1685
Deep Learning-based Automatic Segmentation and Fusion Radiomics-based Prediction of Response to Neoadjuvant Chemotherapy for Osteosarcoma1Peking University people’ hospital, Beijing, China
Synopsis
Keywords: Bone, Tumor, Neoadjuvant chemotherapy · Response prediction
Motivation: The efficacy of neoadjuvant chemotherapy (NAC) directly affects the clinical treatment of osteosarcoma (OS) patients. Consequently, it is essential to accurately assess the effectiveness of NAC.
Goal(s): To develop an automated method for accurately segmenting tumors and predicting the response to NAC in OS patients from conventional sequences of preoperative MRI.
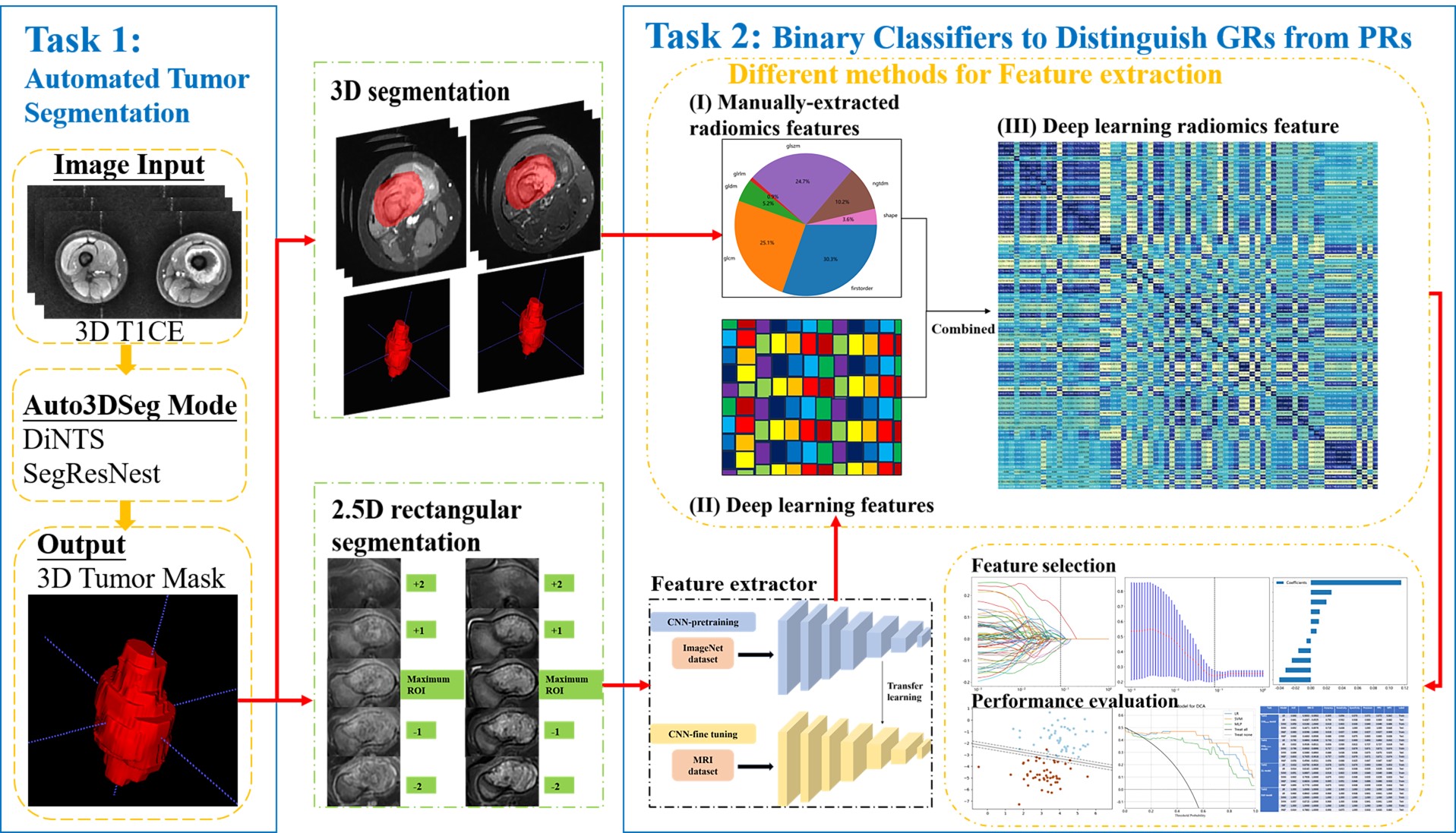
Approach: In the present study, we accomplished two tasks. One involves constructing a deep learning model for automatic tumor segmentation, while the other entails predicting the response to NAC using different feature extraction methods in OS patients.
