1709
Dynamic 31P MRS Reveals Delayed PCr Depletion and Muscle Fatigue in Association with Exercise Training in Patients with Parkinson’s Disease1Advanced Imaging Research Center, University of Texas Southwestern Medical Center, Dallas, TX, United States, 2Department of Radiology, University of Texas Southwestern Medical Center, Dallas, TX, United States, 3Department of Physical Therapy, University of Texas Southwestern Medical Center, Dallas, TX, United States
Synopsis
Keywords: Muscle, Nervous system, Mitochondrial function, energy metabolism
Motivation: Parkinson’s disease (PD) is a leading neurodegenerative disorder. Currently there are no medical interventions or medications to slow the progression of PD. Rehabilitation for aerobics, strength and motor control is critical to consider as it ameliorates symptoms, decrease falls, and improves quality of life. However, the metabolic mechanism of rehab is not fully understood.
Goal(s): Report evidence that, upon targeted muscle exercise training, the muscle energetics is improved at cellular and molecular level.
Approach: PD patients were scanned by 31P MRS before and after a 4-week progressive strengthening program.
Results: Upon rehabilitation, PCr decline with exercise is slowed in parallel to delayed fatigue.
Impact: The metabolic findings in the present study support the note and practice that strength-focused rehab programs can benefit patients with PD in the management of their weakness and improving quality of life.
INTRODUCTION
Parkinson’s disease (PD) is a leading neurodegenerative disorder impacting motor control with signs of bradykinesia, rigidity, and postural instability (1). Currently there are no medical interventions or medications to slow the progression of PD (2), whereas exercise training (rehabilitation) for aerobics,strength and motor control is critical to consider as it ameliorates symptoms, decrease falls, and improves quality of life by properly addressing the underlying