1686
An MRI-based radiomics method combined with clinic-radiological characteristics for the prediction of survival in aggressive spinal tumor1Peking University Third Hospital, Beijing, China, 2University of California, Irvine, CA, United States, 3Radiology, Affiliated Hospital of Qingdao University, Qingdao, China
Synopsis
Keywords: Bone, Skeletal
Motivation: Treatment options for spinal tumors are challenging.
Goal(s): To predict the progression-free survival (PFS) of aggressive spinal tumors based on MRI combined with clinical features to aid early personalized treatment decisions.
Approach: Clinical, pathological and imaging data of 211 patients underwent spinal tumor surgery at two research centers were retrospectively analyzed. Tumoral and peritumoral features were extracted from T1WI and T2WI images. Clinical-radiomics nomogram was developed by radiomics signatures and the predictive clinical parameters.
Results: The integrative model showed best performance in PFS evaluation for the prediction of postoperative PFS, with the AUC was 0.86 and 0.81 in the training and test cohort.
Impact: Rad-score is an independent factor for PFS after resection for spinal tumor. The nomogram established in this study could be an effective tool for the clinical prediction of PFS after surgery.
INTRODUCTION
Spinal neoplasms have a wide range of aggressiveness, from benign lesions to highly invasive malignancies1. Treatment options for spinal tumors are challenging. Due to the heterogeneity of spinal tumors and the surrounding complex and important anatomical structures, how to balance the quality of life and reducing the recurrence rate after surgery often makes clinicians in a dilemma2,3. Assessing clinical and imaging features to explore prognostic factors may help surgeons with early personalized treatment decisions, but has not been fully explored.PURPOSE
To predict the progression-free survival (PFS) of aggressive spinal tumors based on MRI combined with clinical features to aid early personalized treatment decisions.METHODS
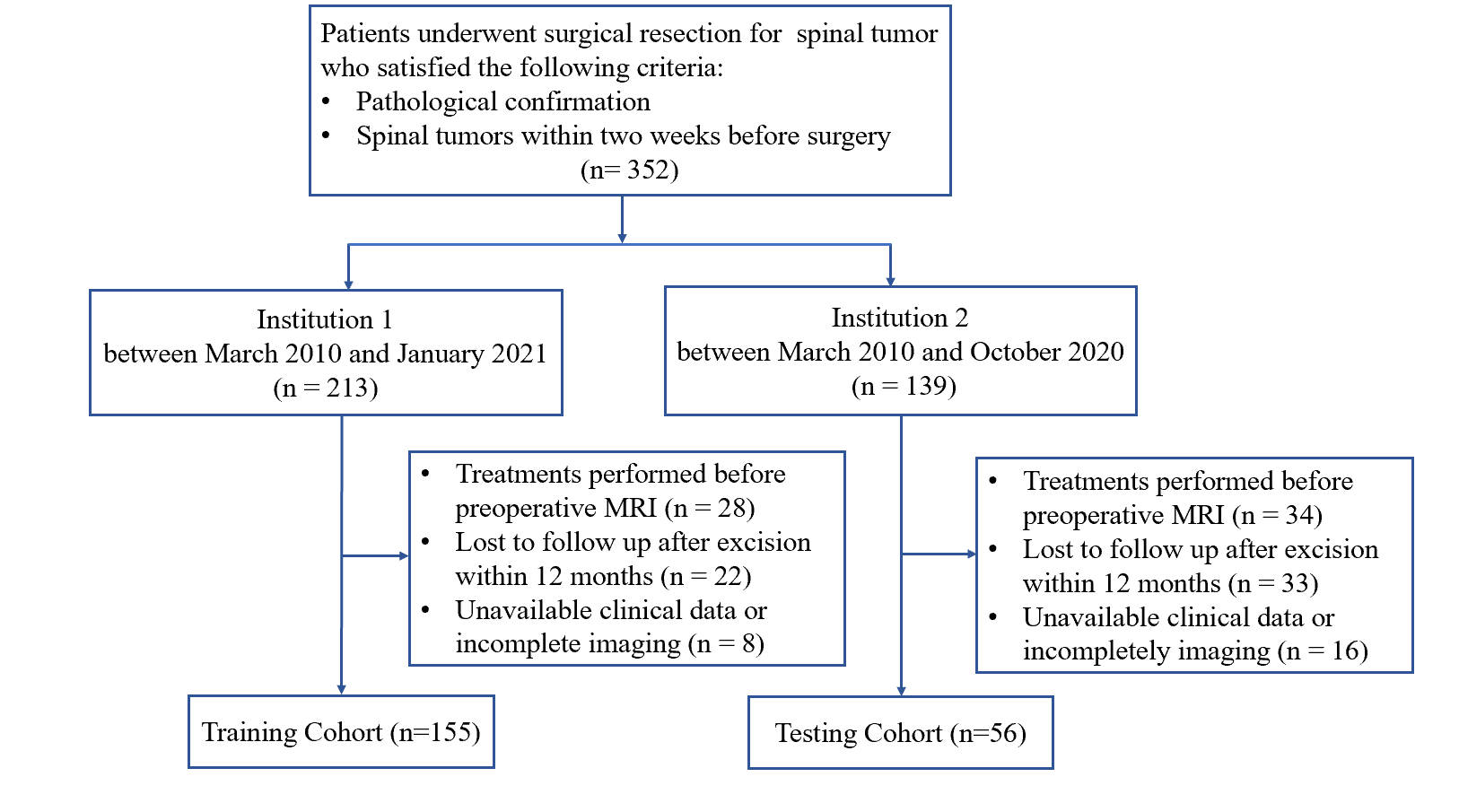
