1722
Abnormal amygdala resting-state functional connectivity in patients with anxiety disorders: A coordinate-based imaging meta-analysis.1Huaxi MR Research Center (HMRRC), Department of Radiology, West China Hospital of Sichuan University, Chengdu, China, 2Research Unit of Psychoradiology, Chinese Academy of Medical Sciences, Chengdu, China, 3Department of Radiology, West China Xiamen Hospital of Sichuan University, Xiamen, China
Synopsis
Keywords: Psychiatric Disorders, fMRI (resting state), anxiety disorders
Motivation: It is necessary to clarify the neurobiological mechanisms of anxiety disorders (ADs) to provide a unique biomarker for diagnosing ADs, facilitating accurate clinical diagnosis and targeted therapeutic interventions.
Goal(s): The primary objective is to elucidate the specific abnormalities in individuals with ADs' amygdala-based whole-brain connectivity.
Approach: The coordinate-based meta-analysis was conducted to find amygdala resting-state functional connectivity in patients with ADs. Furthermore, subgroup analysis was performed to explore potential functional lateralization.
Results: Distinct functional connectivity abnormalities were found in ADs, which provides a reference for diagnosing ADs.
Impact: These findings not only enhance our understanding of the underlying pathophysiological mechanisms in ADs but also may be valuable for the prevention, diagnosis and intervention of ADs.
INTRODUCTION
Although dysfunction of amygdala-related circuits is centrally implicated in anxiety disorders (ADs)[1, 2], previous neuroimaging studies using resting-state functional magnetic resonance imaging in ADs reported inconsistent findings on whole-brain functional connectivity of the amygdala. It is necessary to clarify the aberrant resting-state functional connectivity of the amygdala in ADs using Seed-based d Mapping with Permutation of Subject Images (SDM-PSI), which may contribute to the identification of potential biomarkers that could be valuable for the prevention, diagnosis and intervention of affective disorders.METHODS
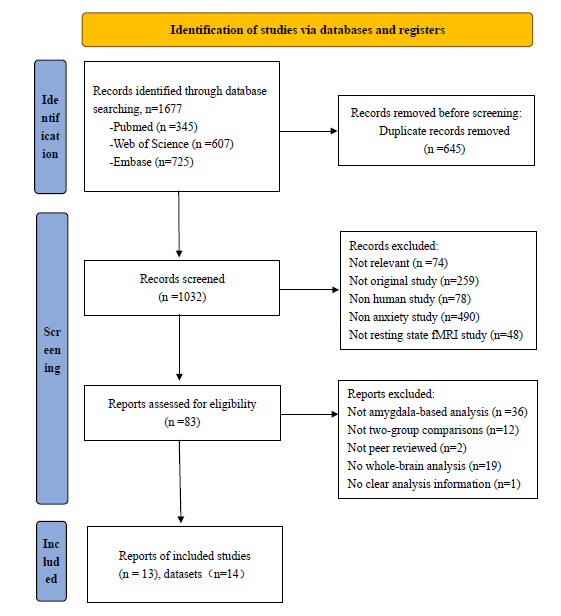
