1731
Common and distinct volumetric alterations of hypothalamic subunits between female patients with anorexia nervosa and bulimia nervosa1Department of Radiology and Huaxi MR Research Center (HMRRC), Functional and Molecular Laging Key Laboratory of Sichuan Province, West China Hospital, Sichuan University, Chengdu, China, Chengdu, China, 2Mental Health Center, West China Hospital of Sichuan University, Sichuan Clinical Medical Research Center for Mental Disorders, Chengdu, China, Chengdu, China, 3Institue of psychoradiology, West China Xiamen Hospital of Sichuan University, Xiamen, China, Xiamen, China
Synopsis
Keywords: Psychiatric Disorders, Neuroscience
Motivation: The structural alterations of hypothalamic subunits involved in the pathophysiology of anorexia nervosa (AN) and bulimia nervosa (BN) remain undetermined.
Goal(s): To investigate the common and distinct alterations in the volumes and structural covariance networks (SCN) of hypothalamic subunits between AN and BN.
Approach: The MRI data were subsegmented and underwent multistage quality control using FreeSurfer, in conjunction with MANCOVA and graph theory analysis.
Results: Larger volumes in the right a-iHyp were found in BN, smaller volumes in the left infTub and right supTub were found in AN, compared to HCs. Global efficacy and characteristic path length altered in AN relative to BN.
Impact: We depict distinct alterations of hypothalamic subunits involved in the pathophysiology of AN and BN. These findings provide novel insight into the role of the hypothalamus in both AN and BN.
INTRODUCTION
The hypothalamus, consisting of several subunits, plays a key role in the pathophysiology of both anorexia nervosa (AN) and bulimia nervosa (BN)[1]. For example, the lateral hypothalamic area (LHA), which stimulates hunger [2], and the ventromedial hypothalamus (VMH) contribute to feelings of satiety [3]. Numerous studies have underscored changes in brain structures in patients with AN [4] and BN[5]. However, the neuroanatomical alterations of the hypothalamus in AN and BN remain relatively undetermined mainly due to methodological limitations. Previous structural imaging in AN and BN often measured the whole hypothalamus rather than considering its discrete subunits. Furthermore, the available literature is not consistent, with reports of smaller [6, 7] and no differences [8] in hypothalamic whole volumes in AN patients compared to healthy controls (HCs). Only one study reported no difference [9] in hypothalamic whole volumes between BN and HCs. One study reported significantly smaller volumes in the mammillary body as part of the hypothalamus in AN than in HCs [10]. However, the common and distinct alterations of hypothalamic subunits in AN and BN remain undetermined. Recent advances in deep machine learning have enabled highly accurate, fully automated segmentation of the whole hypothalamus based on deep convolutional neural networks (CNNs) [11]. Here, we investigated for the first time the volumes and structural covariance network (SCN) of hypothalamic subunits in female patients with AN and BN.METHODS
