1710
Association of MRI Findings with Paraspinal Muscles Fat Infiltration in Patients with Chronic Low Back Pain: A Multicenter Study1The First Affliated Hospital of Kunming Medical University, Yun Nan, China, 2GE HealthCare MR Research, Beijing, China
Synopsis
Keywords: fMRI Analysis, fMRI
Motivation: Understanding the link between paraspinal muscle changes and common causes is crucial for improving treatment approaches for chronic lower back pain (CLBP), which has diverse underlying factors.
Goal(s): Assessing the relationship between MRI findings and paraspinal muscle changes in patients with CLBP.
Approach: We prospectively collected lumbar spine MRI images from CLBP patients. Analyses assessed correlations and regressions between MRI findings and paraspinal muscle cross-sectional area (CSA) and proton density fat fraction (PDFF).
Results: Degenerative lumbar spondylolisthesis (DLS) and intervertebral disc degeneration (IVDD) have a significant impact on the increase in the PDFF of paraspinal muscles.
Impact: This study provides valuable insights for clinicians, enabling them to implement targeted interventions for CLBP patients based on specific MRI findings and key characteristics of muscle remodeling. By improving prevention and treatment approaches.
Introduction
CLBP poses challenges in developing effective prevention and treatment strategies due to its diverse etiology. Common causes of CLBP include IVDD, disc herniation, DLS, facet joint disease, and spinal stenosis1-9. However, The link between these causes and paraspinal muscle fat infiltration in CLBP patients is still debated. It's uncertain if these associations are most prominent individually. Also, the impact of severity or the combination of factors and MRI-identified issues on these links is unclear. This study explores links between lumbar degenerative conditions, paraspinal muscles, and CLBP. Through this, we seek to comprehend their role in CLBP development better. This knowledge can help uncover the underlying mechanisms of CLBP and guide the development of more effective treatment strategies.Methods
