1699
The Role of MR Diagnosed Bilateral Patellar Tendinopathy on Pain and Quality of Life in Elite Athletes1Radiology, Stanford University, Stanford, CA, United States, 2Department of Radiology and Biomedical Imaging, University of California, San Francisco, San Francisco, CA, United States, 3Department of Radiology and Imaging, Hospital for Special Surgery, New York, NY, United States
Synopsis
Keywords: Tendon/Ligament, Tendon/Ligament, Knee, Tendinopathy, Joint, Patient Reported Outcomes, Sports Injury
Motivation: Patellar tendinopathy (PT) is a common athletic overuse injury affecting either or both knees that can lead to pain and early sport retirement. However, athlete reported differences between bilateral and unilateral PT remains unknown.
Goal(s): We tested the hypothesis that athletes with MRI signs of bilateral PT have more self-reported knee problems compared to athletes with no or unilateral PT.
Approach: 53 pre-season elite college athletes were bilaterally imaged and completed knee surveys. Statistical tests were conducted to determine differences between no, unilateral, or bilateral PT.
Results: Significant differences in pain and quality of life in athletes with bilateral PT exist.
Impact: Elite athletes with bilateral patellar tendinopathy (PT) have more pain and a reduced quality of life, problems that may keep athletes from optimal sport performance. MR may help identify at-risk athletes for preventive care, potentially keeping athletes from further injury.
INTRODUCTION
Patellar tendinopathy (PT) is a common overuse injury in jumping sports, such as basketball, often causing long-term knee pain, disability, and early sport retirement1. PT presents itself as pain to the inferior patella in which the pain increases with activity2. PT can affect either or both knees, with studies reporting a prevalence of 32% in elite male basketball players reporting presence of current PT symptoms3. PT is related to higher activity levels4 and athlete demographics1 and may