Results: Radiomics models can serve as a non-invasive tool for predicting treatment response in OS.
Impact: Radiomics have the potential to non-invasively predict the neoadjuvant chemotherapeutic responses. This tool could significantly contribute to avoiding ineffective chemotherapy and optimizing the management of OS patients in the era of personalized medicine.
INTRODUCTION
Osteosarcoma (OS) is the predominant primary bone malignancy and accounts for over 44% of all primary malignant bone tumors [1]. Chemotherapy-induced necrosis in OS is widely acknowledged as a prominent prognostic factor [2]. Not all patients with OS benefit from the current therapeutic regimen, which includes preoperative neoadjuvant chemotherapy (NAC), surgery and postoperative treatment [3], specifically those who exhibit inadequate response to NAC [4, 5]. Consequently, it is essential to accurately assess the effectiveness of NAC. The potential of radiomics in aiding therapeutic planning and evaluation is promising [6, 7]. The aim of this study was to develop an automated method for accurately segmenting tumors and predicting the response to NAC in OS patients from conventional sequences of preoperative MRI examinations using a machine learning approach.METHODS
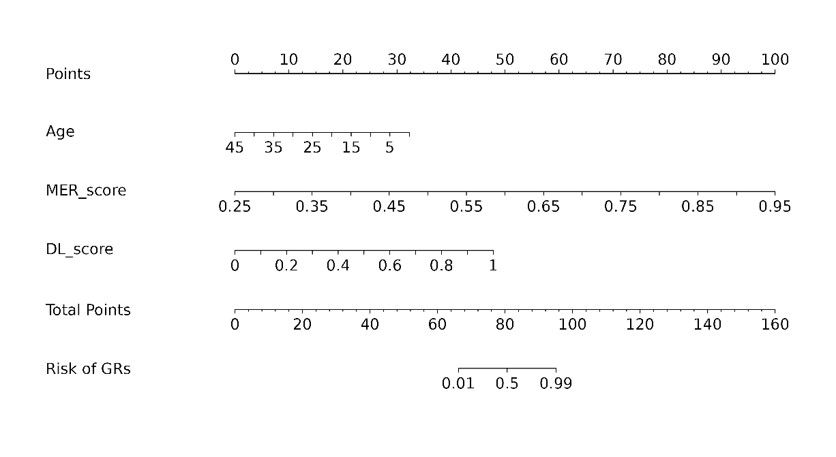
We reviewed axial T2-weighted imaging (T2WI) and contrast-enhanced T1-weighted (T1CE) of 106 patients pathologically confirmed as OS. Our study involved two tasks: (I) the utilization of the Auto3DSeg framework for automated OS segmentation, and (II) based on three feature extraction methods, incorporating manually extracted radiomics (MER) features, deep learning (DL) features based on ResNet18 and fusion features, nine risk classification models were constructed using three classifiers: Logistic Regression (LR), Support Vector Machine (SVM) and Multi-Layer Perceptron (MLP). Specifically, we utilized a cohort of 83 patients to train the automatic segmentation model, which was subsequently employed to segment an additional 23 patients. The evaluation of the model's performance was conducted using the dice coefficient in task 1. The area under the receiver operating curve (AUC), sensitivity, specificity, accuracy, negative predictive value (NPV) and positive predictive value (PPV) were calculated for performance evaluation in task 2. Additionally, we developed a deep learning radiomics nomogram (DLRN) by combining the best MER labels, the best DL labels with clinical indicators.RESULTS
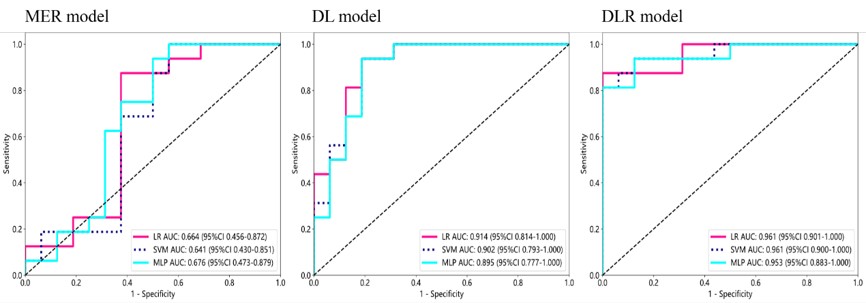