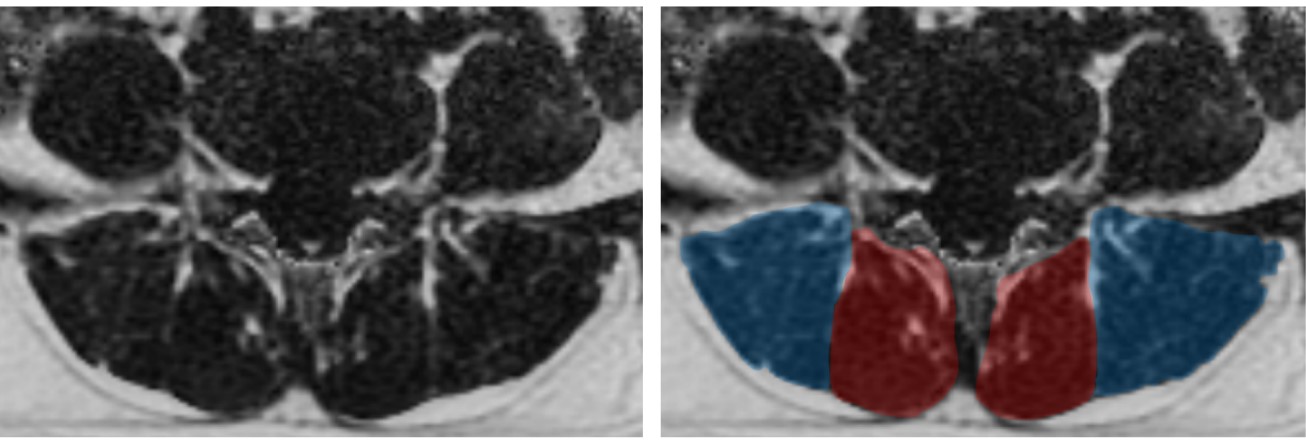
The study obtained institutional review board approval and verbal consent from all participants. The CLBP patient cohort came from four healthcare facilities based on specific criteria. All MR examinations utilized a 3.0T MR scanner (Discovery MR 750, GE Healthcare Systems, Milwaukee, WI, USA) equipped with a 24-channel phased-array spine coil. The sequences include sagittal T2-weighted imaging, T1-weighted imaging, axial T2WI, and the IDEAL-IQ sequence.MRI findings encompassed assessments of DLS, IVDD, facet arthrosis, disc bulge, and disc herniation in regular sequences. Multifidus (MF) and erector spinae (ES) CSA and PDFF were evaluated in IDEAL-IQ sequences, specifically at the mid-levels of the L4/5 and L5/S1 intervertebral discs(Figure 1). Muscle fascia and attachment points were delineated using GE Healthcare's Advantage Workstation 4.6. Statistical analysis was carried out using SPSS 26.0 software (IBM Corp, Armonk, NY, USA). Pearson and Spearman's correlations assessed MRI findings' relation to paraspinal muscle changes in CLBP patients. Univariate and multivariate regression identified risk factors for paraspinal muscle fat infiltration, adjusting for age, sex, and BMI in CLBP patients.Results
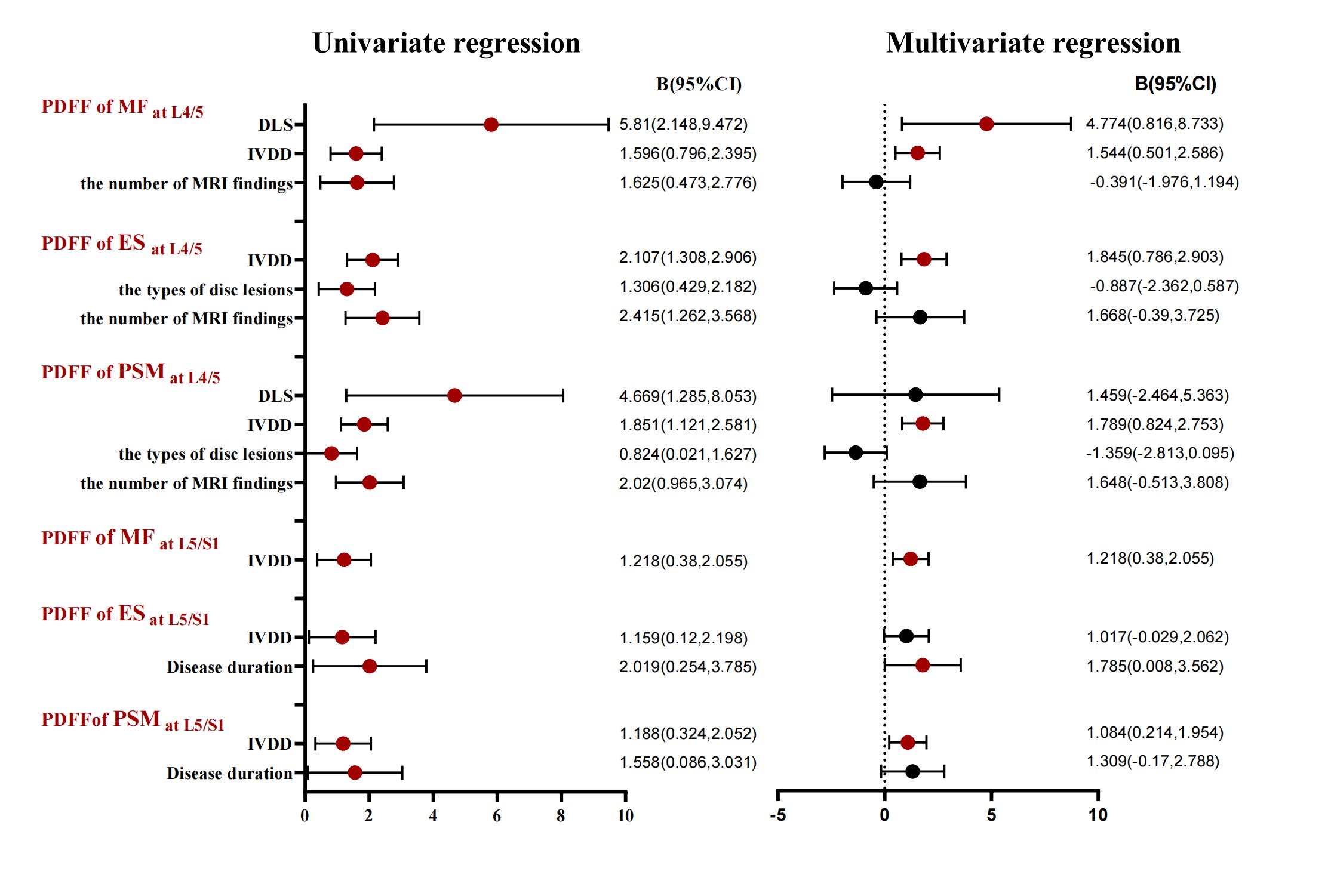
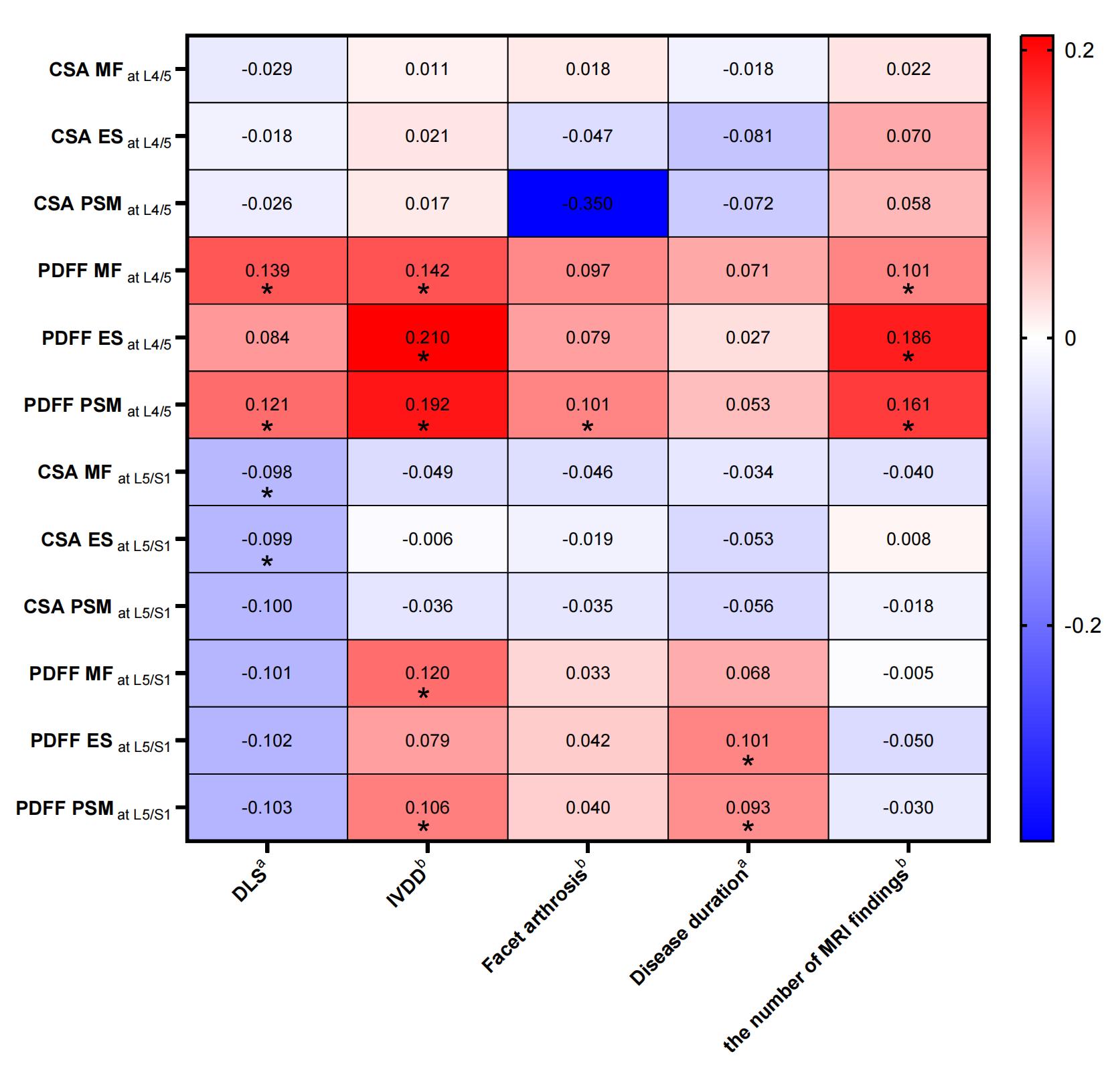
A total of 493 CLBP patients were included in the study. correlation analysis results indicate that IVDD, facet arthrosis, and DLS at the L4-S1 level, are correlated with the PDFF of paraspinal muscles. Multivariate regression analysis indicates that IVDD is the primary factor influencing the paraspinal muscle PDFF at the L4-S1 level (BES at L4/5=1.845, P<0.05); DLS was a factor affecting the PDFF of MF at the L4/5 level (B=4.774, P<0.05). After including age, gender, and BMI,The above-mentioned impact on paraspinal muscle PDFF is no longer statistically significant.