1732
Stimulant medication and development of the dopamine system in ADHD: a pharmacological MRI study1Dept. of Radiology & Nuclear Medicine, Amsterdam UMC location University of Amsterdam, Amsterdam, Netherlands, 2Dept. of Radiology & Nuclear Medicine, Amsterdam UMC location Vrije Universiteit Amsterdam, Amsterdam, Netherlands, 3CIBM, Center for Biomedical Imaging, Ecole Polytechnique Fédérale de Lausanne (EPFL), Lausanne, Switzerland, 4Accare, Centre for Academic Child and Adolescent Psychiatry, UMC Groningen, Groningen, Netherlands, 5Dutch Autism and ADHD Research Center, Amsterdam Brain and Cognition, University of Amsterdam, Amsterdam, Netherlands
Synopsis
Keywords: Psychiatric Disorders, Neuroscience
Motivation: The effects of stimulant treatment (e.g. methylphenidate) on the brain’s dopamine system remain unclear. While animal studies and short-term human trials suggest potential lasting impacts, a comprehensive understanding is lacking.
Goal(s): This study aimed to investigate the persistent effects of stimulant treatment on the dopamine system.
Approach: Using data from a naturalistic follow-up of an ADHD trial, we examined the cerebral blood flow (CBF) response to methylphenidate as a proxy for dopamine function.
Results: Our findings reveal age-dependent effects. Specifically, we observed a negative association between medication use and CBF response in adolescents, while such an association was absent in adults.
Impact: We found an association between patterns of stimulant treatment for ADHD and the cerebral blood flow response to a dopamine-challenge in adolescents, but not adults. This suggests potential for personalization of stimulant treatment approaches for adolescents with ADHD.
Introduction
Stimulant medication, such as methylphenidate (MPH) and dexamphetamine, is commonly prescribed to children and adolescents with ADHD for extended periods of time. Yet, the effects on the development of the brain’s dopamine (DA) system remain unclear.Animal studies have suggested that MPH administration during development may have long-term effects on brain development, which are fully expressed close to adulthood (“the neurochemical imprinting hypothesis”).1,2 Indeed, in a randomized controlled trial (RCT), we previously showed that 4-month treatment with MPH, compared to placebo, decreased the cerebral blood flow (CBF) response to an acute challenge with MPH after one-week washout in stimulant