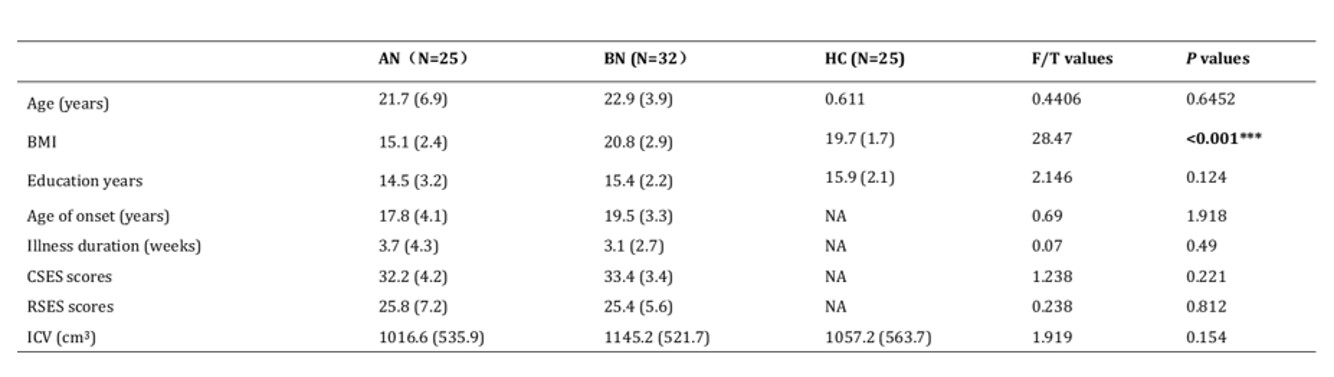
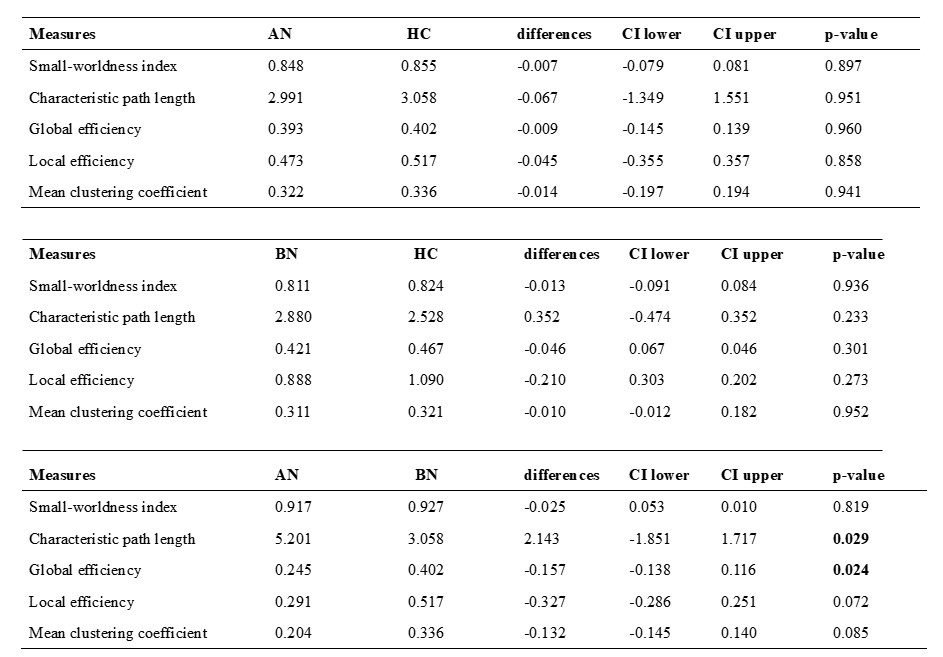
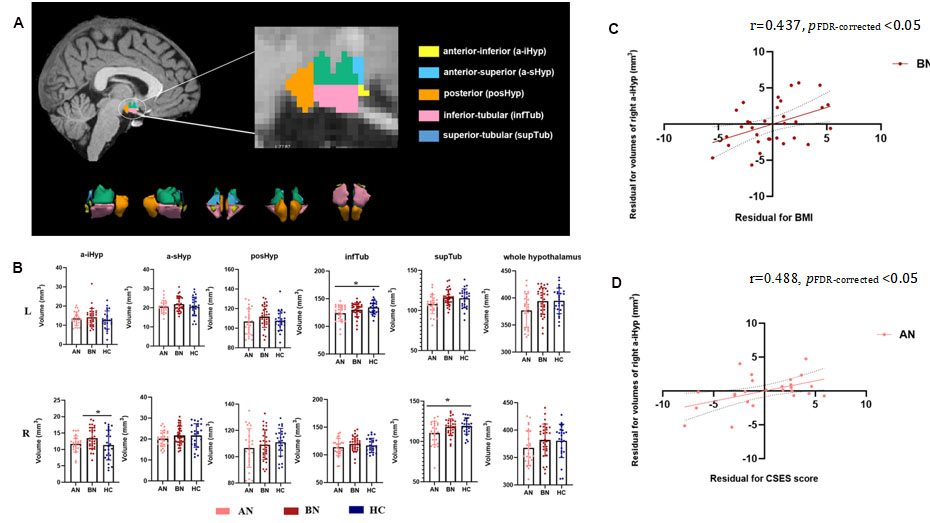
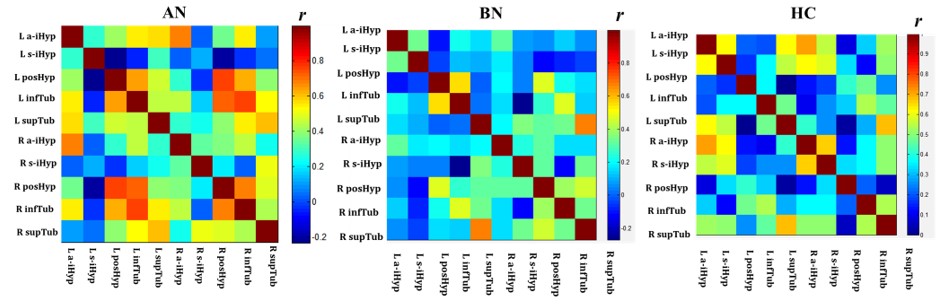
A total of 25 female patients with AN, 32 female patients with BN and 25 age-, education years-matched females HCs were included in this study after giving written informed consent. Both the AN and BN patients were medication-free. All patients completed the Core Self-Evaluation Scale (CSES) to assess core self-evaluation and the Rosenberg Self-Esteem Scale (RSES) to assess self-esteem. All High-resolution, T1-weighted images scans were performed using a Philips 3.0T MRI scanner, and were automatically segmented and measured using an automated segmentation module in FreeSurfer (V 7.3.2) based on CNNs via deep machine learning methods [10]. The hypothalamus was segmented into five subunits, including anterior-inferior (a-iHyp), anterior-superior (a-sHyp), posterior (posHyp), inferior tubular (infTub) and superior tubular (supTub). All segmentations were visually inspected following a QC protocol that is similar to hippocampal subfield QC by the ENIGMA consortium. No MRl measurements for participants showed signs of software failure in hypothalamic subunit measurements. We conducted multivariate analysis of covariance (MANCOVA) to test for group differences in the volumes of hypothalamus and hypothalamic subunits among AN, BN and HCs, with age, education years and intracranial volume (ICV) as covariates. Post hoc two-by-two t-test were conducted. Partial correlation analyses were performed to identify the associations of hypothalamic measures with BMI, illness duration, age of onset, CSES and RSES scores in the patients with AN and BN respectively, controlling for age, education years and ICV. A false discovery rate (FDR) correction was applied to correct for multiple hypothesis testing issues in above-mentioned analyses. We also performed an analysis of the SCN of hypothalamic subunits using graph theory via the BRAH. The characteristic path length, global efficiency, local efficiency, clustering coefficient, small-worldness index) were compared between groups by testing the statistical significance of the differences using nonparametric permutation tests with 1000 permutations.RESULTS
The demographic information and clinical characteristics of the subjects are shown in Table 1. The volumes of left and right whole hypothalamus and hypothalamic subunits were not significantly different among the AN, BN and HC groups (Fig. 1). However, post hoc analysis found larger volumes in right a-iHyp in BN , while smaller volumes in left infTub and right supTub in AN patients than those in HCs (pFDR-corrected <0.05, Fig. 1). The volumes of right a-iHyp were positively correlated with BMI (r=0.437, pFDR-corrected <0.05) in BN patients and CSES scores (r=0.488, pFDR-corrected <0.05) in AN patients, respectively. The global efficacy was decreased, whereas the characteristic path length was increased in AN relative to BN (p<0.05, Table 2).DISCUSSION & CONCLUSION
