1689
Rapid MRI Protocol for Pediatric MSK Infections: Can We Safely Remove Contrast and Sedation?1Northwestern University Feinberg School of Medicine, Chicago, IL, United States, 2Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, IL, United States
Synopsis
Keywords: Whole Joint, Infection
Motivation: Magnetic resonance imaging (MRI) is the gold standard for diagnosis of acute pediatric musculoskeletal infection. However, there are several barriers in the pediatric population, namely poor efficiency of image acquisition.
Goal(s): The present study evaluates physician perspectives on a novel rapid MRI protocol for capturing rapid, non-contrast, limited sequence protocol that has been shown to greatly decrease sedation, scan time, hospital length of stay, and charges without missing actionable diagnoses.
Approach: We administered a series of traditional and rapid protocol cases and associated quiz to six providers.
Results: We found similar success rates of diagnoses and physician confidence between rapid and traditional sequences.
Impact: Our study shows that rapid MRI protocols can be adopted without impeding diagnostic accuracy or reducing the confidence of readers.
Acute musculoskeletal infection (MSKI), including osteomyelitis, septic arthritis, and myositis, is a common medical emergency that affects an estimated 1 in 5,000 children in their lifetime [1]. Early diagnosis and treatment are crucial for preventing adverse sequelae. Though MRI is the preferred diagnostic tool for acute MSKI, there are several challenges in the pediatric population that can lead to delays in care. To improve the efficiency of MRI acquisition, we developed a rapid, non-contrast, limited sequence protocol that was previously shown to greatly decrease sedation, scan time, hospital length of stay, and charges without missing actionable diagnoses. The present study aimed to evaluate provider perspectives on the rapid MRI protocol by administering a series of cases and associated questionnaire to six providers.
Methods:
In a previous study, we described a new rapid MRI protocol that acquires fluid-sensitive sequences and diffusion with avoidance of sedation and contrast administration. This protocol was limited for use in suspected infections of the extremities and pelvis. Initially, our protocol uses a large field-of-view (FOV) single-shot fast spin echo sequence to identify the anatomic area of interest. Then, small, focused FOV images of the area are acquired, including axial, sagittal, and coronal T2-weighted fat-suppressed (T2FS) images, a coronal T1-weighted sequence, and axial diffusion-weighted imaging (DWI) with an accompanying ADC (apparent diffusion coefficient) map. This protocol is now standard of care at our large, tertiary academic children’s hospital.
In the present study, we selected 48 cases of possible acute pediatric MSKI, with 25 being captured using the rapid protocol and 23 with traditional, pre- and post-contrast sequences. There were 22 infections in the rapid protocol (17 osteomyelitis) and 18 (13 osteomyelitis) in the traditional cohort. Six readers were recruited for this study: two attending pediatric radiologists, one MSK radiology fellow, two attending pediatric orthopaedic surgeons, and one pediatric orthopaedic surgery fellow. For each case, readers were asked whether the following were present: 1) any infection, 2) osteomyelitis, 3) soft tissue abscesses, 4) subperiosteal abscesses, 5) intraosseous abscesses, and 6) pathologic joint effusion. Additionally, there were asked to rate their confidence for each factor on a scale of 1 to 3. A score of 1 indicated “not confident”, 2 was “moderately confident,” and 3 reflected being “very confident.” Responses for the rapid and traditional cohort were compared using chi-squared and unpaired, two-sample T tests, with significance at P < 0.05.