weakness, another progressive motor symptom in PD (3). Although the exact cause of weakness in PD is unknown, one theory indicates a central cause as supported by strength improvements with the use of dopaminergic drugs (4). An alternative theory points to peripheral weakness from muscle deconditioning with contributions from cortical neuromuscular recruitment or peripheral fatigue (4,5). Understanding the mechanism of exercise adaptation, the primary intervention with potential to slow strength decline, can guide treatment prescription and to drive evidence-based therapy in PD. 31P MRS has been successfully applied to investigation of muscle energy metabolism (6,7). Here we report non-invasive evidence that, upon targeted muscle exercise training, the depletion of PCr, the immediate energy buffer of ATP, is slowed in parallel to delayed fatigue during exercising.METHODS
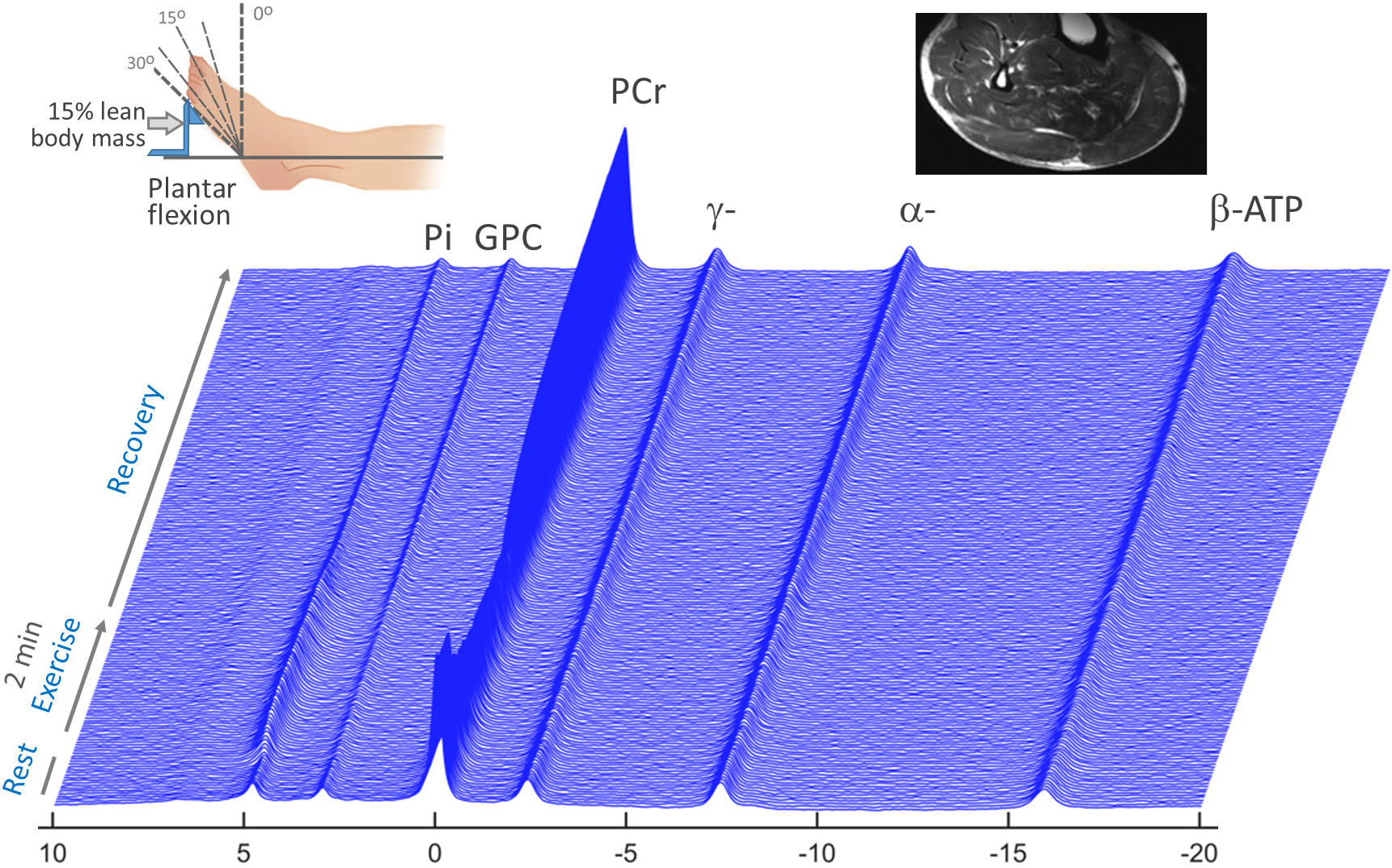
The study was conducted in 14 individuals clinically diagnosed with PD with inclusion criteria of Hoehn and Yahr stages 1- 4. The participants were scanned by 31P MRS before and after a 4-week progressive strengthening program (2 sets of heel raises to fatigue, 3 times a week). Calf muscle PCr depletion with exercise and recovery after exercise were measured on a 7T human MRI scanner. The in-magnet exercise was conducted in a supine position by single-legged rhythmic plantar flexion with the foot pushing against a pedal at a workload personalized to 15% of lean body mass, a rotation angle of 30o (full range), and a 2s repetition (1s push / 1s release) for 2-min. Data acquisition conditions TR = 2 s, NA = 1 s, number of dynamic scans 200 (15 at rest, 60 during exercise, and 125 post-exercise recovery). The time courses of the PCr (and Pi) signals, by integral, were fitting with a mono-exponential function to evaluation the steady-state depletion (and accumulation) levels and the corresponding time constants. A similar evaluation was also made on the recoveries of PCr and Pi signals after exercise. The t-test (at 95% confidence level) on the rehab effect and the linear correlation between before and after rehab were evaluated using internal functions in Matlab.RESULTS AND DISCUSSION
