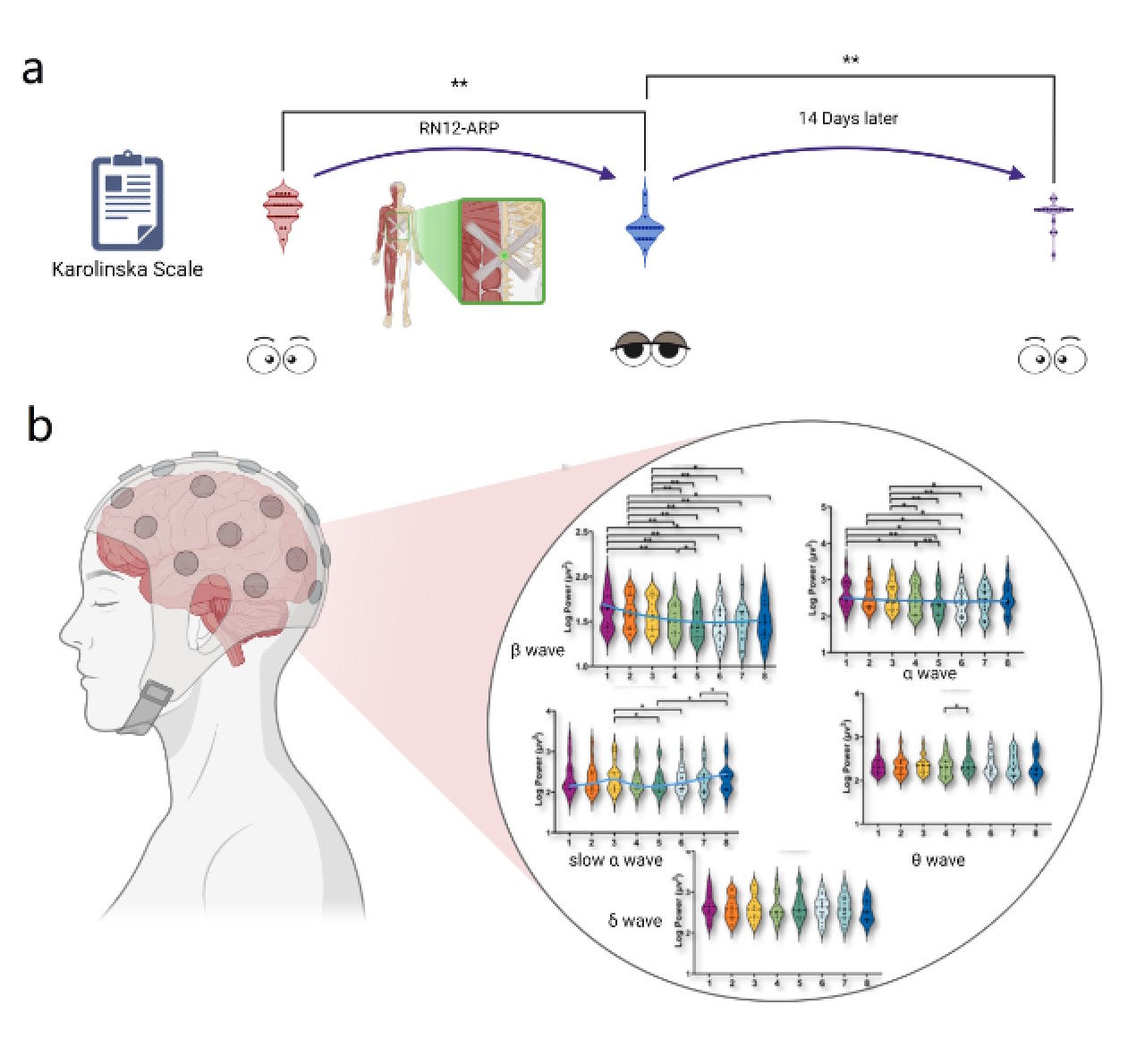
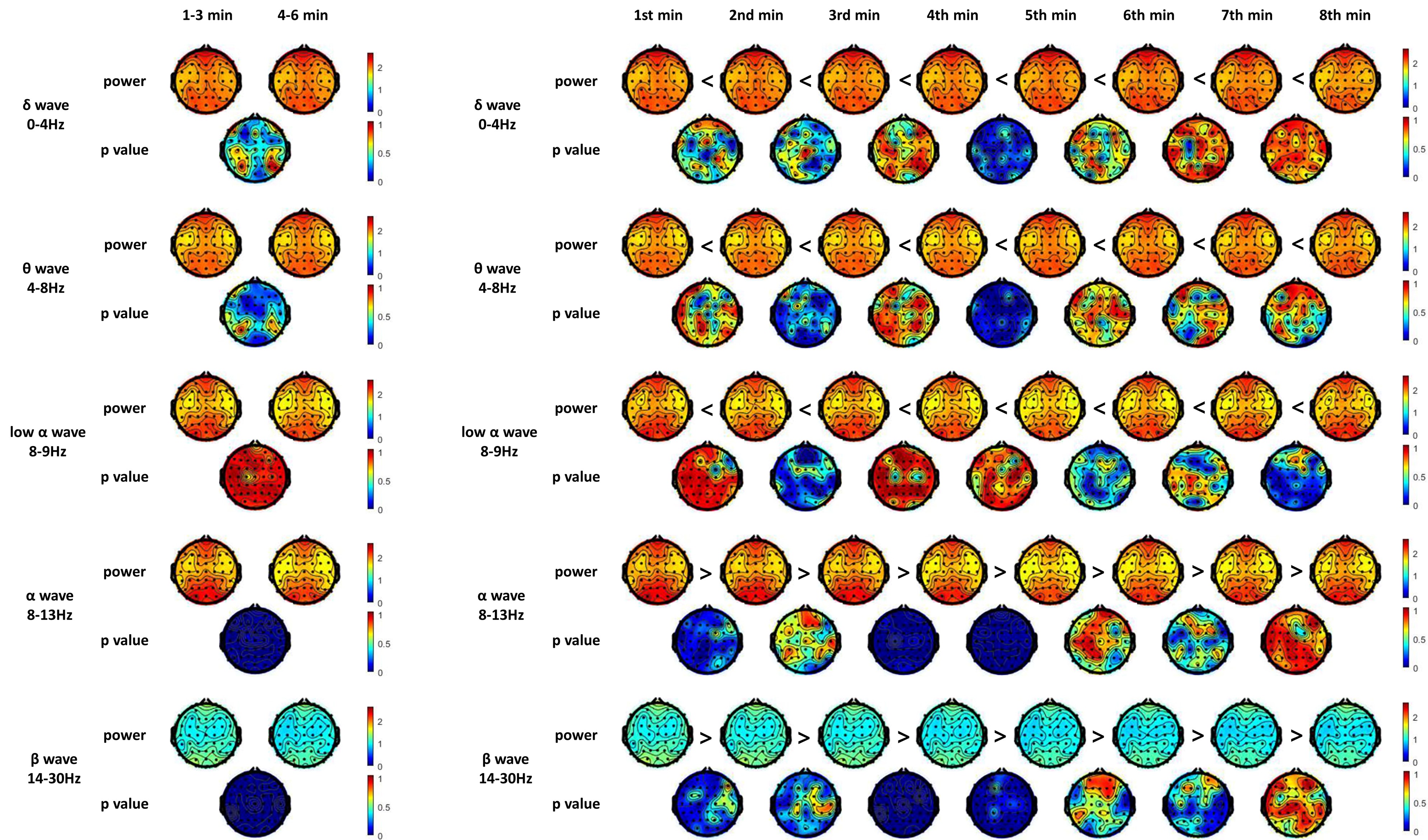
Subjective assessments, notably Karolinska scale scores 6, revealed an immediate increase in sleepiness post-RN12-ARP (Figure 2a), with this effect dissipating within 14 days. Objective evaluations using scales like the Pittsburgh Sleep Quality Index (PSQI) 12, Insomnia Severity Index (ISI) 13, and Epworth Sleepiness Scale (ESS) 14 demonstrated no significant changes post-treatment.Analysis of sleep diaries painted a different picture, indicating trends toward faster sleep onset, reduced total sleep duration, improved sleep quality, and daytime alertness. EEG data recorded during RN12-ARP sessions revealed altered brain activity patterns, with diminished beta and alpha wave activity suggesting a transition toward a more sedated state, while increasing low alpha and theta activity indicated heightened sleepiness (Figure 2b and Figure 3).