(Figure 2 and Figure 3)Discussion
Our study's linear regression findings suggest that disc bulge/herniation at the L4/L5 level affects nearby paraspinal muscles, consistent with previous single-factor research on muscle fat infiltration. However, when combined with other factors in multivariate analysis, disc bulge/herniation doesn't independently influence muscle fat infiltration. Additionally, IVDD and DLS are significant influencing factors for fat infiltration of the paraspinal muscles. Nevertheless, after adjusting for factors that could potentially influence muscle fat as control variables, the effects of IVDD and DLS on paraspinal muscle fat infiltration have disappeared. Previous studies have reported that age and gender affect overall muscle mass, which further affects back muscle atrophy and fat infiltration, and as age increases, fat infiltration increases 2, 10 One study found that women have more fat infiltration in the MF and ES muscles at the L4-S1 levels, as well as men have more fat infiltration in the PS at the L5/S1 level3, which may be related to the decrease in muscle function due to hormone deficiency after menopause12, 13 and the chosen level of the intervertebral disc8. While the association between paraspinal muscle fat infiltration and BMI remains a matter of debate8, 12, 14 In conjunction with the above research results and existing pieces of literature, our study further substantiates that age, gender, and BMI are important factors for the degree of paraspinal muscle fat infiltration in CLBP patients. Before adjusting these personal factors as covariates, the