1735
Disentangling disease-specific and trauma-related alterations of regional cortical intrinsic activity in post-traumatic stress disorder1Department of Radiology and Huaxi MR Research Center (HMRRC), Functional and Molecular lmaging Key Laboratory of Sichuan Province, West China Hospital, Sichuan University, Chengdu, China, 2Institute of psychoradiology,West China Xiamen Hospital of Sichuan University, Xiamen, China
Synopsis
Keywords: Psychiatric Disorders, Psychiatric Disorders
Motivation: Trauma can lead to plastic alterations to regional cortical intrinsic activity, and dysregulation in a normal adaption to stress could contribute to PTSD. However, few previous studies disentangled trauma-related adaptation and maladaptation related to PTSD in regional cortical intrinsic activity.
Goal(s): To disentangle trauma-related and PTSD-related abnormalities in regional cortical intrinsic activity.
Approach: We compared the (fraction) amplitude of low frequency fluctuations and regional homogeneity among PTSD patients, traumatized and non-traumatized subjects.
Results: In all trauma-related results, we found decreased (f)ALFF in the bilateral cerebellum, inferior temporal gyrus and middle occipital gyrus was also PTSD-related.
Impact: We disentangled the distinction between trauma-related and PTSD specific alteration as measured by regional cortical intrinsic activity. It suggested trauma may cause decreased (f)ALFF in cerebellum, however, severe dysfunction exceeding individul’ capabilities to cope with stress may lead to PTSD.
Introduction
Posttraumatic Stress Disorder (PTSD) is associated with several symptoms, including intrusive memories, hyperarousal and active fight or flight defensive responses. Trauma exposure, a direct trigger of PTSD, has been linked to development of PTSD, impairing patients’ learning and memory functions [1]. Interestingly, 5-10% of the trauma-exposed population could occur PTSD [2-3], hence it is important to know the distinction between trauma-related brain alteration and PTSD specific alteration. A previous study has reported that compared with TCs, PTSD patients exhibited increased intrinsic activity (ALFF and ReHo) in the left inferior parietal lobule (IPL) and decreased in the right lingual gyrus [4]. However, it hasn’t tease apart these trauma-specific effects would be hugely relevant., furthermore, in this study, it was significant heterogeneity in the types of traumas that PTSD patients were exposed to and kept mismatching of gender. However, pathophysiologic characteristics of PTSD patients and TCs with the altered different regional cortical intrinsic activity and disentanglement of PTSD specific and trauma-related alterations remains poorly understood, although it is critical for the development of treatment strategies and classification for this population and thus for improving patient care and preventing relapse.Methods
A total of 47 PTSD patients, 64 trauma-exposed controls are included in this study finally. 46 age- and sex-match healthy control (HC) subjects who never experienced earthquake. All of PTSD patients and TCs were medicine-free and underwent trauma exposure firsthand. All participants were diagnosed following the clinician-administered PTSD Scale (CAPS) in diagnostic and fourth edition (DSM-IV). Resting-state functional MRI images were acquired using a 3.0 T MRI system and an eight-channel phase array head coil. We used the Data Processing Assistant for Resting-State fMRI (DPARSF, http://www.restfmri.net, version 5.3), implemented within the MATLAB toolbox for functional and anatomical data preprocessing to sequently acquire individual maps of regional cortical intrinsic activity parameters, including ALFF, fALFF and ReHo. Further group-level ANOVA and post hoc analysis of difference of functional connectivity among PTSD, TC and HC groups were conducted via SPM12 software (https://www.fil.ion.ucl.ac.uk/spm/software/spm12/). The significance threshold was set as P < 0.001 (uncorrected) at the voxel level and a family-wise error (FWE) corrected P < 0.05. Then we extracted neural function values of regions to performed post hoc analysis via SPSS software (IBM SPSS Statistics for Windows, version 19.0) (P<0.05).Results
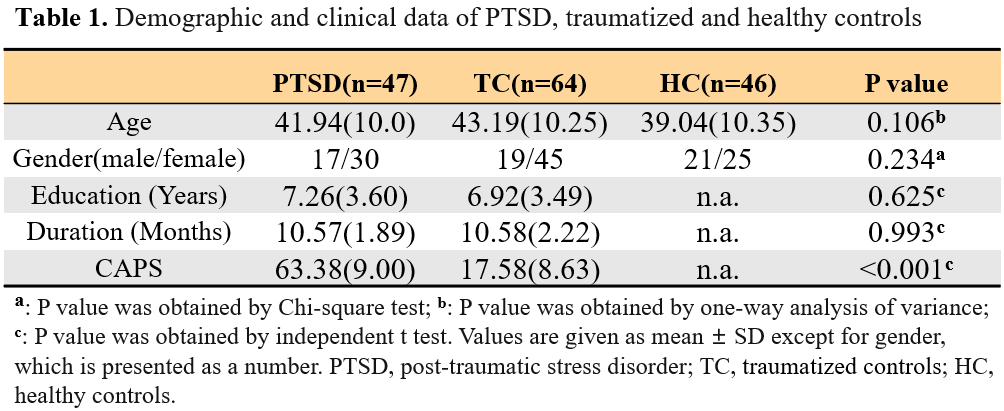
Demographic and clinical characteristicsThe demographic information and clinical characteristics of the subjects are shown in Table 1.