treatment-naive children, but not adults, with ADHD.3 This suggests age-dependent persistent effects of MPH-treatment on the short-term. To investigate whether these effects are long-lasting, we here present the results from a 4-5 year naturalistic follow-up of the initial RCT participants. We hypothesized that higher stimulant medication use during this naturalistic follow-up would be associated with less CBF-response in adolescents, but not adults, meaning that age-dependent MPH effects on the dopamine system would be long-lasting.
Methods
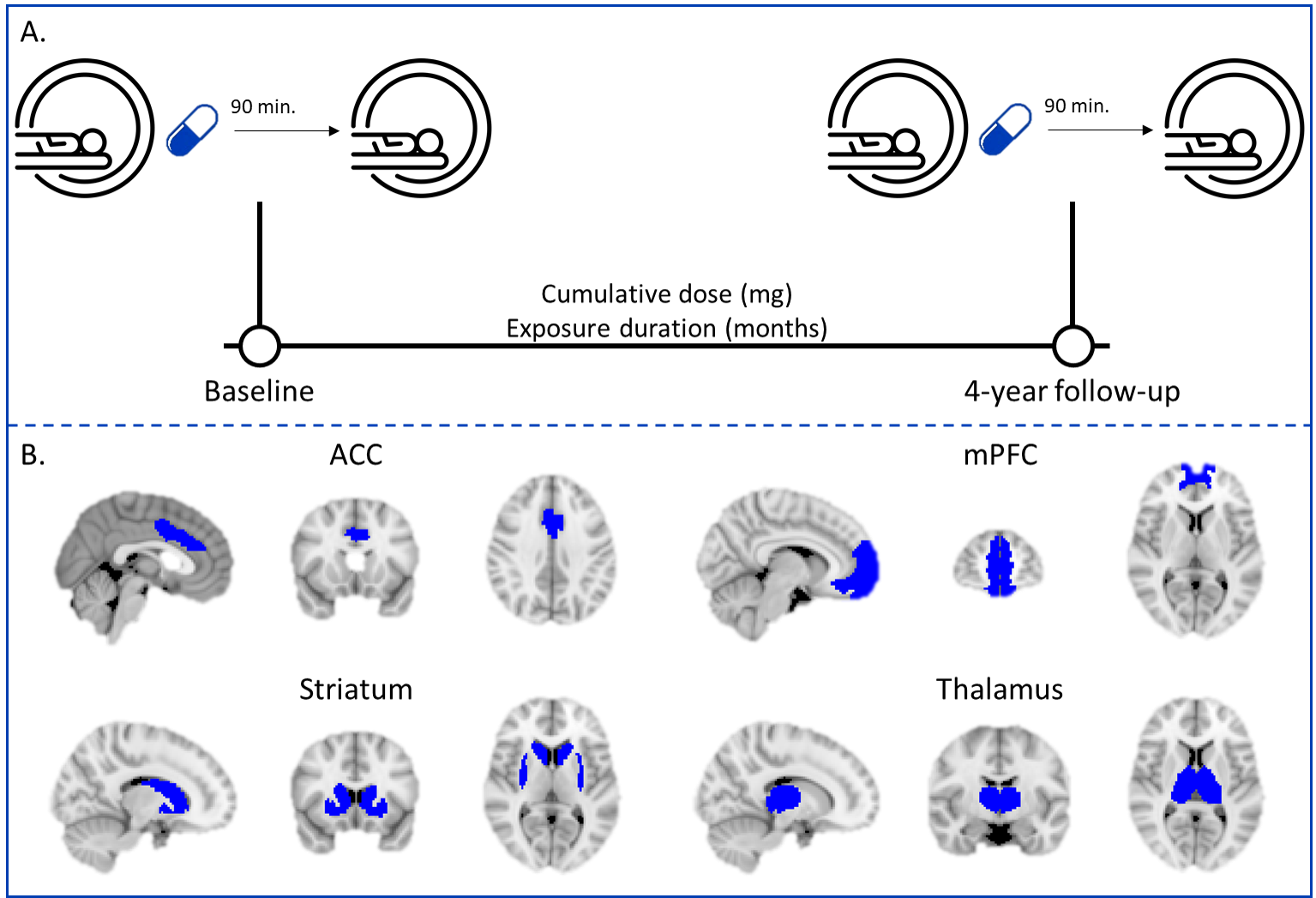
In the initial RCT3, 50 boys (mean age=11.4±0.8yrs) and 49 men (mean age=28.6±4.6yrs) with ADHD were included. All participants were stimulant treatment-naïve at baseline and met strict criteria for ADHD diagnosis (all subtypes) according to the DSM-IV criteria4. From the initial RCT, 33 adolescent and 25 adult participants returned for the 4-year follow-up assessment.At baseline and 4-year follow-up, MR scanning was performed using 3T Philips MR scanners (Intera/Achieva/Ingenia) with an 8-channel receive-only head coil. To assess dopamine function, a 2D gradient-echo echo-planar imaging pseudo-continuous arterial spin labelling (pCASL) sequence (TR/TE=4000/14ms; post-label delay=1525ms; label duration=1650ms; FOV=240x240x119mm; 75 dynamics; voxel size=3x3x7mm; no background suppression) was acquired before (pre-MPH) and 90 minutes after (post-MPH) a single-dose short-acting MPH-challenge (0.5mg/kg; max. 20mg for adolescents, max. 40mg for adults; Figure 1A). Additionally, we acquired a 3D T1-weighted fast-field echo sequence (TR/TE=9.8/4.6ms; FOV=256x256x120mm; voxel size=0.875x0.875x1.2mm) for registration purposes.
ASL post-processing was performed using the ExploreASL pipeline (v1.11.0Beta5) in Matlab (R2022b). A fixed spike removal threshold (1mm) was used for motion outlier exclusion. Median CBF (mL/min/100g) was estimated for total gray matter (GM) and four predefined regions of interest (ROIs): anterior cingulate cortex (ACC), medial prefrontal cortex (mPFC), striatum and thalamus (Figure 1B). For analysis, CBF was calculated for each ROI relative to total GM, since total GM CBF may experience large physiological and vascular variability across development and a MPH-challenge, respectively. The relative CBF (rCBF)-response was calculated as (post-MPH - pre-MPH)/pre-MPH, taking into account each individuals’ pre-MPH rCBF.