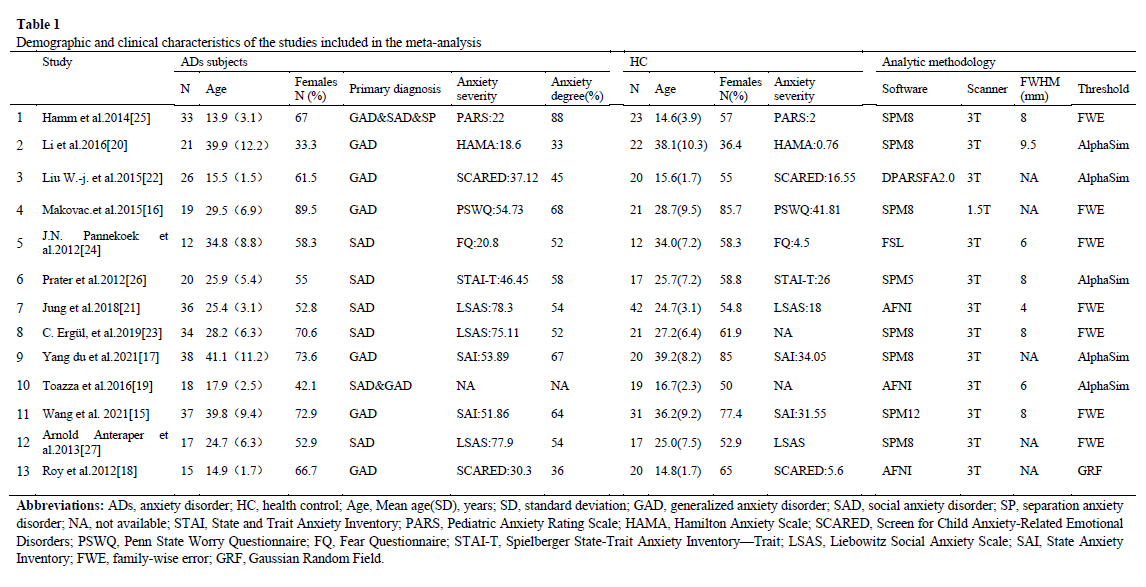
All relevant studies were systematically searched until April 6, 2023. Data were extracted from records directly contrasting ADs and healthy controls, including amygdala-based functional connectivity magnetic resonance imaging data. Subgroup analyses were used to control for age differences between studies and investigate potential differences in functional lateralization.RESULTS
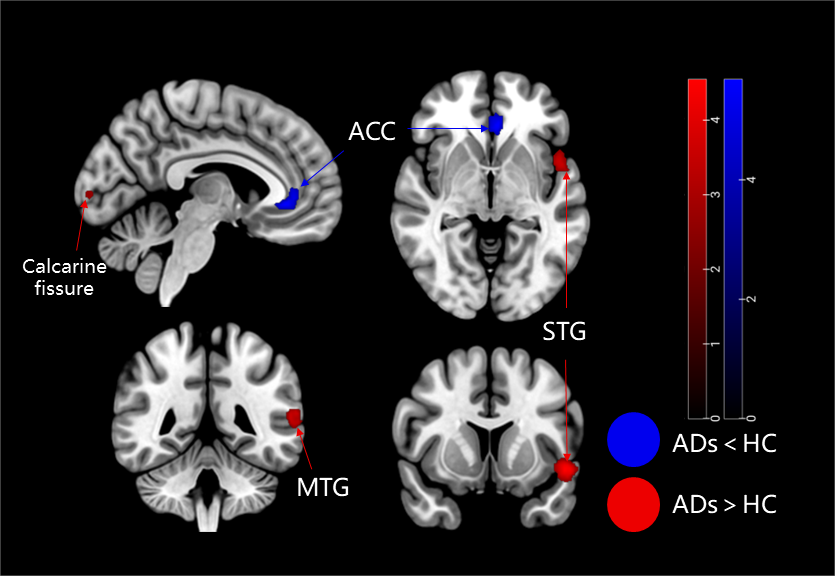
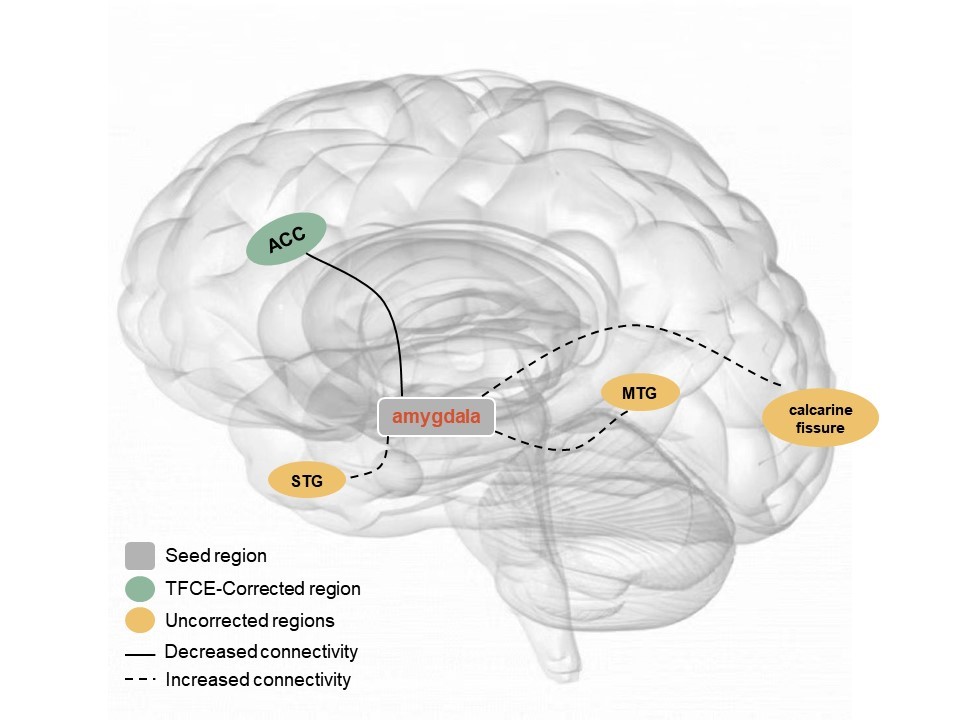
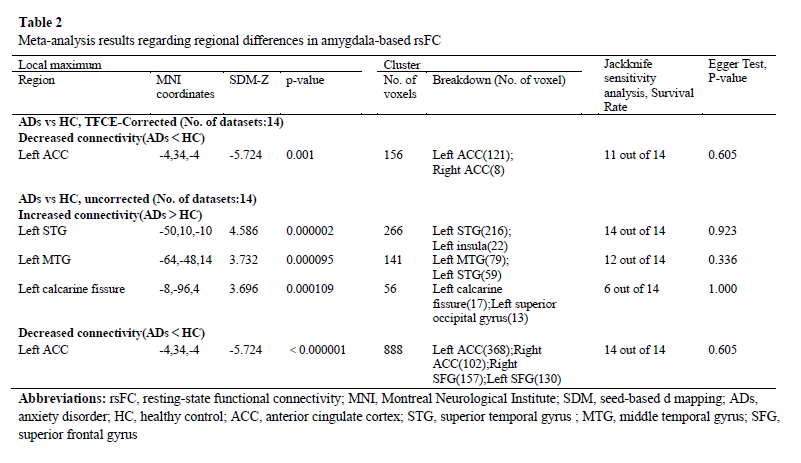
Fourteen datasets (336 ADs and 312 healthy controls) met the predefined inclusion and exclusion criteria of this meta-analysis. Detailed sample characteristics of each study were extracted and shown in Figure 1. After TFCE-Corrected, one consistent and strong decreased connectivity of the amygdala was observed with a large cluster centred at the left ACC and extending to the paracingulate gyri. In the relatively lenient case of uncorrected control before FWE correction, in addition to the left ACC, the resulting meta-analytical map includes 3 clusters of increased connectivity between the amygdala and other brain regions. Cluster 1 extends from the left STG to the insula. Cluster 2 extends from the left MTG to the left STG. Cluster 3 extends from the left calcarine fissure to the left superior occipital gyrus (Figure 2). The results of the adult subgroup analyses were highly consistent with the pooled meta-analysis findings. In the left amygdala-based meta-analysis, we found decreased amygdala connectivity with ACC, which is largely consistent with the results of the main analysis. In the right amygdala-based whole-brain meta-analysis, no significant results were found. Abnormal coupling of the amygdala to the ACC in the presence of functional lateralization.DISCUSSION