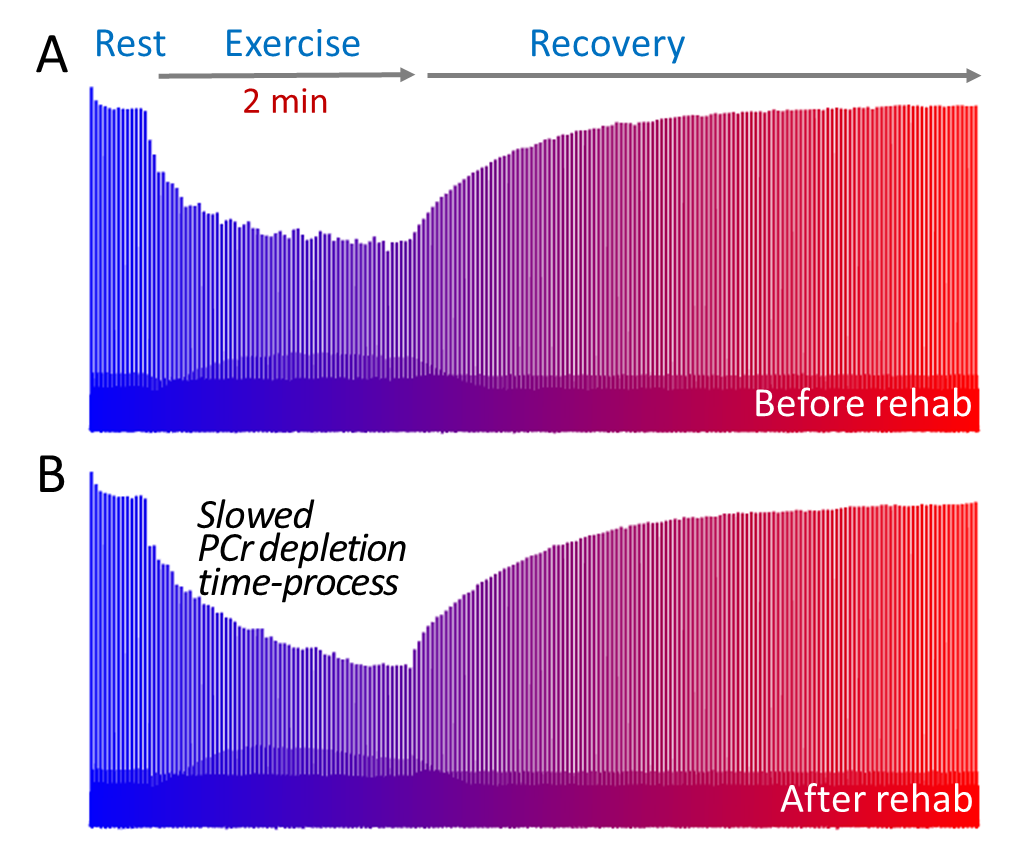
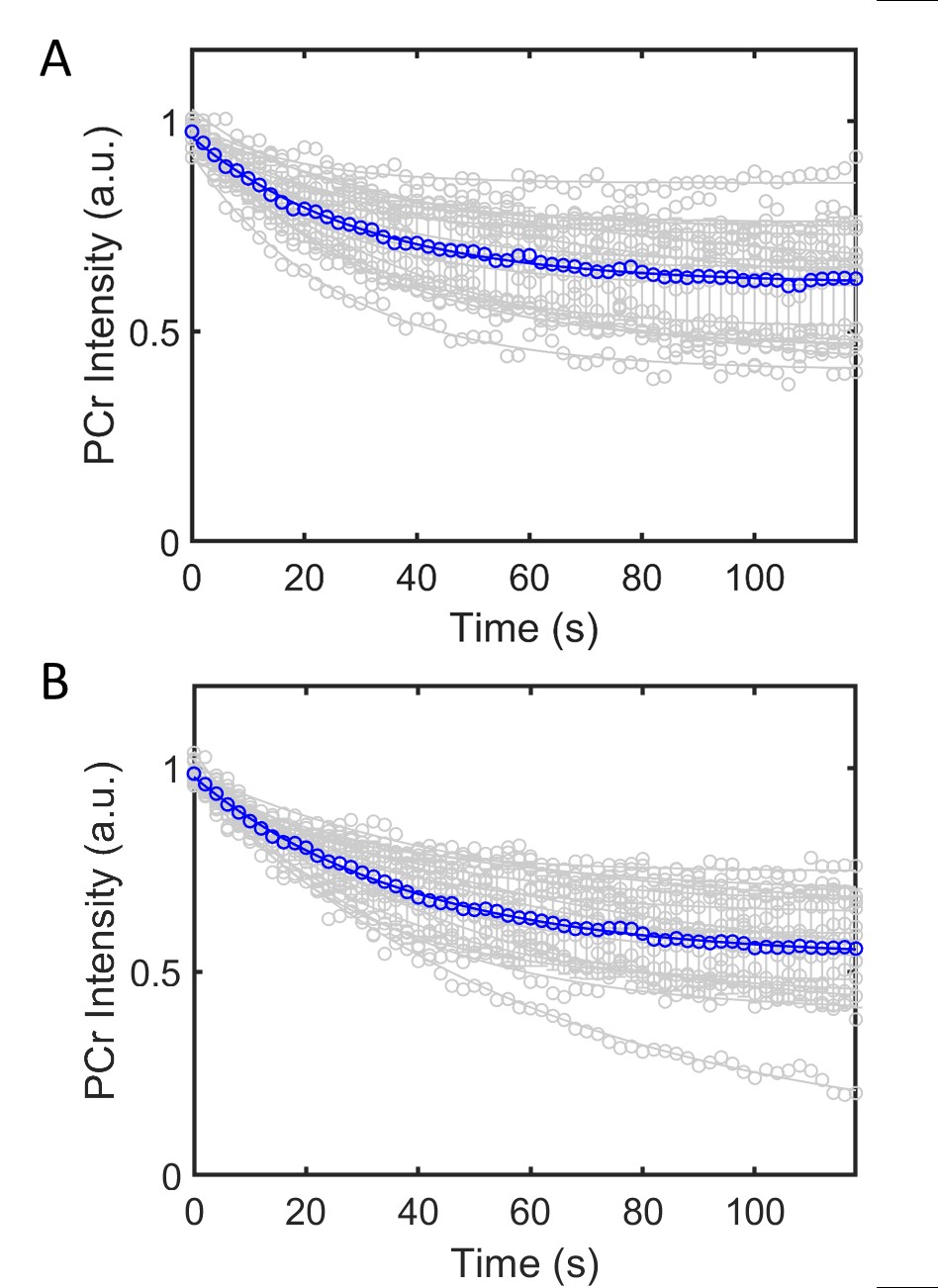
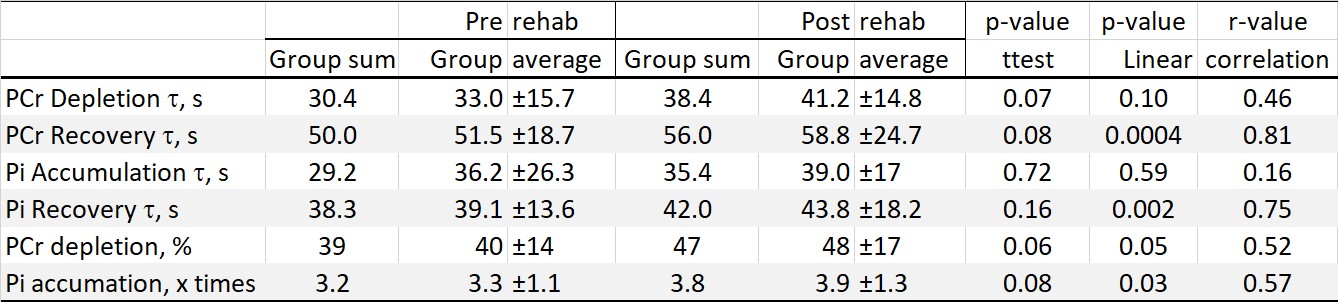
Figure 1 presents typical dynamic 31P MR spectra acquired from calf muscle of patients with PD, showing PCr depletion in parallel to Pi accumulation during muscle contraction and the subsequent recoveries toward resting levels following exercise. Figure 2 presents stack plots of dynamic PCr 31P signals before (A) and after (B) 4-wk rehabilitation, showing that the time course of PCr depletion is responsive to the strength training. Figure 3 shows PCr (A) and Pi (B) time courses acquired during exercise for individual patients. Table 1 summarizes the PCr and Pi time constants during and after exercise before and after rehab. A noticeable rehab effect is found at PCr, characterized by a limiting steady-state depletion of 48 ± 17%, which is 20% greater than that observed before rehab, and by a depletion time constant of 41.2 ± 14.8 s, which is approximately 30% slower than that observed before rehab (p = 0.07, n = 14). The result is consistent with the sign of muscle fatigue, i.e, reduced range of motion during plantar flexion, which occurred at a delayed time after rehab. Previous studies have shown an association between exercise training with an attenuation in PCr decline during exercise, suggestive of a reduced reliance on PCr energy buffer storage (6.7).CONCLUSION
In summary, using real-time dynamic 31P MRS, we found that the level of PCr limiting depletion (available for use as fuel) and the time constant for reaching PCr limiting depletion at steady state are both increased in patients with PD after strength-focused rehab. This metabolic improvement is in parallel to the sign of