not be the primary source of knee pain5. However, it remains unknown whether there is a difference in pain between athletes with bilateral and unilateral PT.This study analyzed pre-season Division 1 (D1) basketball players and swimmers to test the hypothesis that athletes with MRI signs of bilateral PT have more self-reported knee pain compared to athletes with no or unilateral PT.
METHODS
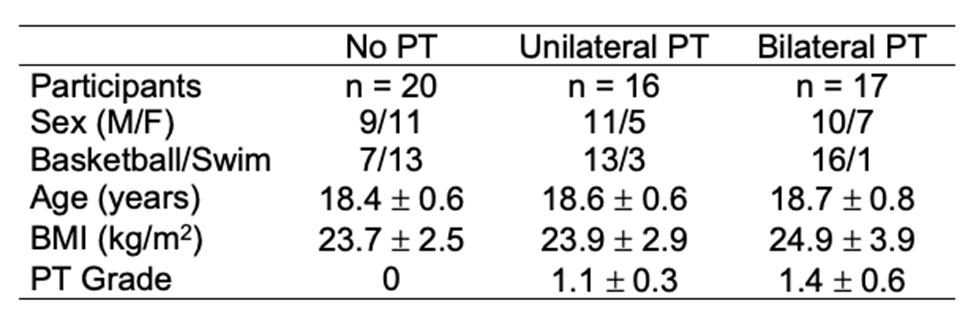
Fifty-three D1 elite athletes participated in this multicenter Institutional Review Board approved study. Thirty-six first-year college basketball players and 17 swimmers were bilaterally imaged pre-season using a 3 Tesla (3T) with 2-dimensional (2D) proton density (PD) fast spin echo (FSE) with fat saturation scans acquired in the oblique sagittal plane. Participants completed the Knee injury and Osteoarthritis Outcome Score (KOOS) survey, a measure of knee health in five individual subscales: pain, symptoms, function during activities of daily living (ADL), function in sports and recreation (Sport), and quality of life (QOL)6. KOOS subscale scores ranged from 0-100 with a lower score signifying more knee problems6. A radiologist graded the FSE knee images using a Modified Noyes classification system that scored the patellar tendon. A grade of 0 had no increased signal intensity, and a grade of 3 had increased signal intensity on > 66% of the tendon cross-section (Figure 1). Athletes were stratified into groups: no (PT grade=0), unilateral (one knee, PT grade ≥1), or bilateral PT (both knees, PT grade ≥1) (Table 1). Differences in KOOS were determined through a Kruskal Wallis test with Wilcoxon Rank Sum post-hoc tests with Bonferroni corrections (α=0.05).RESULTS
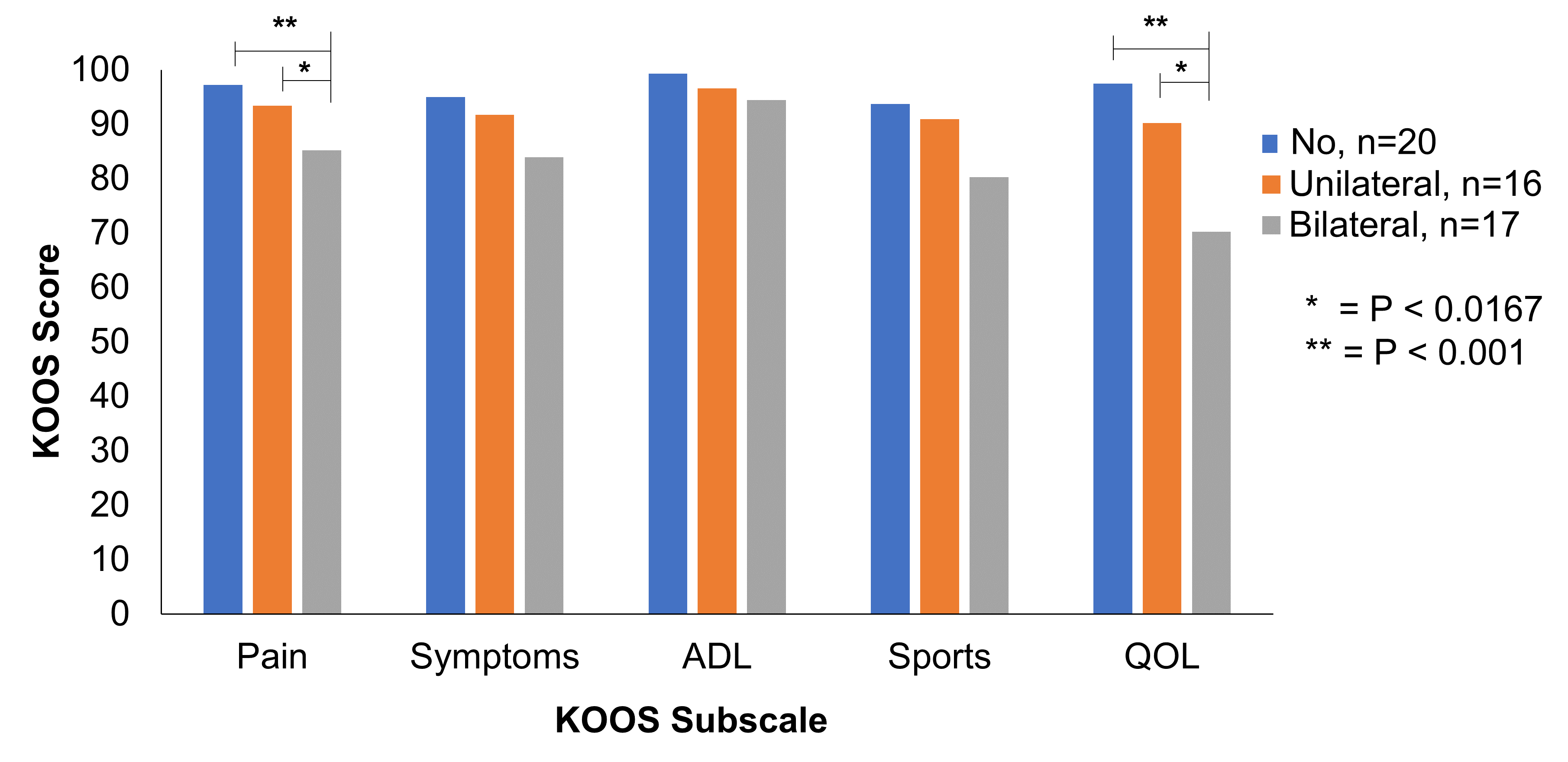