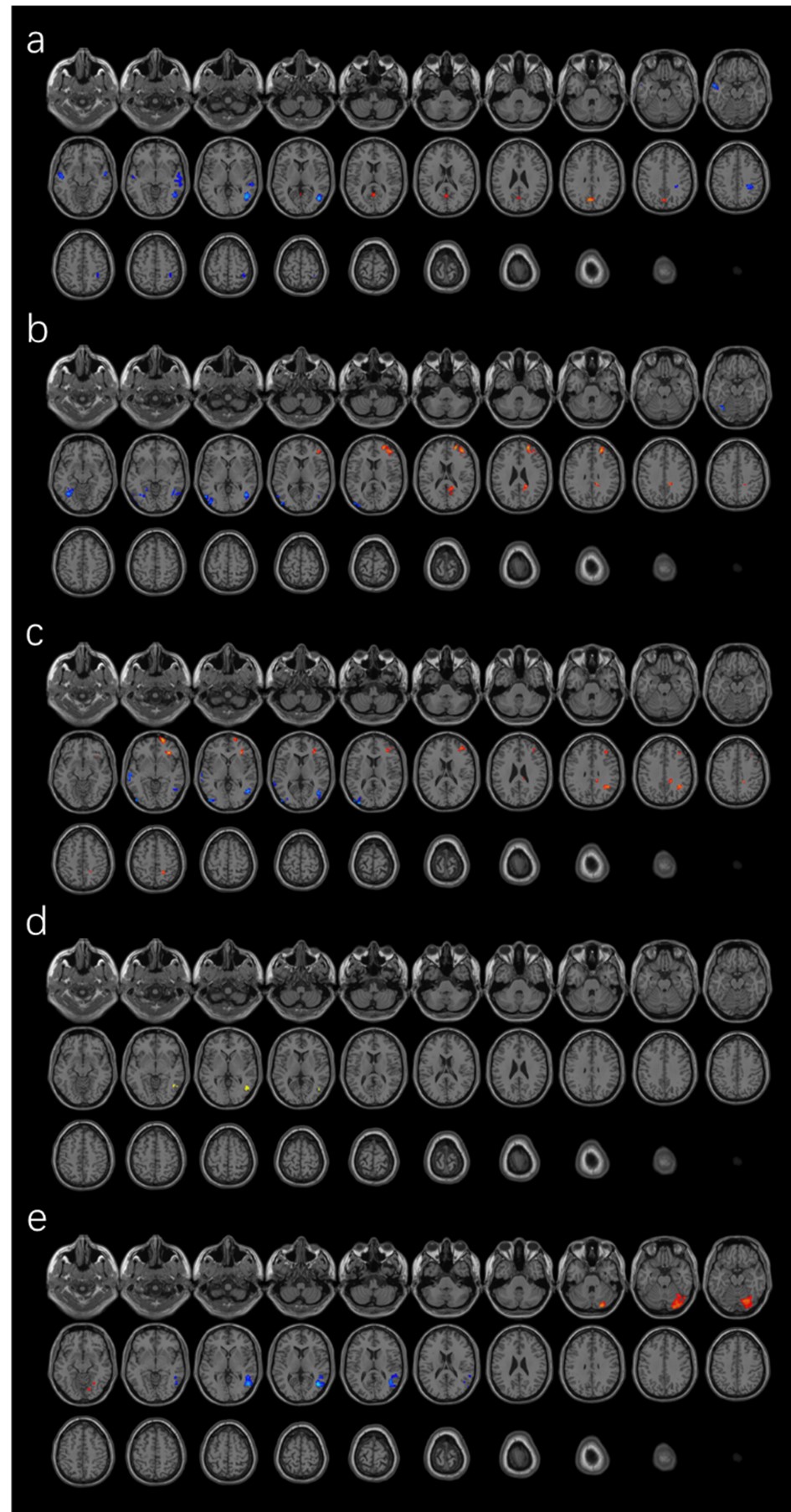
Resting-state fMRI results (Figure 4) showed significant differences post-RN12-ARP, primarily in areas like the middle frontal gyrus and Brodmann areas 9 and 10. Functional connectivity analysis demonstrated increased connectivity in the right middle temporal gyrus and inferior temporal gyrus, along with decreased connectivity in the right cerebellum. Analysis of brain network properties revealed reduced global efficiency and small-world characteristics, suggesting a decline in information integration and memory organization 15. Local brain regions displayed varying changes in efficiency, reflecting different sleepiness states.