Stimulant medication use per participant was calculated based on medication received during the RCT (titrated per individual according to Dutch clinical treatment guidelines) and medication history information between the RCT and 4-year follow-up obtained from pharmacies. Cumulative dose (mg) of stimulant medication was converted to MPH-equivalents as previously described.6,7 In addition, exposure duration (months) to stimulant medication was calculated.
Statistical analysis was performed in R (v4.0.3). The main and interaction effects of medication use (cumulative dose/exposure duration), age group (adolescents/adults), and visit (baseline/follow-up) on rCBF-response to a MPH-challenge were assessed using three-way linear mixed effects models. Motion (mm), MR scanner at baseline (Intera/Achieva), baseline age (yrs), and scan interval (months) were included as covariates in all models. All analyses were corrected for multiple comparisons (FDR=5%).
Results
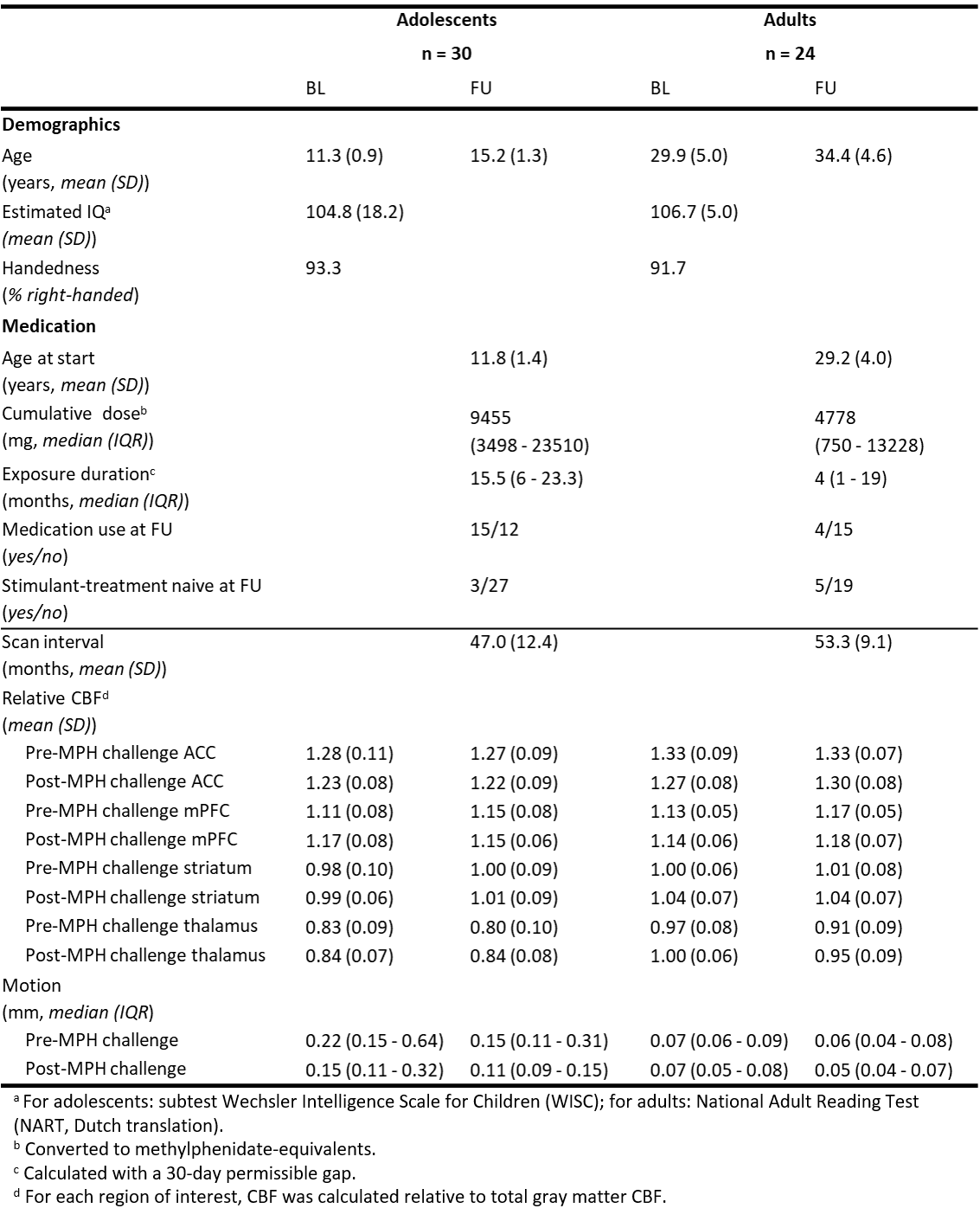
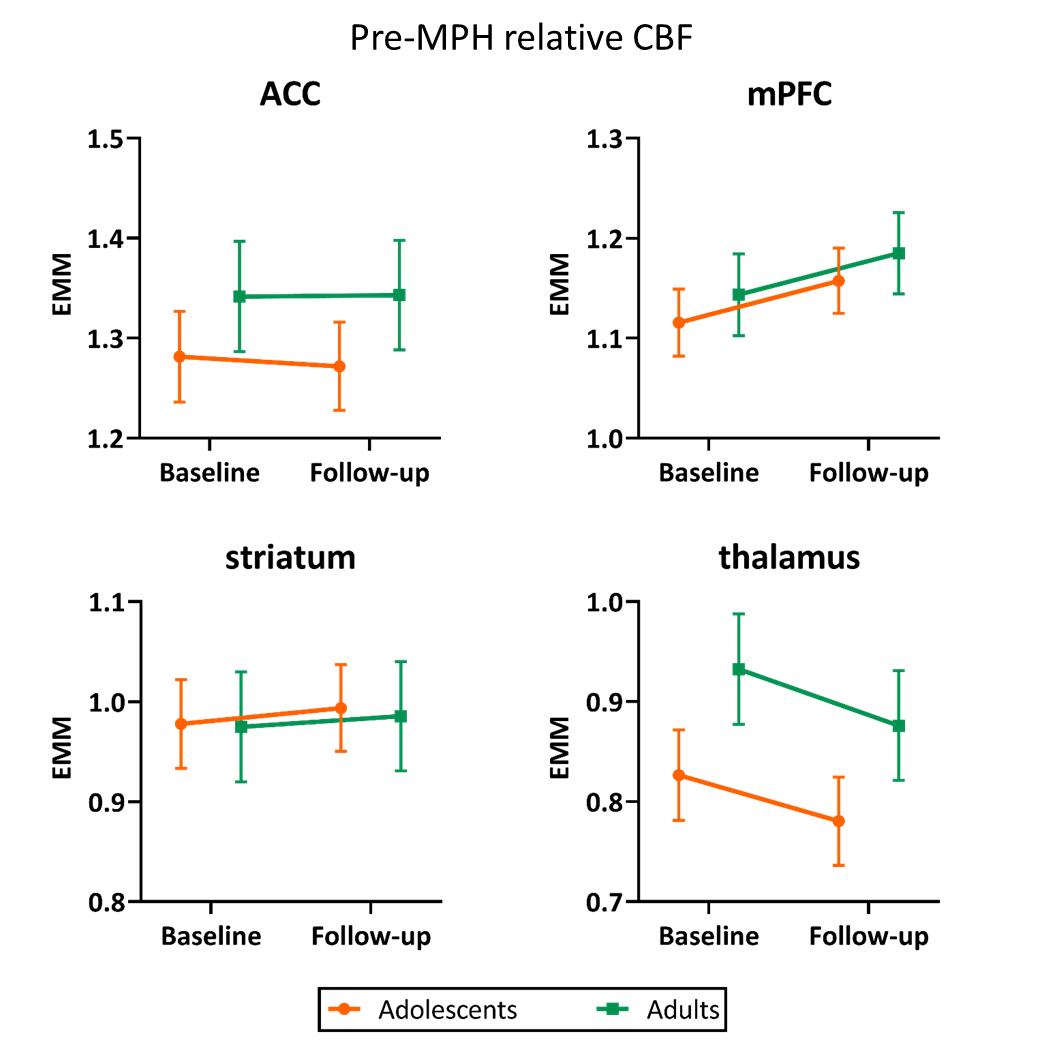
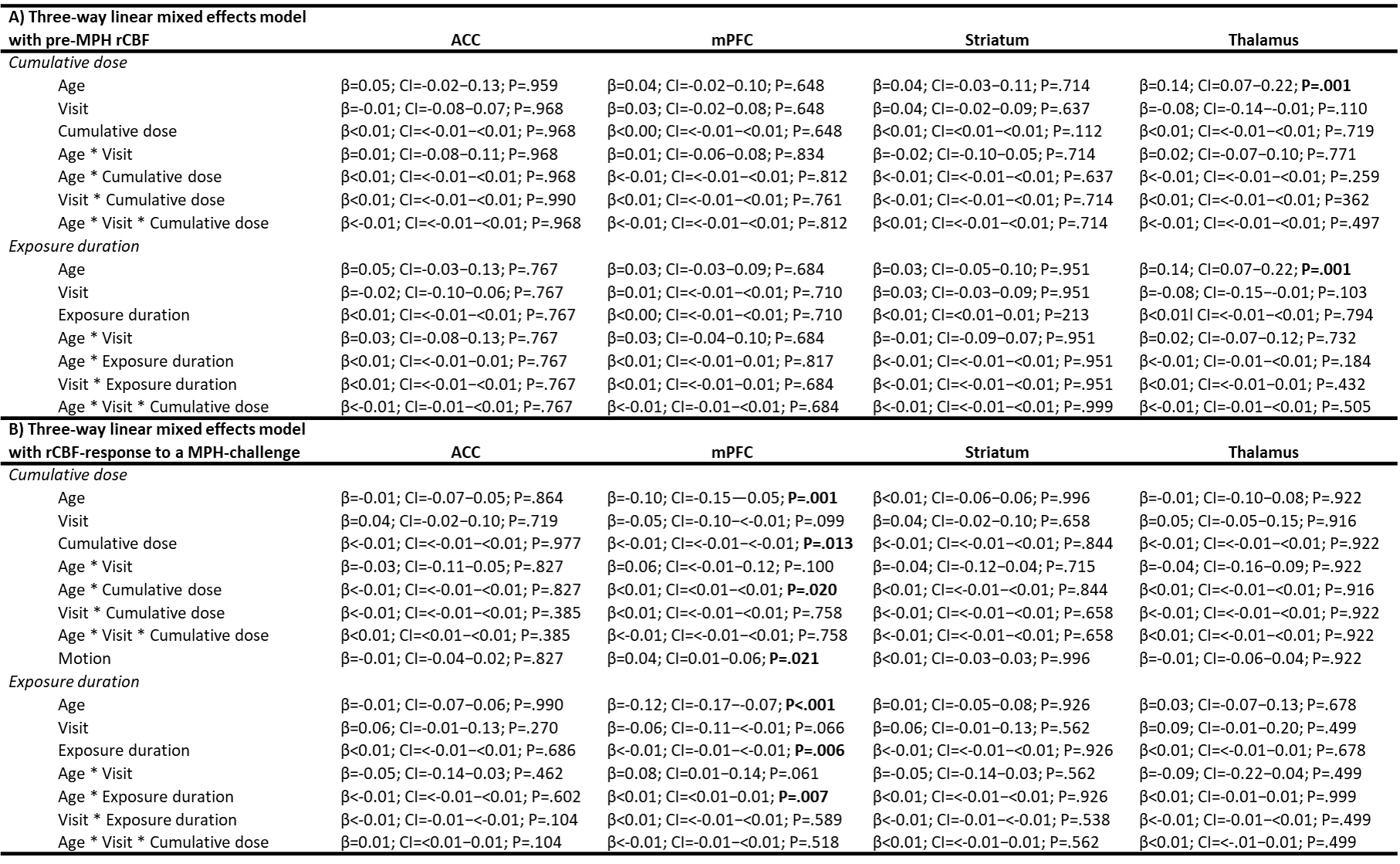
From the participants that returned for the follow-up assessment, 3 participants (2 adolescents, 1 adult) were excluded from analysis due to incomplete data or undisclosed stimulant medication use before baseline assessment, resulting in a final sample of 30 adolescents and 24 adults (Table 1).rCBF pre-MPH: We found no age-by-medication-by-visit interaction effect on pre-MPH rCBF (Table 2A; Figure 2). We did observe a main effect of age group on thalamic rCBF (p=.001), with adults showing higher pre-MPH rCBF than adolescents (independent of visit).