Athletes with bilateral PT had significantly more pain (KOOS_pain=85.2±11.1) than athletes who had no PT (KOOS_pain=97.2±2.7, P <0.001) or unilateral PT (KOOS_pain=93.4±11.5, P <0.01) PT. Athletes with bilateral PT also had reduced QOL (KOOS_QOL=70.2±17.8) compared to athletes with no PT(KOOS_QOL=97.5±4.3, P <0.001) and unilateral PT (KOOS_QOL=90.2±17.4, P <0.01) (Figure 3). There were no significant differences between groups for the KOOS symptoms, ADL, or Sports subscales. There were no significant differences between no and unilateral PT in all KOOS subscales (Figure 3).DISCUSSION
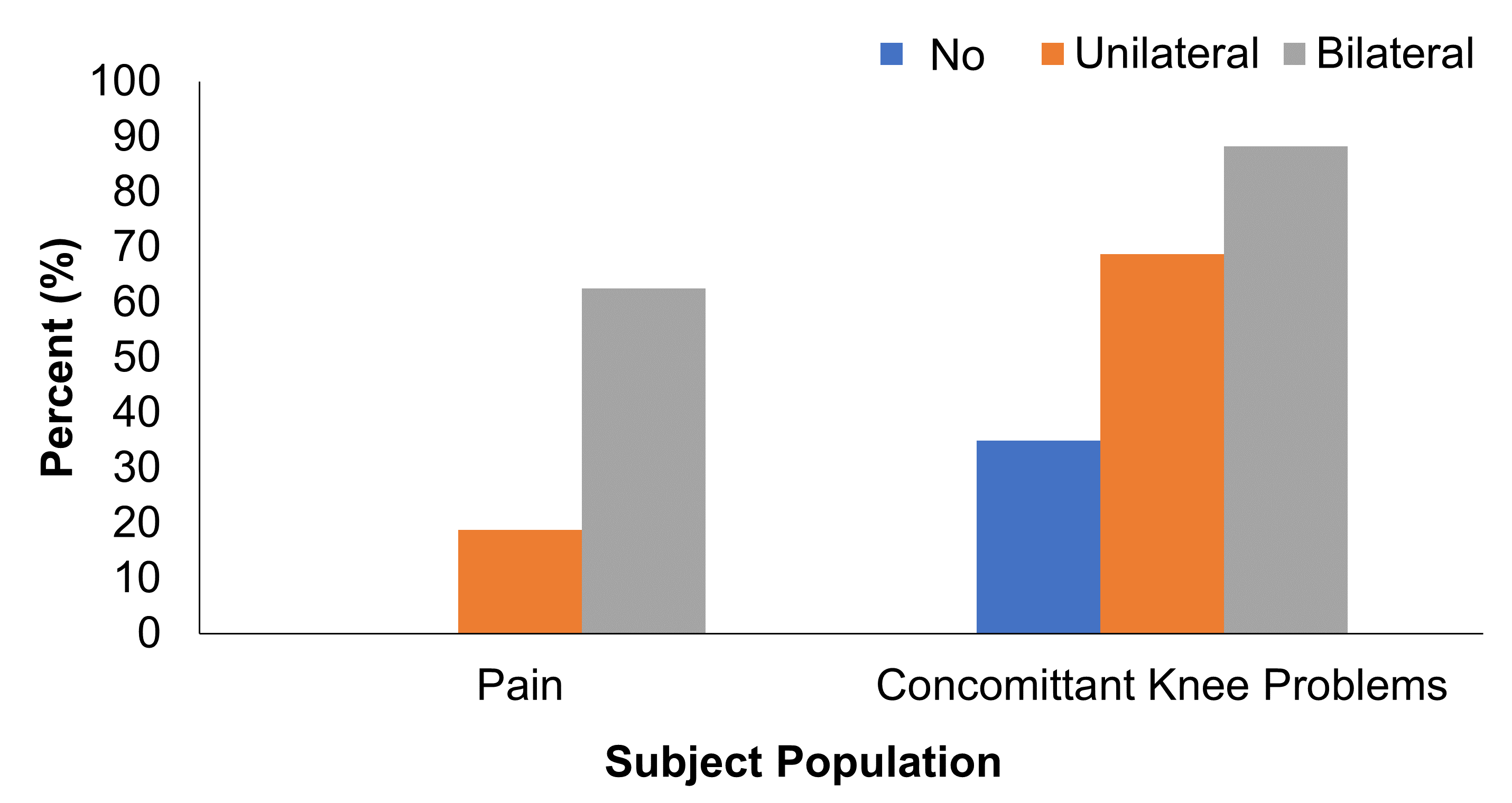
We found that pre-season athletes with MRI signs of bilateral PT have more pain and a reduced QOL than the athletes with no or unilateral PT (Figure 3). Not all athletes with PT reported pain. About 19% of athletes with unilateral PT and 63% of athletes with bilateral PT, respectively, reported significant knee pain (KOOS Pain <897) (Figure 4).Others have suggested PT may not be the primary cause of knee pain5. Our athletes had various concomitant MRI knee findings, with about 35%, 69%, and 88% reporting other knee problems for no, unilateral, and bilateral PT, respectively (Figure 4). Concomitant knee problems such as cartilage damage, edema, and anterior cruciate ligament (ACL) reconstruction were present in all three groups. With bilateral PT athletes reporting increased pain and decreased QOL compared to unilateral and no PT, bilateral PT could be a source of knee pain.
This is a small, preliminary study with classification of PT based on presence of signal intensity of the patellar tendon on a 2D PD FSE with fat saturation. Future work can include a larger study with bone shape, regional T2, and biomechanical analyses between the athletes to investigate more specific risk factors, with the possibility of developing a metric for predicting those who may develop symptomatic PT. Our study population was young and just beginning their elite athletic careers as D1 players. Using MR to identify at-risk athletes may be helpful in prescribing preventive care to keep athletes from further injury since PT is often a long-term and potentially career ending problem.
CONCLUSION