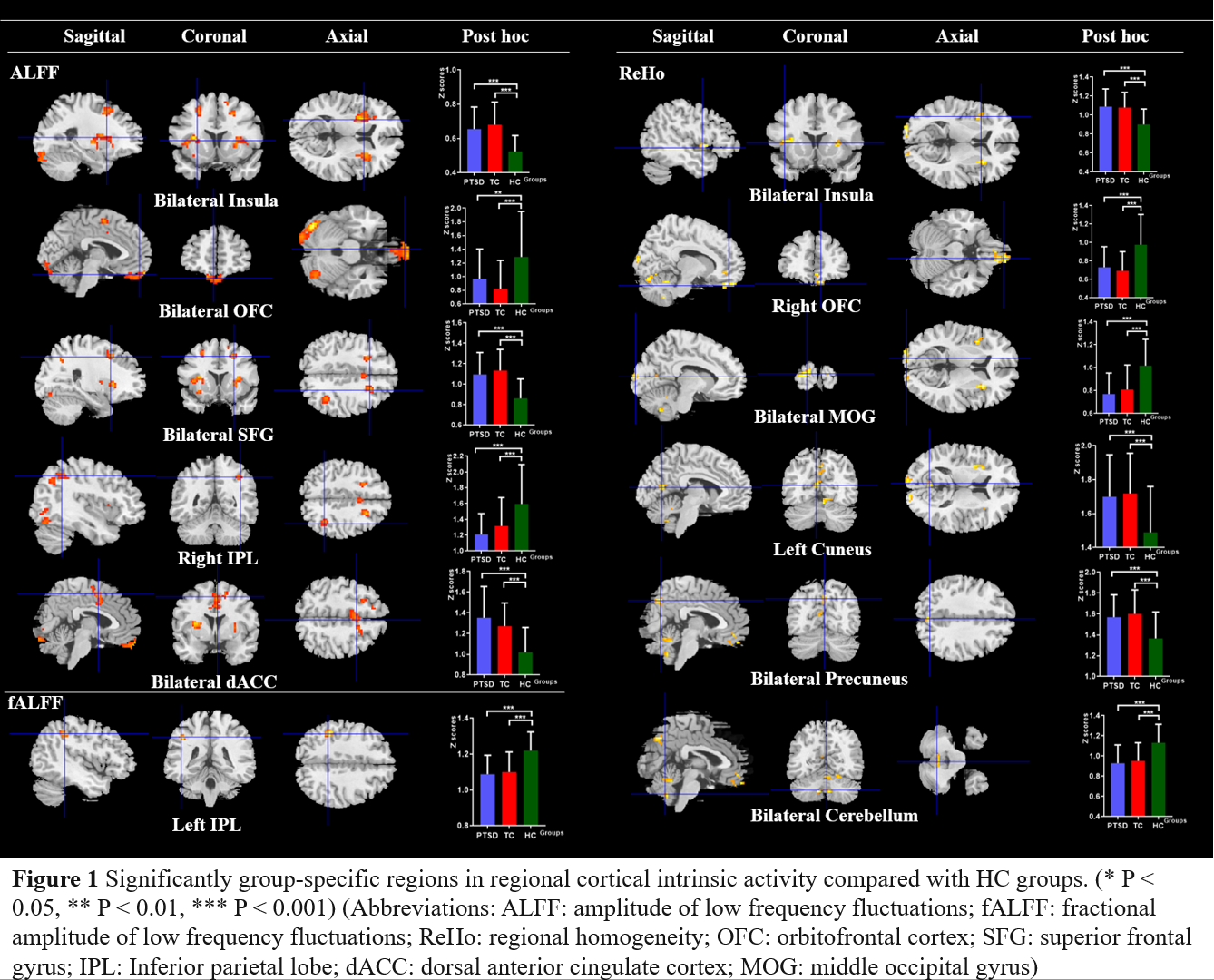
Trauma-related alterations
Compared with the HCs, both PTSD patients and TCs had significantly higher ALFF in the bilateral insula, superior frontal gyrus (SFG) and dorsal anterior cingulate cortex (dACC) but lower ALFF in the bilateral cerebellum, OFC, inferior temporal gyrus (ITG) and right IPL. In the fALFF analysis, both PTSD patients and TCs exhibited significantly lower fALFF in bilateral cerebellum, middle occipital gyrus (MOG), left IPL, insula, putamen and right cuneus when compared with HCs. In the ReHo analysis, both PTSD and TC groups showed enhanced ReHo in the left cuneus, bilateral insula and precuneus but significantly decreased ReHo in the bilateral MOG, cerebellum and right OFC when compared to HCs (Figure 1).