significant influence exhibited by DLS and the IVDD on paraspinal muscle fat infiltration shown in this study was confounded by the overlapping influence of age, gender, and BMI on the degree of muscle fat infiltration. We argue that the clinical significance of individual factors in paraspinal muscle quality changes is uncertain. Associations seen in prior single-factor studies could be coincidental.Conclusion
In conclusion, our MRI findings in CLBP patients indicate that DLS and the IVDD have a significant impact on the increase in paraspinal muscle PDFF. Additionally, age, gender, and BMI are important factors influencing the degree of muscle fat infiltration in CLBP patients.Acknowledgements
No acknowledgement found.References
1. Noonan AM, Brown SHM. Paraspinal muscle pathophysiology associated with low back pain and spine degenerative disorders. JOR Spine. 2021;4(3):e1171. Epub 2021/10/07. doi: 10.1002/jsp2.1171. PubMed PMID: 34611593; PubMed Central PMCID: PMCPMC8479522.
2.Huang Y, Wang L, Zeng X, Chen J, Zhang Z, Jiang Y, et al. Association of Paraspinal Muscle CSA and PDFF Measurements With Lumbar Intervertebral Disk Degeneration in Patients With Chronic Low Back Pain. Front Endocrinol (Lausanne). 2022;13:792819. Epub 2022/06/21. doi: 10.3389/fendo.2022.792819. PubMed PMID: 35721738; PubMed Central PMCID: PMCPMC9204273.
3. Wang Z, Zhao Z, Han S, Hu X, Ye L, Li Y, et al. Advances in research on fat infiltration and lumbar intervertebral disc degeneration. Frontiers in Endocrinology. 2022;13. doi: 10.3389/fendo.2022.1067373.
4. Huang Y, Wang L, Luo B, Yang K, Zeng X, Chen J, et al. Associations of Lumber Disc Degeneration With Paraspinal Muscles Myosteatosis in Discogenic Low Back Pain. Front Endocrinol (Lausanne). 2022;13:891088. Epub 2022/06/01. doi: 10.3389/fendo.2022.891088. PubMed PMID: 35634490; PubMed Central PMCID: PMCPMC9136003.