Results:
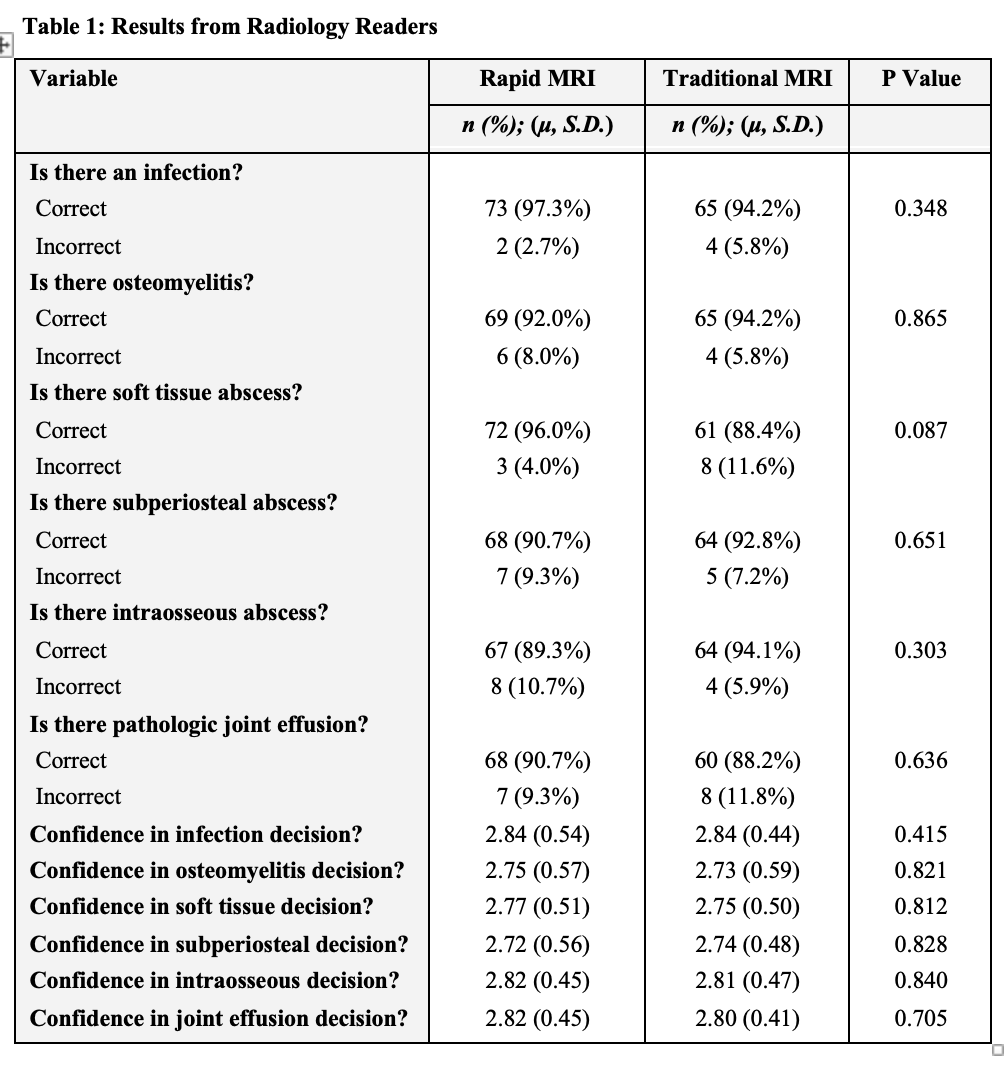
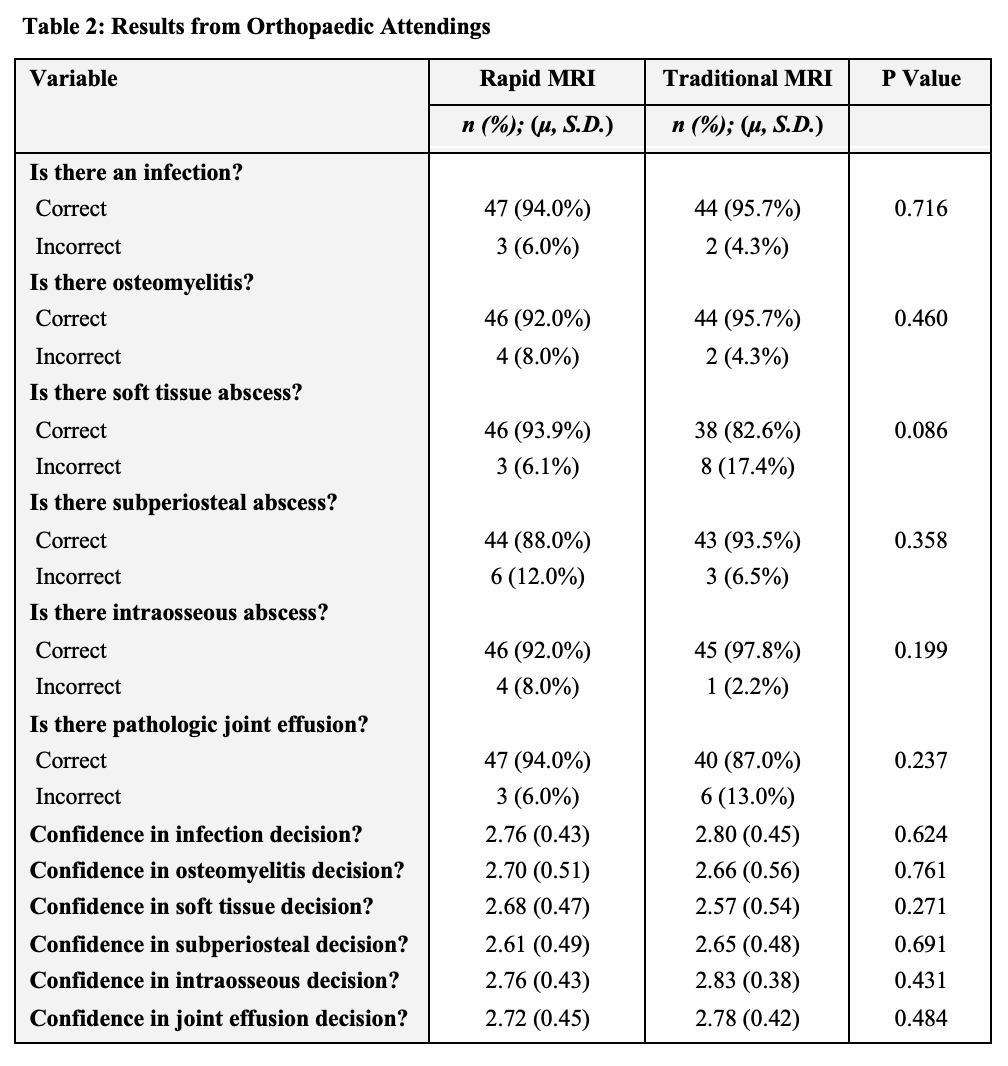
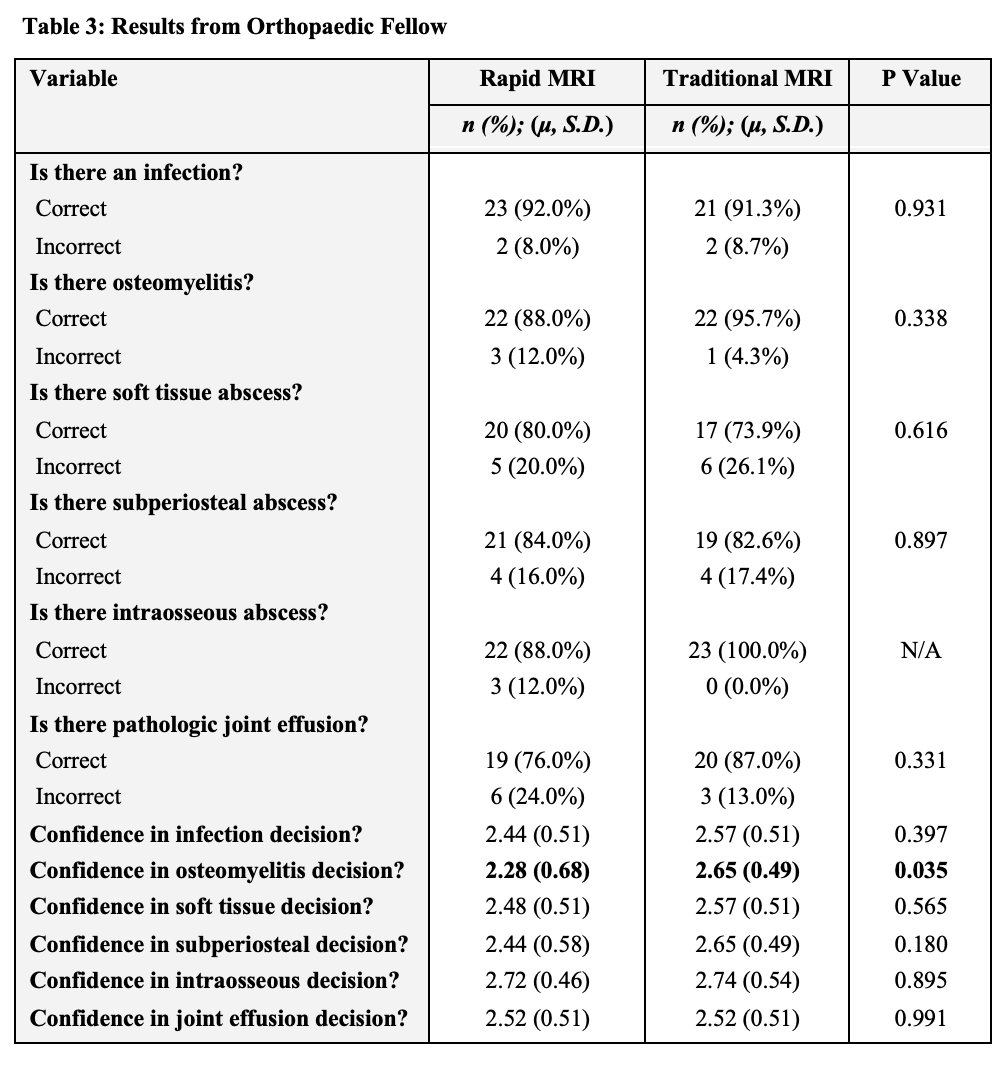
A total of 48 cases were included in our study. When comparing the 75 total rapid and 69 traditional cases reviewed by radiologist readers, there was no difference in the accuracy of diagnosing infection (97.3% vs. 94.2%; P = 348), osteomyelitis (92.0% vs. 94.2%; P = 0.865), soft tissue abscess (96.0% vs. 88.4%; P = 0.087), subperiosteal abscess (90.7% vs. 92.8%; P = 0.651), intraosseous abscess (89.3% vs. 94.1%; P = 0.303), or pathologic joint effusion (90.7% vs. 88.2%; P = 0.636). Additionally, there was no difference in reader confidence for any outcome, with all P > 0.05 (Table 1). In two attending pediatric orthopedists, there was similarly no difference in the accuracies of any outcome or associated confidence, with all P > 0.05 (Table 2). As shown in Table 3, there was decreased confidence with the rapid protocol in osteomyelitis decisions for the orthopaedic fellow (2.28 vs. 2.65; P = 0.035); however, there was no significant difference in accuracy (88.0% vs. 95.7%; P = 0.338).
Discussion:
The rapid MRI protocol preserves diagnostic accuracy and does not lead to decreased physician confidence in radiology attendings, pediatric orthopedic attendings, and MSK radiology fellows. Though there may be an initial learning curve to adopting the rapid MRI protocol, our study suggests that similar diagnostic confidence can be achieved.
Acknowledgements
No acknowledgement found.References
[1] De Boeck H. Osteomyelitis and septic arthritis in children. Acta Orthop Belg. 2005;71(5):505-515.Figures