Through a comprehensive meta-analysis, we show for the first time the whole-brain resting-state amygdala-based abnormal FC in patients with ADs. Compared with HCs, ADs patients showed lower FC between the amygdala and the left ACC extending to the paracingulate gyrus. There is thought to be an anatomical and functional connection between the ACC and the amygdala. They work in synergy to process and regulate emotional responses. The decreased FC between the amygdala and ACC supports the hypothesis of a top-down emotion dysregulation model for ADs pathogenesis[3, 4]. Aberrant connectivity between the amygdala and ACC may underlie pervasive attention, interpretation, and memory bias towards threatening information and persistent negative self-reflection in ADs patients [5]. Amygdala-ACC FC may be a potential and promising target for treating ADs. Adult subgroup meta-analysis showed the same result of reduced rsFC in the adult study as the main analysis. This suggests no significant difference in FC abnormalities between adults and children with ADs. ADs patients showed increased FC between the amygdala and the following areas: left STG, insula, left MTG, and left calcarine fissure. The STG helps with word recognition, language comprehension, perception of emotional expression and the high-level cognitive process of fear experience and amygdala activity regulation [6, 7]. The increased rsFC between the amygdala and STG may lead to an overreaction to sensations and an inaccurate understanding of information. MTG is interconnected with the STG in terms of anatomical location and function. Increased FC between the amygdala and MTG may reflect an enhanced susceptibility to inaccurate interpretation of stimuli [8]. The insula is structurally connected to the amygdala and is involved in perceiving interoceptive states and emotional processing [9]. When analyzing the bilateral amygdala separately as seed regions, we observed that the left amygdala demonstrated decreased rsFC with ACC, whereas the right amygdala did not yield statistically significant results. This indicates that the ACC exhibited different patterns of hemispheric asymmetry in rsFC with the left and right amygdala in ADs patients compared to HCs. The left amygdala predominates in the rsFC of ADs patients. Systematic whole-brain jack-knife sensitivity analysis and heterogeneity analysis provide reliable results. Consequently, these findings depicted the neurocircuit model of ADs traditional pathophysiology through the brain's intrinsic connectivity and elaborated on the neural mechanisms of ADs.Acknowledgements