5. Cooley JR, Jensen TS, Kjaer P, Jacques A, Theroux J, Hebert JJ. Spinal degeneration is associated with lumbar multifidus morphology in secondary care patients with low back or leg pain. Scientific Reports. 2022;12(1). doi: 10.1038/s41598-022-18984-1.
6. Cao B, Zuo Y, Xu Y, Wu F, Du H, Hou Y, et al. Correlation between fat infiltration of paraspinal muscle and L4 degenerative lumbar spondylolisthesis in asymptomatic adults. Asian J Surg. 2023;46(2):834-40. Epub 2022/09/13. doi: 10.1016/j.asjsur.2022.08.097. PubMed PMID: 36096928.
7. Jung M, Rospleszcz S, Loffler MT, Walter SS, Maurer E, Jungmann PM, et al. Association of lumbar vertebral bone marrow and paraspinal muscle fat composition with intervertebral disc degeneration: 3T quantitative MRI findings from the population-based KORA study. Eur Radiol. 2023;33(3):1501-12. Epub 2022/10/15. doi: 10.1007/s00330-022-09140-4. PubMed PMID: 36241920; PubMed Central PMCID: PMCPMC9935727.
8. Shi L, Yan B, Jiao Y, Chen Z, Zheng Y, Lin Y, et al. Correlation between the fatty infiltration of paraspinal muscles and disc degeneration and the underlying mechanism. BMC Musculoskelet Disord. 2022;23(1):509. Epub 2022/06/01. doi: 10.1186/s12891-022-05466-8. PubMed PMID: 35637476; PubMed Central PMCID: PMCPMC9150320.
9. Marty B, Reyngoudt H, Boisserie J-M, Le Louër J, C. A. Araujo E, Fromes Y, et al. Water-Fat Separation in MR Fingerprinting for Quantitative Monitoring of the Skeletal Muscle in Neuromuscular Disorders. Radiology. 2021;300(3):652-60. doi: 10.1148/radiol.2021204028.
10. Urrutia J, Besa P, Lobos D, Campos M, Arrieta C, Andia M, et al. Lumbar paraspinal muscle fat infiltration is independently associated with sex, age, and inter-vertebral disc degeneration in symptomatic patients. Skeletal Radiol. 2018;47(7):955-61. Epub 2018/01/31. doi: 10.1007/s00256-018-2880-1. PubMed PMID: 29379999.
11. Ozcan-Eksi EE, Eksi MS, Akcal MA. Severe Lumbar Intervertebral Disc Degeneration Is Associated with Modic Changes and Fatty Infiltration in the Paraspinal Muscles at all Lumbar Levels, Except for L1-L2: A Cross-Sectional Analysis of 50 Symptomatic Women and 50 Age-Matched Symptomatic Men. World Neurosurg. 2019;122:e1069-e77. Epub 2018/11/12. doi: 10.1016/j.wneu.2018.10.229. PubMed PMID: 30415054.
12. Kjaer P, Bendix T, Sorensen JS, Korsholm L, Leboeuf-Yde C. Are MRI-defined fat infiltrations in the multifidus muscles associated with low back pain? BMC Med. 2007;5:2. Epub 2007/01/27. doi: 10.1186/1741-7015-5-2. PubMed PMID: 17254322; PubMed Central PMCID: PMCPMC1796893.
13. Sions JM, Elliott JM, Pohlig RT, Hicks GE. Trunk Muscle Characteristics of the Multifidi, Erector Spinae, Psoas, and Quadratus Lumborum in Older Adults With and Without Chronic Low Back Pain. J Orthop Sports Phys Ther. 2017;47(3):173-9. Epub 2017/02/06. doi: 10.2519/jospt.2017.7002. PubMed PMID: 28158957; PubMed Central PMCID: PMCPMC7064314.
14. Ozcan-Eksi EE, Turgut VU, Kucuksuleymanoglu D, Eksi MS. Obesity could be associated with poor paraspinal muscle quality at upper lumbar levels and degenerated spine at lower lumbar levels: Is this a domino effect? J Clin Neurosci. 2021;94:120-7. Epub 2021/12/06. doi: 10.1016/j.jocn.2021.10.005. PubMed PMID: 34863425.
Figures