1691
Differentiating Between Malignant and Benign Bone Tumors: Combined Diagnostic Value of DWI, IVIM and DKI1The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China, 2Clinical & Technical Support, Philips Healthcare, Beijing, 100102, China, Beijing, China
Synopsis
Keywords: Other Musculoskeletal, Tumor
Motivation: The integration of various diffusion models can yield more precise insights into tumor diffusion and perfusion.
Goal(s): To investigate the utility of combining DWI, IVIM and DKI in the differential diagnosis of benign and malignant bone tumors.
Approach: Six parameters derived from three diffusion models of 107 patients were statistically compared through either the independent samples t-test or Mann-Whitney U test. Diagnostic performance was assessed using ROC curves for both individual examinations and their combined analysis in distinguishing between benign and malignant tumors.
Results: The combination of ADC, D, D*, MK, and MD values had better diagnostic efficacy than these parameters alone.
Impact: Statistically significant differences were observed in the values of ADC, D, D*, MD, and MK between benign and malignant bone tumors. Furthermore, the combination of ADC, D, D*, MK, and MD values had better diagnostic efficacy than these parameters alone.
Introduction
Despite being among the rarest cancer types, malignant bone tumors present a significant threat to human health due to their elevated mortality, disability, and metastasis rates. DWI captures biological information and quantify the dispersion of water molecules within tissue. Nonetheless, due to the intricate cellular microstructural