- Data of patients diagnosed with spinal tumor and underwent the initial surgery from two separate hospitals with confirmed pathological diagnosis between March 2010 and January 2021 were retrospectively collected: a training set from the Peking University Third Hospital (n = 155), and an external test set from the Affiliated Hospital of Qingdao University (n = 56). Data from the training set were used to establish the prediction model, and data from the test set were used for external testing. The primary outcome was PFS.
- The inclusion and exclusion criteria are shown in Figure 1.
- Patient baseline clinical characteristics and pathologic data were collected from medical records, including age, sex, tumor type and histology, location, the international classification of diseases 10th revision (ICD-10, https://icd.who.int/browse10/2019/en) grading, surgery method, progression-free survival (PFS) and post-operative recurrence.
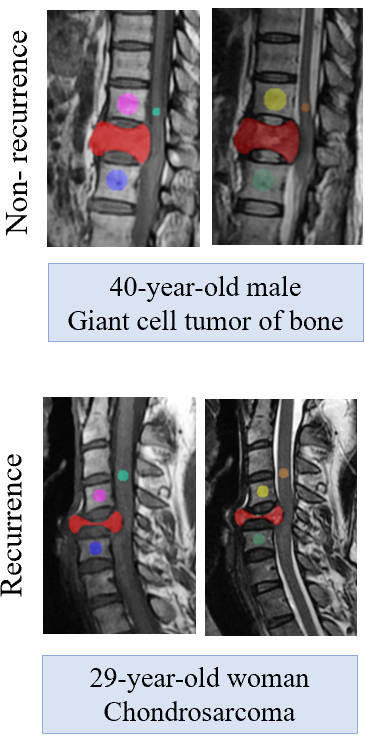
- We used the open-source ITK-SNAP software for lesion segmentation. At the same time, two kinds of ROI were selected for the adjacent normal vertebrae and spinal cord (Figure 2). Tumoral and peritumoral features were extracted separately from T1WI and T2WI images and the least absolute shrinkage and selection operator was used to screen the most valuable radiomics features. Clinical-radiomics nomogram was developed by radiomics signatures and the most predictive clinical parameters. An integrative model was developed for personalized PFS prediction, which combined the radiomics signature, clinical and MRI features, using multivariable Cox regression model. Model performance was evaluated with the C-index. In a bid to achieve a more holistic analysis, this study integrated clinical characteristics with selected radiomics features. This melding of data enabled the construction of the Kaplan-Meier survival model, offering detailed insights into patient survival probabilities over time. Furthermore, leveraging this combined data, a prognostic nomogram was developed. This graphical representation was designed to aid clinicians and researchers in visualizing the interrelation between various factors and predicting potential outcomes. The nomogram, built upon the consolidated radiomics-clinical model, is not just a statistical tool but also a valuable guide for prognosis and future research directions. The prediction model and nomogram were validated in the training and test cohorts.