Elite D1 athletes with bilateral PT have more pain and a reduced QOL than athletes with no or unilateral PT, problems that may keep athletes from optimal sport performance. Using MR pre-season to identify at-risk athletes may be helpful in prescribing preventive care to keep athletes from further injury during the season and beyond.Acknowledgements
This work was supported by the NBA, National Institutes of Health (R01EB002524, K24AR062068), GE Healthcare, Canadian Institutes of Health Research, and Wu Tsai Human Performance Alliance. The authors would like to thank Tie Liang for statistical assistance.
References
1. Theodorou A, Komnos G, Hantes M. Patellar tendinopathy: an overview of prevalence, risk factors, screening, diagnosis, treatment and prevention. Archives of Orthopaedic and Trauma Surgery. 2023; 143:6695–6705.
2. Malliaras P, Cook J, Purdam C, Rio E. Patellar tendinopathy: clinical diagnosis, load management, and advice for challenging case presentations. Journal of Orthopaedic & Sports Physical Therapy. 2015; 45(11):888-898.
3. Lian OB, Engebretsen L, Bahr R. Prevalence of jumper’s knee among elite athletes from different sports: a cross-sectional study. Am J Sports Med. 2005;33(4):561-567.
4. Toppi J, Fairley J, Cicuttini FM, et al. Factors associated with magnetic resonance imaging defined patellar tendinopathy in community-based middle-aged women: a prospective cohort study. BMC Musculoskeletal Disorders. 2015; 16:184.
5. Hannington M, Tait T, Docking S, et al. Prevalence and Pain Distribution of Anterior Knee Pain in Collegiate Basketball Players. Journal of Athletic Training. 2022;57(4):319–324.
6. Roos EM and Lohmander LS. The Knee injury and Osteoarthritis Outcome Score (KOOS): from joint injury to osteoarthritis. Health and Quality of Life Outcomes. 2003; 1:64.
7. Muller B, Yabroudi MA, Lynch A, et al. Defining Thresholds for the Patient Acceptable Symptom State for the IKDC Subjective Knee Form and KOOS for Patients Who Underwent ACL Reconstruction. Am J Sports Med. 2016; 44:2820-2826.