barriers within tumors, water diffusion within tumors can be complex. Intravoxel Incoherent Motion (IVIM) is a bi-exponential model that concurrently reflects genuine water molecule diffusion within tissue and microvascular perfusion. This reveals the intricate microstructural properties of tumor tissue. Diffusion kurtosis imaging (DKI) can quantitively estimate the skewed distribution of water diffusion through a non-Gaussian distribution model which were more sensitive to heterogeneous and irregular tumor intracellular environments[1]. The objective of this study is to investigate the utility of combining DWI, IVIM and DKI in the differential diagnosis of benign and malignant bone tumors.Methods
107 bone tumor patients (70 males and 37 females, age ranged from 7 to 73 years) including 41 benign and 66 malignant cases diagnosed based on pathological biopsy were included in this study. MR imaging was performed on a 3.0-T clinical scanner (Ingenia CX, Philips Healthcare, Best, the Netherlands) with an eighteen-channel phased-array coil. All patients underwent STIR, DWI, IVIM (b=0、10、30、50、75、100、150、300、500、800、1000、1500s/mm2, NEX=4) and DKI (b=0、800、1500s/mm2, diffusion gradient directions=15) MRI. Considering the heterogeneity of the tumor, the radiologist manually defined the region of interest (ROI) of the tumor contour based on DWI images of the largest plane of the tumor. The ROI was then automatically replicated to other parameter maps, including apparent diffusion coefficient (ADC) for DWI, pseudo-diffusion (D*), perfusion fraction (f) and diffusion coefficient (D) for IVIM, and mean diffusion coefficient (MD) and mean kurtosis (MK) for DKI. These parameters were compared using either the independent samples t-test or Mann-Whitney U test according to whether the data follows a normal distribution. Pathological diagnosis served as the standard for our analysis. Additionally, Receiver Operating Characteristic (ROC) curves were generated to assess the combined discrimination of benign and malignant bone tumors. A P value < 0.05 was considered statistically significant.Results
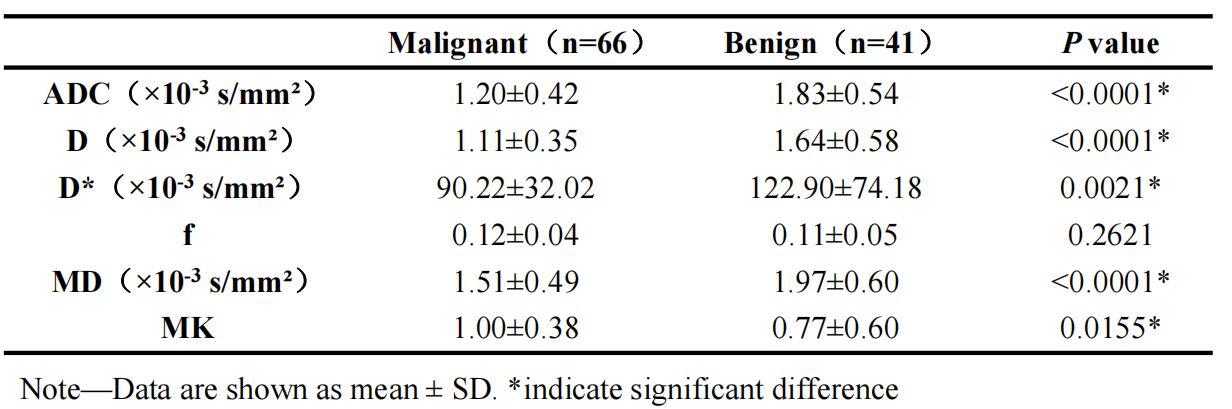
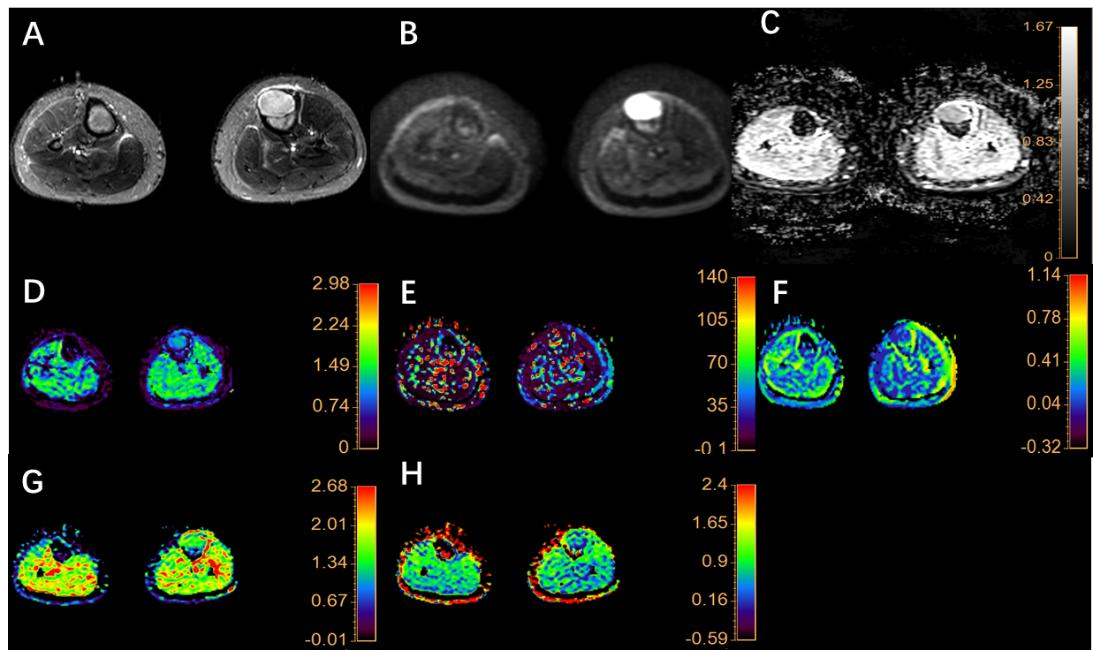
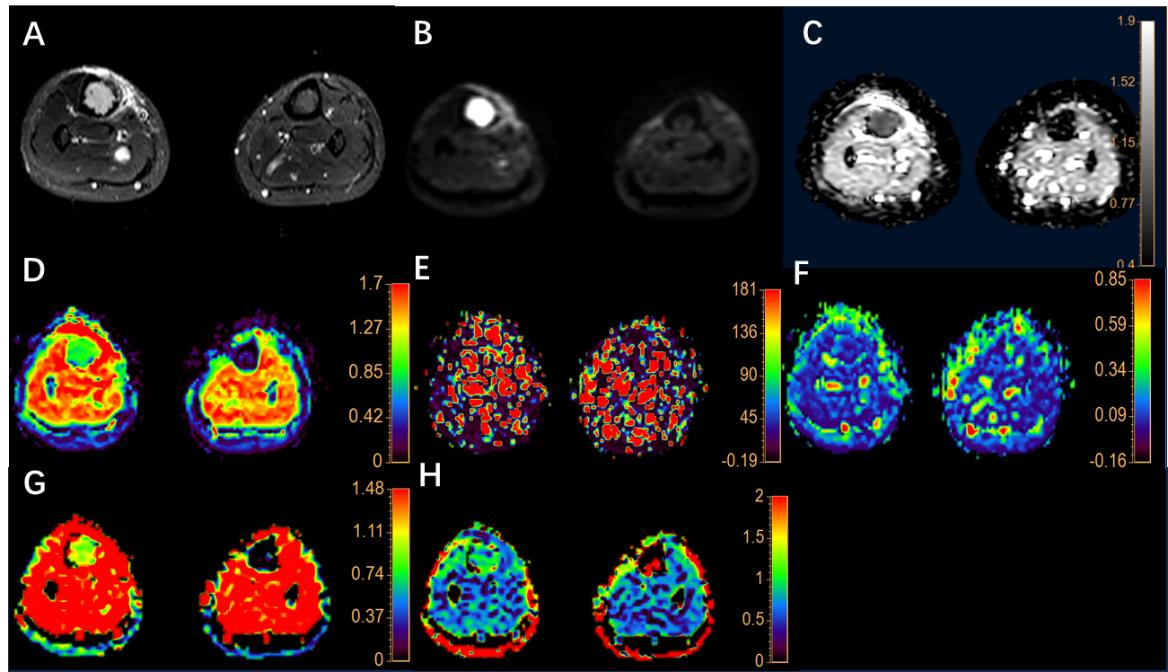
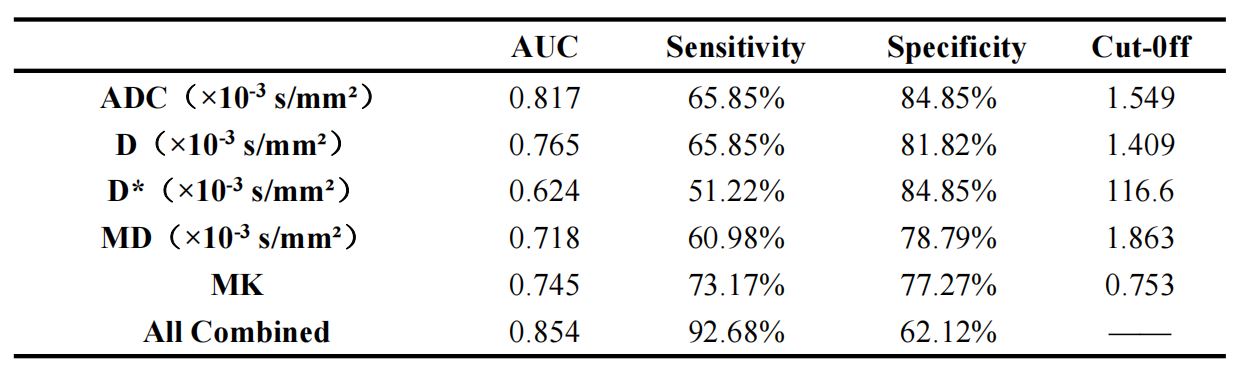
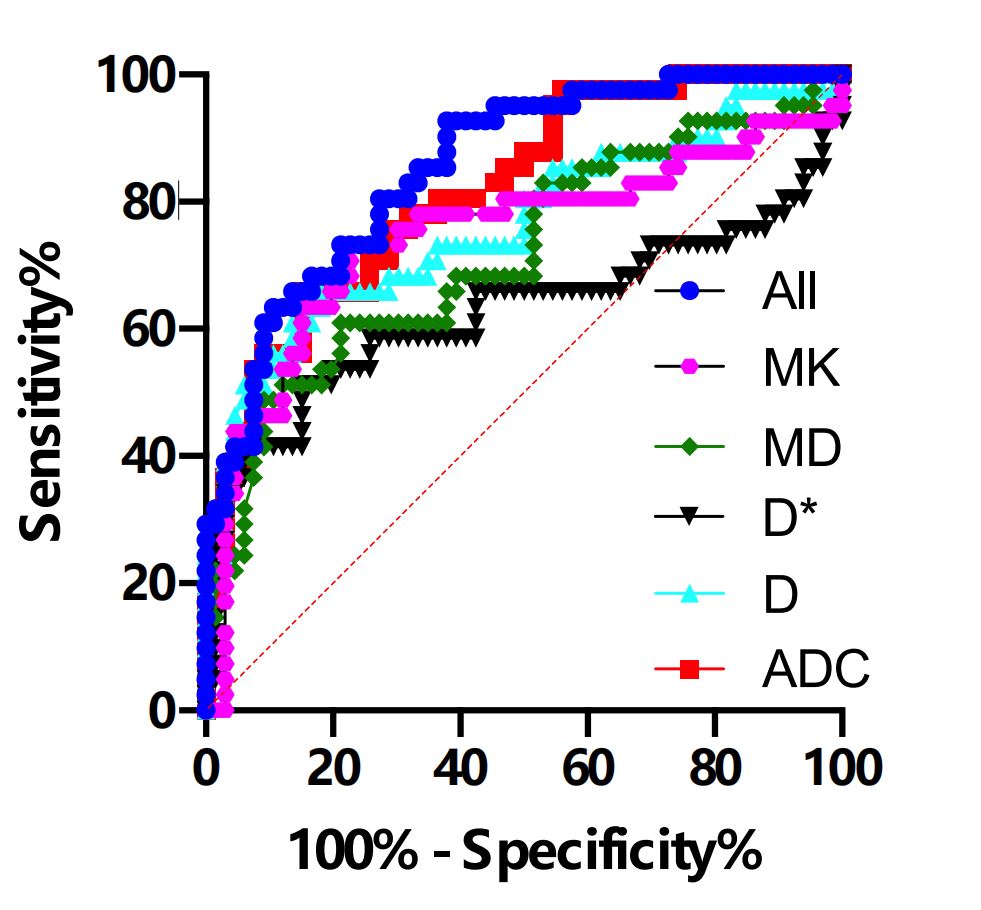
The ADC, D, D* and MD of malignant bone tumors exhibited lower values compared to benign tumors, whereas the f and MK values were marginally elevated. Statistically significant differences were observed in the values of ADC, D, D*, MD, and MK between benign and malignant bone tumors (Table 1). The representative images were shown in Figure 1 and 2. ROC analysis demonstrated that the area under the curve (AUC) for ADC, D, D*, MK, and MD in distinguishing between benign and malignant bone tumors was 0.817, 0.765, 0.624, 0.745, and 0.718, respectively. The integrative analysis combining D, D*, MK, MD, and ADC values enhanced the diagnostic accuracy, yielding an AUC of 0.854, sensitivity 92.68% and specificity 62.12%(Table 2 and Figure 3).Discussion