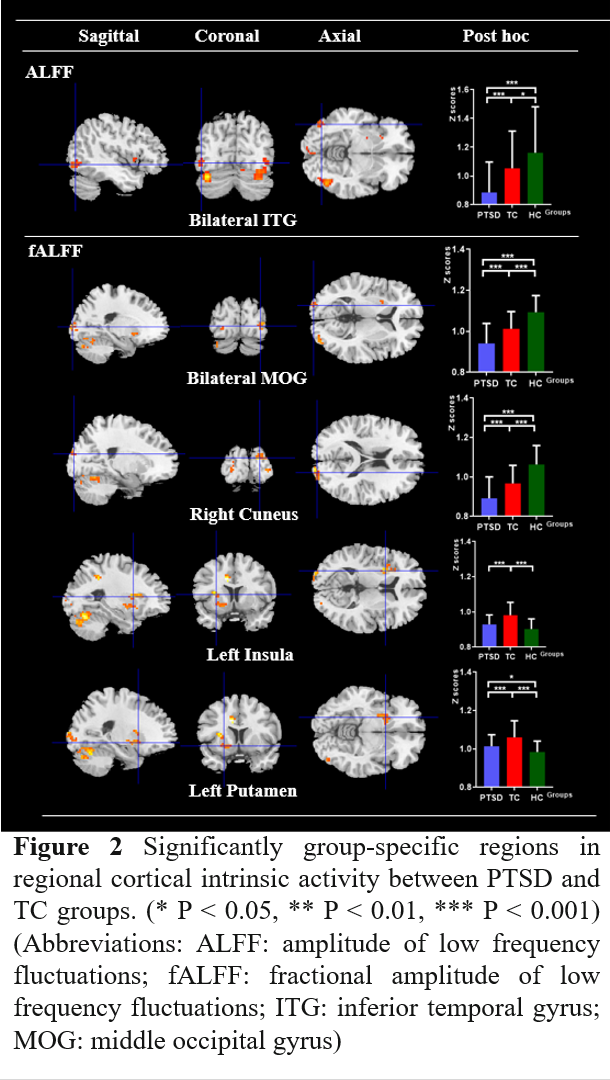
PTSD-related alterations
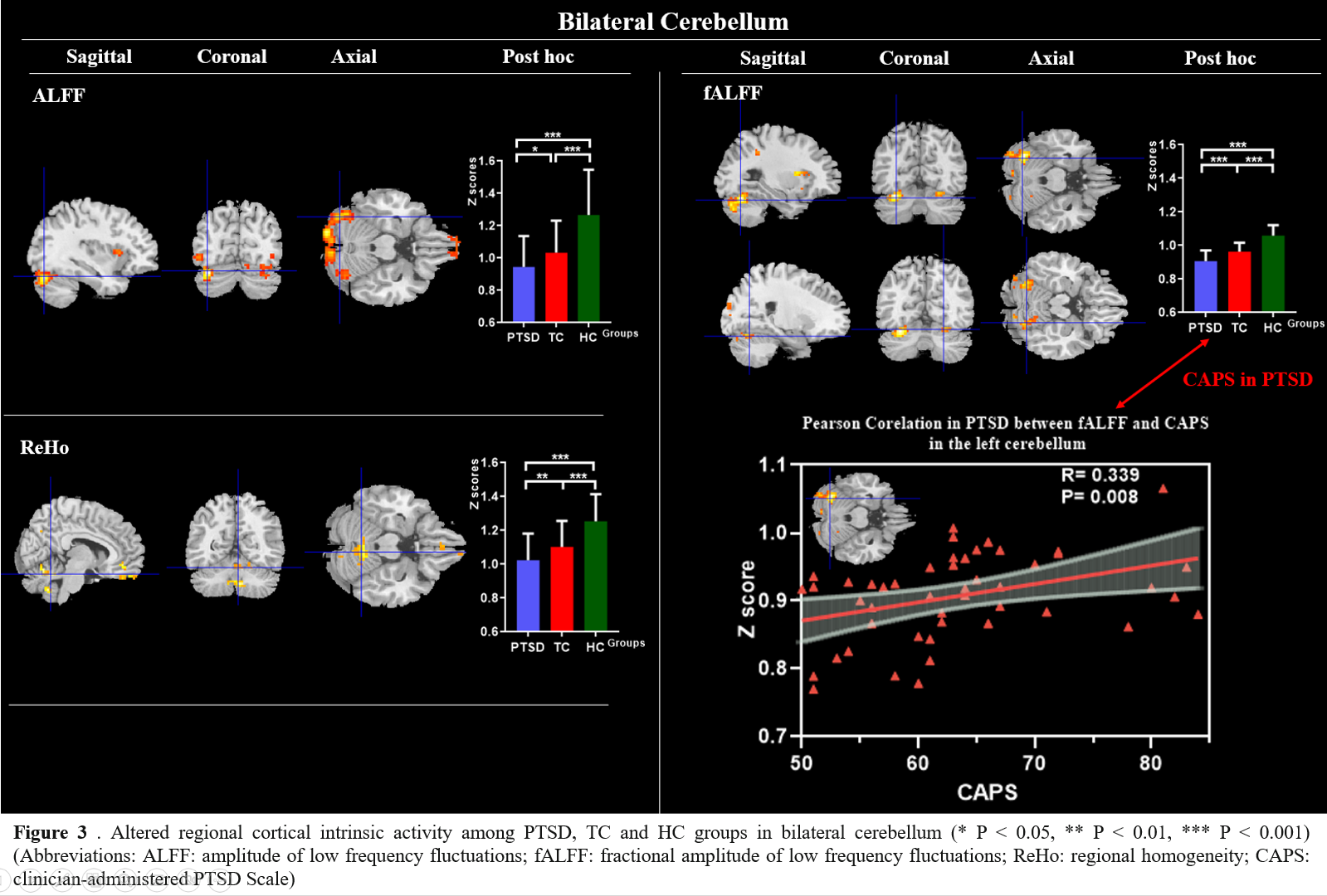
In the aforementioned alterations, we found that PTSD patients showed significantly decreased (f)ALFF in the, bilateral cerebellum, ITG, MOG, and right cuneus (Figure 2). Moreover, significantly decreased ReHo was also identified in the bilateral cerebellum. We found the positive correlation between fALFF values of PTSD in the left cerebellum and CAPS scores (Figure 3).
Discussion & Conclusion
We demonstrated that abnormal regional cortical intrinsic activities of most distinguished regions were more likely associated with the same trauma. Trauma may cause decreased (f)ALFF in cerebellum and visual network, however, severe dysfunction in this region that exceed individual’ capabilities to cope with stress may lead to PTSD. Secondly, severity of PTSD symptoms measured with CAPS scores correlated with fALFF in left cerebellum. Overall, these results may help us understand the neurobiological mechanism, improving preventive strategies for the trauma-exposed population and providing evidence to develop clinical practice based on altered regional cortical intrinsic activity.Acknowledgements
This study was supported by National Key R&D Program of China (Grant No. 2022YFF1202400).References
[1] Samuelson, K.W., Krueger, C.E., Burnett, C., Wilson, C.K., 2010. Neuropsychological functioning in children with posttraumatic stress disorder. Child Neuropsychol. 16,119–133.
[2] Koch, S.B., van Zuiden, M., Nawijn, L., Frijling, J.L., Veltman, D.J., Olff, M., 2016. Aberrant resting-state brain activity in posttraumatic stress disorder: a meta-analysis and systematic review. Depress. Anxiety 33, 592–605.
[3] Koenen, K., Ratanatharathorn, A., Ng, L., McLaughlin, K., Bromet, E., Stein, D., . . . Kessler, R. (2017). Posttraumatic stress disorder in the World Mental Health Surveys. Psychological Medicine, 47(13), 2260-2274.
[4] Disner SG, Marquardt CA, Mueller BA, Burton PC, Sponheim SR. Spontaneous neural activity differences in posttraumatic stress disorder: A quantitative resting-state meta-analysis and fMRI validation. Hum Brain Mapp. 2018 Feb;39(2):837-850. doi: 10.1002/hbm.23886. Epub 2017 Nov 15. PMID: 29143411; PMCID: PMC6866285.
Figures