To the best of our knowledge, this is the first study investigating the volumes and SCN of the hypothalamic subunits in AN and BN and comparing these measures between AN and BN. These findings demonstrated that anterior hypothalamic are involved in BN, while tubular hypothalamic are involved in AN. Moreover, the divergences in the SCN of the hypothalamic subunit between AN and BN provide differential evidence at the local network level. The enlargement of the right a-iHyp might be linked to weight restoration in BN and disruption of the core self-evaluation in AN. Overall, these findings provide novel insight into the role of the hypothalamus in both AN and BN.Acknowledgements
This study was supported by grants from National Key R&D Program of China (Grant No. 2022YFF202405); Natural Science Foundation of Sichuan Province (2022NSFSC0052) and the 1.3.5 Project for Disciplines of Excellence, West China Hospital, Sichuan University (Grant No. ZYJC21041).References
1. Berner, L.A., et al., Neuroendocrinology of reward in anorexia nervosa and bulimia nervosa: Beyond leptin and ghrelin. Mol Cell Endocrinol, 2019. 497: p. 110320.
2. Berrios, J., et al., Food cue regulation of AGRP hunger neurons guides learning. Nature, 2021. 595(7869): p. 695-700.
3. Zhang, J., et al., An excitatory ventromedial hypothalamus to paraventricular thalamus circuit that suppresses food intake. Nat Commun, 2020. 11(1): p. 6326.
4. Su, T., et al., Structural and functional brain alterations in anorexia nervosa:A multimodal meta-analysis of neuroimaging studies. Hum Brain Mapp, 2021. 42(15): p. 5154-5169.
5. Donnelly, B., et al., Neuroimaging in bulimia nervosa and binge eating disorder: a systematic review. J Eat Disord, 2018. 6: p. 3.
6. Boghi, A., et al., In vivo evidence of global and focal brain alterations in anorexia nervosa. Psychiatry Res, 2011. 192(3): p. 154-9.
7. Titova, O.E., et al., Anorexia nervosa is linked to reduced brain structure in reward and somatosensory regions: a meta-analysis of VBM studies. BMC Psychiatry, 2013. 13: p. 110.
8. van Opstal, A.M., et al., Hypothalamic BOLD response to glucose intake and hypothalamic volume are similar in anorexia nervosa and healthy control subjects. Front Neurosci, 2015. 9: p. 159. 9. Amianto, F., et al., Brain volumetric abnormalities in patients with anorexia and bulimia nervosa: a voxel-based morphometry study. Psychiatry Res, 2013. 213(3): p. 210-6.
10. Billot,
B., et al., Automated segmentation of the
hypothalamus and associated subunits in brain MRI. Neuroimage, 2020. 223: p. 117287.
Figures