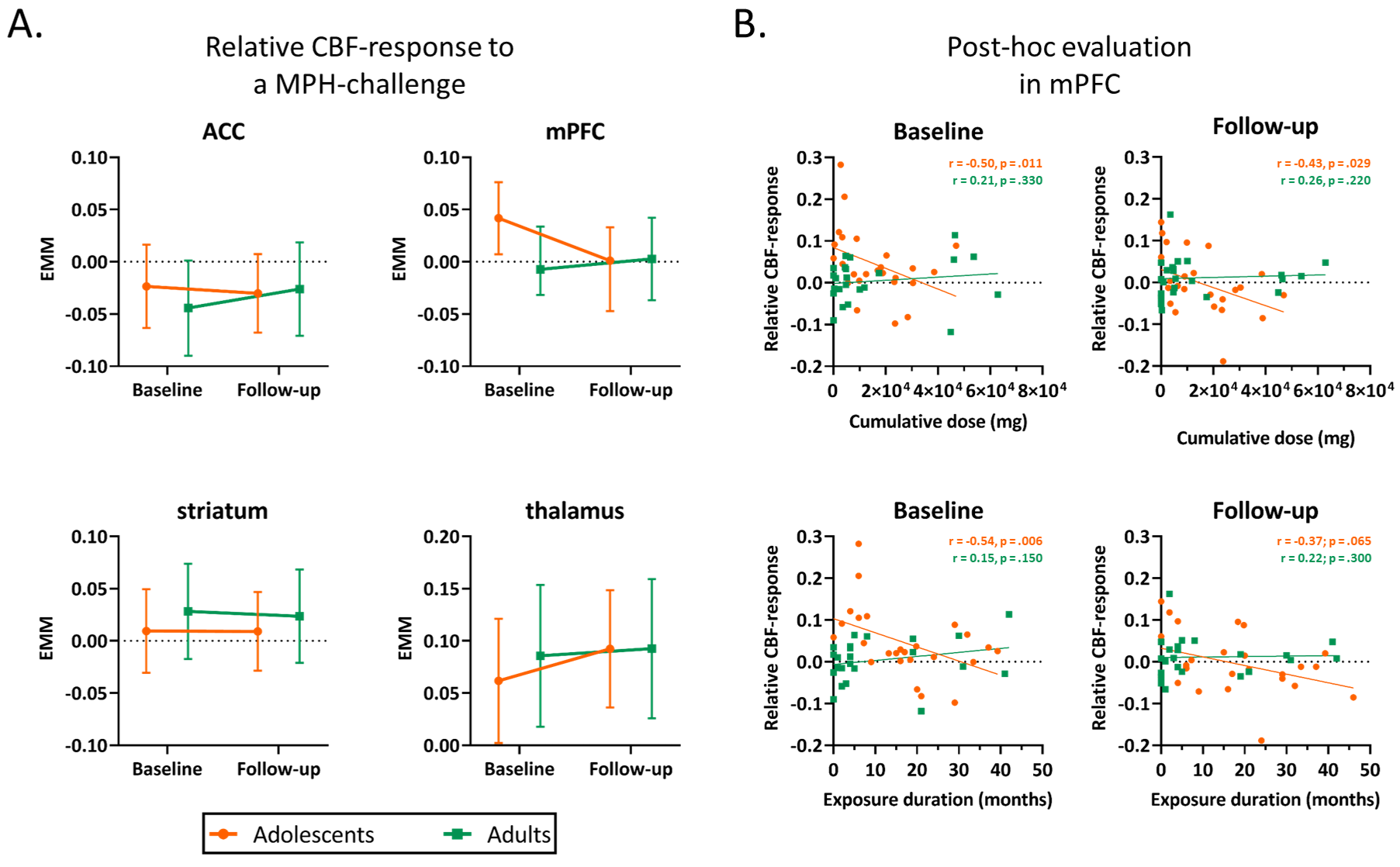
rCBF-response: We found no age-by-medication-by-visit interaction effect on rCBF-response in adolescents or adults. We did, however, identify an age-by-medication interaction effect in the mPFC (cumulative dose: p=.020; exposure duration: p=.007; Table 2B, Figure 3A). Post-hoc analysis revealed a negative association between medication use and rCBF-response in adolescents only (Figure 3B).