Figures
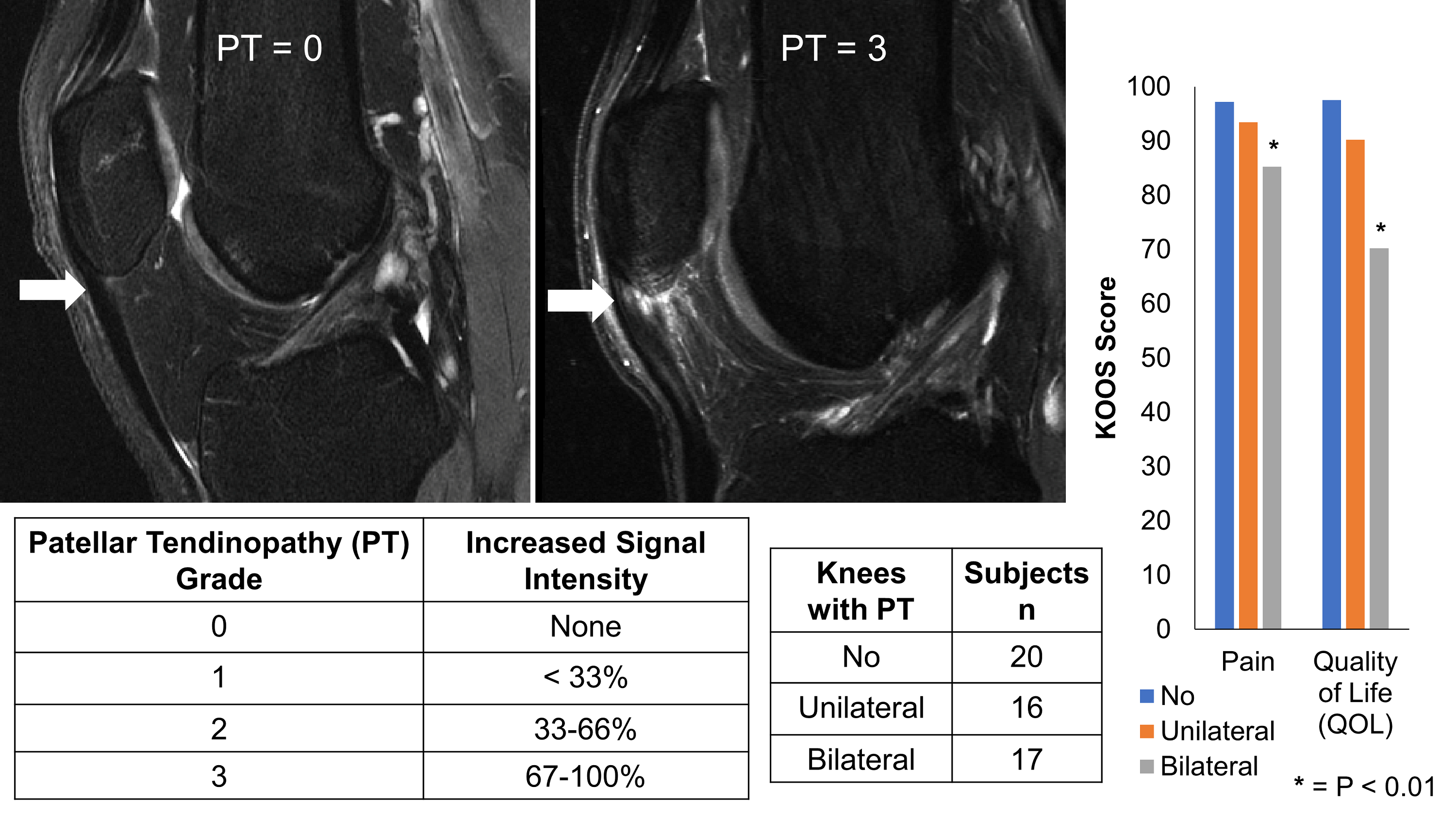
Figure 1: Patellar tendinopathy (PT), as graded by a radiologist, on a scale of 0-3, based on increased high-signal percentage of the axial cross-sectional tendon width. Athletes were stratified into bilateral, unilateral, or no PT. Athletes with bilateral PT had significantly more pain and reduced quality of life (QOL) than those with no or unilateral PT (P <0.01).