No acknowledgement found.References
1. Sergerie K, Chochol C, Armony JL: The role of the amygdala in emotional processing: a quantitative meta-analysis of functional neuroimaging studies. Neurosci Biobehav Rev 2008, 32(4):811-830.
2. Habel U, Windischberger C, Derntl B, Robinson S, Kryspin-Exner I, Gur RC, Moser E: Amygdala activation and facial expressions: explicit emotion discrimination versus implicit emotion processing. Neuropsychologia 2007, 45(10):2369-2377.
3. Mochcovitch MD, da Rocha Freire RC, Garcia RF, Nardi AE: A systematic review of fMRI studies in generalized anxiety disorder: evaluating its neural and cognitive basis. J Affect Disord 2014, 167:336-342.
4. Roy AK, Shehzad Z, Margulies DS, Kelly AM, Uddin LQ, Gotimer K, Biswal BB, Castellanos FX, Milham MP: Functional connectivity of the human amygdala using resting state fMRI. Neuroimage 2009, 45(2):614-626.
5. Bogels SM, Mansell W: Attention processes in the maintenance and treatment of social phobia: hypervigilance, avoidance and self-focused attention. Clin Psychol Rev 2004, 24(7):827-856.
6. Phillips ML YA, Scott SK, Calder AJ, Andrew C, Giampietro V, Williams SC, Bullmore ET, Brammer M, Gray JA: Neural responses to facial and vocal expressions of fear and disgust. Proc Biol Sci 1998.
7. Quirk GJ, Armony JL, LeDoux JE: Fear conditioning enhances different temporal components of tone-evoked spike trains in auditory cortex and lateral amygdala. Neuron 1997.
8. Pannekoek JN, Veer IM, van Tol MJ, van der Werff SJ, Demenescu LR, Aleman A, Veltman DJ, Zitman FG, Rombouts SA, van der Wee NJ: Resting-state functional connectivity abnormalities in limbic and salience networks in social anxiety disorder without comorbidity. Eur Neuropsychopharmacol 2013, 23(3):186-195.
9. Phan KL, Wager T, Taylor SF, Liberzon I: Functional neuroanatomy of emotion: a meta-analysis of emotion activation studies in PET and fMRI. Neuroimage 2002, 16(2):331-348.
Figures