Discussion
In line with the neurochemical imprinting hypothesis1,2 and our short-term findings from the initial RCT3, we found that stimulant medication use during development was associated with estimates of DA-functioning of the mPFC. Individuals that needed more medication during the 4-5 year naturalistic follow-up showed less rCBF-response to an acute challenge with MPH, suggesting potential for personalization of stimulant treatment approaches. Future studies will investigate this further and relate DA-functioning to ADHD symptom severity and other clinical outcomes.Acknowledgements
This study was funded by the Dutch non-profit organizations KiddyGoodPills and Suffigium. The RCT (baseline data) was funded by a personal research grant awarded to LR by the Academic Medical Center, University of Amsterdam, and 11.32050.26ERA-NET PRIOMEDCHILD FP 6 (EU). We would like to thank all participants and their parents for their contribution to this study and all students that helped with collection and analysis of the data.References
1. Andersen SL. Trajectories of brain development: point of vulnerability or window of opportunity? Neurosci Biobehav Rev. 2003;27(1-2):3–18. DOI: 10.1016/s0149-7634(03)00005-8.
2. Urban KR, Waterhouse BD, Gao WJ. Distinct age-dependent effects of methylphenidate on developing and adult prefrontal neurons. Biol Psychiatry. 2012 Nov 15;72(10):880–8. DOI: 10.1016/j.biopsych.2012.04.018.
3. Schrantee, A., Tamminga, H. G., Bouziane, C., Bottelier, M. A., Bron, E. E., Mutsaerts, H. J., Zwinderman, A. H., Groote, I. R., Rombouts, S. A., Lindauer, R. J., Klein, S., Niessen, W. J., Opmeer, B. C., Boer, F., Lucassen, P. J., Andersen, S. L., Geurts, H. M., & Reneman, L. (2016). Age-Dependent Effects of Methylphenidate on the Human Dopaminergic System in Young vs Adult Patients With Attention-Deficit/Hyperactivity Disorder: A Randomized Clinical Trial. JAMA psychiatry, 73(9), 955–962. https://doi.org/10.1001/jamapsychiatry.2016.1572
4. American Psychiatric Association, American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-IV. Vol. 4. Washington, DC: American psychiatric association; 1994.
5. Mutsaerts HJMM, Petr J, Groot P, Vandemaele P, Ingala S, Robertson AD, Václavů L, Groote I, Kuijf H, Zelaya F, O'Daly O, Hilal S, Wink AM, Kant I, Caan MWA, Morgan C, de Bresser J, Lysvik E, Schrantee A, Bjørnebekk A, Clement P, Shirzadi Z, Kuijer JPA, Wottschel V, Anazodo UC, Pajkrt D, Richard E, Bokkers RPH, Reneman L, Masellis M, Günther M, MacIntosh BJ, Achten E, Chappell MA, van Osch MJP, Golay X, Thomas DL, De Vita E, Bjørnerud A, Nederveen A, Hendrikse J, Asllani I, Barkhof F. ExploreASL: An image processing pipeline for multi-center ASL perfusion MRI studies. Neuroimage. 2020 Oct 1;219:117031. doi: 10.1016/j.neuroimage.2020.117031. Epub 2020 Jun 8. PMID: 32526385.
6. Norman LJ, Sudre G, Bouyssi-Kobar M, Sharp W, Shaw P. A Longitudinal Study of Resting-State Connectivity and Response to Psychostimulant Treatment in ADHD. Am J Psychiatry. 2021 Aug 1;178(8):744-751. doi: 10.1176/appi.ajp.2021.20091342. Epub 2021 Jun 4. PMID: 34086483; PMCID: PMC8528221.
7. Nasky KM, 2018. Stimulant Dose Conversion Calculator. https://psychopharmacopeia.com/stimulant_conversion.php
Figures