RESULTS
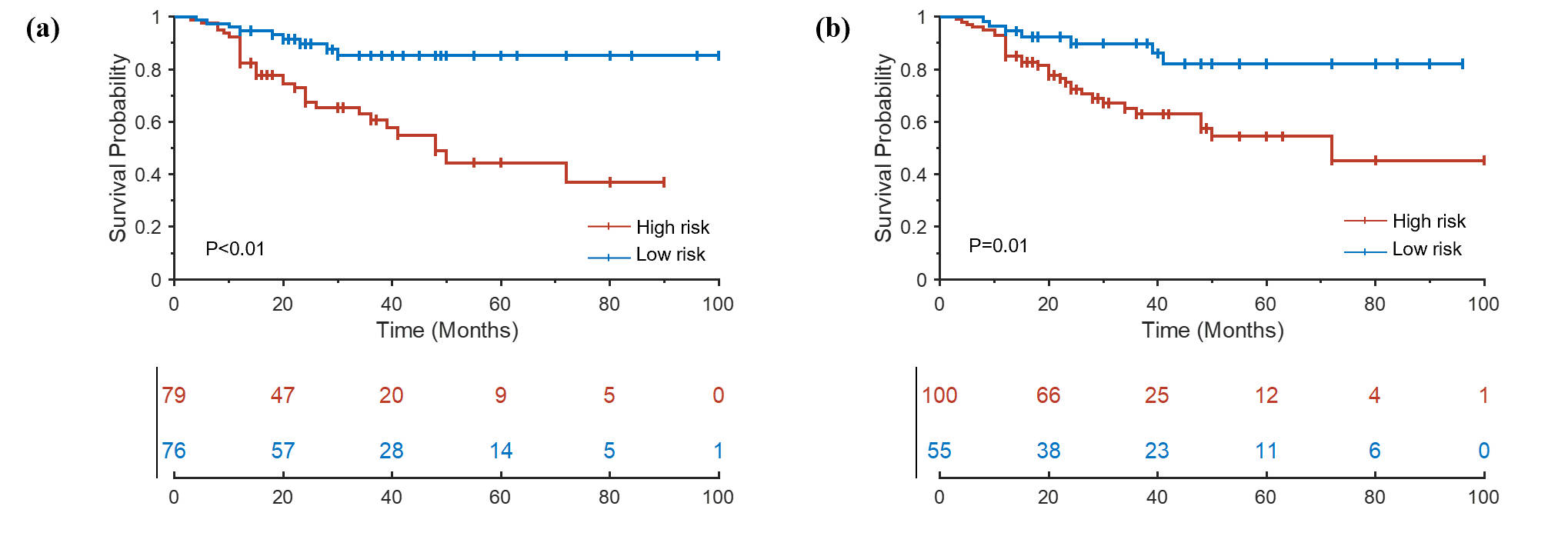
Enneking stage (hazards ratio [HR], 2.66; 95% confidence interval [CI], 1.42–4.52; p < 0.001), vertebral compression (HR, 2.01; 95% CI, 0.67–2.72; p = 0.01), and the international classification of diseases (HR, 1.92; 95% CI, 1.14–2.72; p = 0.02) were identified as significant risk predictors of PFS. The integrative model, which combined radiomics signature and clinical features, showed best performance in PFS evaluation for the prediction of postoperative PFS, with the area under the receiver operating characteristic curve (AUC) was 0.86 and 0.81 in the training and external test cohort, respectively. Kaplan-Meier survival analysis (Figure 3) showed combined model (p < 0.01) and tumoral radiomics model (p = 0.01) were independent risk factors for PFS.DISCUSSION
Our study has several limitations. Since this study required all subjects to be patients with primary spinal tumors undergoing surgical treatment, the sample size was still relatively small despite involving two centers. Multi-center data for model validation and refinement is important. Secondly, some molecular biomarkers have been used to predict the prognosis of some tumors, but were not included in this study. The main reason is that there is no consensus and no routine clinical testing. Adding molecular pathology may be an important extension of radiomics. Third, the ROI of spinal tumor has to be contoured manually due to the complexity of adjacent anatomy, which is labor-consuming. In the future, appropriate automatic segmentation techniques for the treatment of spinal tumors are promising, optimizing the end-to-end diagnosis-treatment-follow-up chain.CONCLUSION
Rad-score is an independent factor for PFS after resection for spinal tumor. The nomogram established in this study could be an effective tool for the clinical prediction of PFS after surgery.Acknowledgements
We are grateful to Nan Li (Research Center of Clinical Epidemiology, Peking University Third Hospital) for comments and suggestions.References
1. Sundaresan N, Rosen G, Boriani S. Primary malignant tumors of the spine. Orthop Clin North Am. 2009;40(1):21-36, v.
2. Melcher I, Disch A C, Khodadadyan-Klostermann C, et al. Primary malignant bone tumors and solitary metastases of the thoracolumbar spine: results by management with total en bloc spondylectomy. Eur Spine J. 2007;16(8):1193-1202.
3. Sciubba D M, De la Garza Ramos R, Goodwin C R, et al. Total en bloc spondylectomy for locally aggressive and primary malignant tumors of the lumbar spine. Eur Spine J. 2016;25(12):4080-4087.
Figures