muscle fatigue that occurs during repetitive exercise. Given that patients with PD may have progressive weakness and that there is a lack of effective medical treatment for PD, this present metabolic finding supports that strength-focused rehab may benefit patients with PD in the management of weakness and improving quality of life.Acknowledgements
We thank instrumental support from the Human Imaging Core, the Advanced Imaging Research Center, at UTSW, operational assistance from Corey Mozingo, and technical support from Ivan Dimitrov.References
1. Paasuke, M., et al., Leg-extension strength and chair-rise performance in elderly women with Parkinson's disease. Journal of Aging and Physical Activity, 2004. 12(4): p. 511-24. 2. Fox, S.H., et al., International Parkinson and movement disorder society evidence‐based medicine review: update on treatments for the motor symptoms of Parkinson's disease. Movement Disorders, 2018. 33(8): p. 1248-1266. 3. Corcos, D.M., et al., A two‐year randomized controlled trial of progressive resistance exercise for Parkinson's disease. Movement Disorders, 2013. 28(9): p. 1230-1240. 4. Nallegowda, M., et al., Role of sensory input and muscle strength in maintenance of balance, gait, and posture in Parkinson's disease: a pilot study. American Journal of Physical Medicine and Rehabilitation, 2004. 83(12): p. 898-908. 5. David, F.J., et al., Progressive resistance exercise and Parkinson's disease: a review of potential mechanisms. Parkinsons Disease, 2012. 2012: p. 124527 6. Jones AM, Wilkerson DP, Berger NJ, and Fulford J. Influence of endurance training on muscle [PCr] kinetics during high-intensity exercise. Am J Physiol Regul Integr Comp Physiol 293: R392-401, 2007. 7. Burgomaster KA, Howarth KR, Phillips SM, Rakobowchuk M, Macdonald MJ, McGee SL, and Gibala MJ. Similar metabolic adaptations during exercise after low volume sprint interval and traditional endurance training in humans. J Physiol 586: 151-160, 2008.Figures