The utility of D* and f for diagnosis has been contentious in prior research[2]. The variance observed in the f within this study may stem from the substantial number of malignant bone tumors, the diversity of their pathological types, the uneven distribution, and the marked disparities in the vascular architecture among tumors of differing malignancies[3]. Combining multi-diffusion models yields a higher diagnostic efficacy than any single one. Such an integrative approach more accurately captures the nuances of true diffusion dynamics and the intricate water molecule movement within biological tissues, offering a detailed representation of the tumor microstructure's complexity and its subtle alterations[4].Conclusions
In this study, statistically significant differences were observed in the values of ADC, D, D*, MD, and MK between benign and malignant bone tumors. Furthermore, the combination of ADC, D, D*, MK, and MD values had better diagnostic efficacy than these parameters alone.Acknowledgements
No acknowledgement found.References
[1] Le Bihan D, Iima M. Diffusion Magnetic Resonance Imaging: What Water Tells Us about Biological Tissues. PLoS Biol ,2015, 13(7): e1002203.
[2] Polverari G, Ceci F, Bertaglia V, et al. 18 F-FDG pet parameters and radiomics features analysis in advanced NSCLC treated with immunotherapy as predictors of therapy response and survival[J]. Cancers, 2020, 12(5): 1163.
[3] Suzuki A, Maeda T, Baba Y, et al. Acidic extracellular pH promotes epithelial mesenchymal transition in Lewis lung carcinoma model[J].Cancer Cell Int, 2014, 14(1): 129.
[4] Sevtap Arslan, Fatma Bilge Ergen, Güzide Burça Aydın, et al. Different Attenuation Models of Diffusion-Weighted MR Imaging for the Differentiation of Benign and Malignant Musculoskeletal Tumors[J].J Magn Reson Imaging,2022,55(2):594-607.
Figures