DISCUSSION & CONCLUSION
This study illuminates the effects of RN12-ARP on brain activity and sleep-related parameters. The immediate increase in subjective sleepiness post-RN12-ARP aligns with observed EEG changes, including reduced beta and alpha waves, alongside heightened low alpha and theta wave activity. This objective shift reinforces participants' reported sleepiness. Psychological scales showed no significant post-RN12-ARP changes, suggesting they may not capture immediate effects adequately. Conversely, sleep diaries indicated trends toward quicker sleep onset, enhanced quality, and increased daytime alertness, hinting at RN12-ARP's cumulative and prolonged effects. These findings imply that RN12-ARP can induce sleepiness and may hold promise for addressing insomnia, but further research is needed to explore mechanisms and potential implications for non-pharmacological insomnia interventions. In conclusion, this study offers valuable insights into RN12-ARP as a non-pharmacological intervention for sleep issues, especially in insomnia cases. This approach may hold promise in clinical practice to address sleep disturbances, but the transient nature of increased sleepiness post-RN12-ARP raises questions about the intervention's duration. Further research is crucial to understand underlying mechanisms and assess RN12-ARP's sustained impact on sleep quality and related parameters. RN12-ARP's ability to influence brain activity and induce sleepiness presents potential for addressing insomnia and related sleep disturbances. However, comprehensive comprehension and evaluation of its mechanisms and long-term clinical effectiveness necessitate further investigation.Acknowledgements
Thiswork was supported by National Natural Science Foundation of China(NO.61971151).References
1. Puledda, F. & Shields, K. Non-pharmacological approaches for migraine. Neurotherapeutics 15, 336-345 (2018).
2. Qian, X. et al. Assessment of the efficacy of tuina on treating cervicogenic headache: A protocol for systematic review and meta-analysis. Medicine 100 (2021).
3. Liu, Z. et al. A review on the mechanism of Tuina promoting the recovery of peripheral nerve injury. Evid Based Complement Alternat Med 2021, 6652099(2021).
4. Liu, S. et al. A neuroanatomical basis for electroacupuncture to drive the vagal–adrenal axis. Nature 598, 641-645 (2021).
5. Myers, T. W. Anatomy Trains: Myofascial Meridians for Manual Therapists and Movement Professionals, Chapter 6. 4 edition, (Elsevier, 2020).
6. Åkerstedt, T. & Gillberg, M. Subjective and objective sleepiness in the active individual. International journal of neuroscience 52, 29-37 (1990).
7. Delorme, A. & Makeig, S. EEGLAB: an open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. Journal of neuroscience methods 134, 9-21 (2004).
8. Giavasis, S. et al. The Configurable Pipeline for the Analysis of Connectomes (C-PAC) 2020-21: Transitioning Out of Beta.
9. Zou, Q.-H. et al. An improved approach to detection of amplitude of low-frequency fluctuation (ALFF) for resting-state fMRI: fractional ALFF. Journal of neuroscience methods 172, 137-141 (2008).
10. Zang, Y., Jiang, T., Lu, Y., He, Y. & Tian, L. Regional homogeneity approach to fMRI data analysis. Neuroimage 22, 394-400 (2004).
11. Hoptman, M. J. et al. Amplitude of low-frequency oscillations in schizophrenia: a resting state fMRI study. Schizophrenia research 117, 13-20 (2010).
12. Buysse, D. J., Reynolds III, C. F., Monk, T. H., Berman, S. R. & Kupfer, D. J. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res 28, 193-213 (1989).
13. Xie, D. et al. Functional connectivity abnormalities of brain regions with structural deficits in primary insomnia patients. Front Neurosci 14, 566 (2020).
14. Johns, M. W. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep 14, 540-545 (1991).
15. Liang, X., Wang, J. & He, Y. Human connectome: structural and functional brain networks. Chinese Science Bulletin 55, 1565-1583 (2010).
Figures