In the task1, the automatic segmentation models (DiNTS and SegResNest) were trained for 116 and 750 epochs and achieved Dice coefficients of 0.771 and 0.845 in a dataset of 83 patientst, respectively. The SegResNest, which achieved the higher Dice coefficient, underwent reassessment and achieved a Dice coefficient of 0.868 in a dataset comprising 106 patients.In the task2, the MLP classifier achieved the highest AUC values of 0.943 and 0.676 on the training and test cohorts in the MER model. As for performance of the DL model, the LR classifier outperformed both SVM and MLP classifier in the validation set, with an AUC of 0.914, accuracy of 0.875, sensitivity of 0.812, specificity of 0.938, precision of 0.929, PPV of 0.929 and NPV of 0.833. In the DLR model, the LR classifier demonstrated the highest classification performance, achieving an AUC of 0.961 and accuracy of 0.938 in the validation cohort.
DISCUSSION
In our study, three models, namely the MER, the DL and the DLR models, were developed based on the T2WI and T1CE sequences, and their performances were compared. The DLR model demonstrated superior performance compared to both the MER model and the DL model. We hypothesize that combining MER with DL radiomics can enhance the extraction of valuable information from conventional MRI brain images and improve prediction results, in line with previous studies27. In conclusion, our findings suggest that radiomics have the potential to non-invasively predict the neoadjuvant chemotherapeutic responses.Our study expands the work of several recent studies that have focused on prediction of the response of NAC in OS patients. Zhang et al. developed and evaluated three classifiers, that is KNN, SVM and LR, to estimate neoadjuvant chemotherapeutic responses in 102 individuals with OS using T1CE data. The three classifiers achieved AUCs of 0.86, 0.92 and 0.93, respectively [8]. Zhong et al. devised a pipeline for the automatic segmentation of the ROI and employed a nomogram that combined the MRI-based radiomics score with clinical variables to forecast neoadjuvant chemotherapeutic responses in 144 patients with OS using T2WI data. The segmentation model, trained using nnU-Net, attained a Dice coefficient of 0.869, while the clinical-radiomics nomogram yielded an AUC of 0.793 and an accuracy of 79.1% [9]. In our study, we expanded the analysis to incorporate two sequences and conducted comprehensive radiomic analyses on the MER model, the DL models and the DLR models. This distinguishes our study from a previous one that solely relied on one kind model, especially classical ML model.
CONCLUSION
In conclusion, our findings suggest that radiomics, especially fusion radiomics, can accurately predict the response to NAC in patients diagnosed with OS. Radiomics could greatly assist in avoiding ineffective chemotherapy and optimizing the management of OS patients in the era of personalized medicine.Acknowledgements
The authors have no relevant financial or non-financial interests to disclose.
References
[1] Choi, J.H. & Ro, J.Y. The 2020 WHO Classification of Tumors of Soft Tissue: Selected Changes and New Entities. Adv Anat Pathol 28, 44-58 (2021).
[2] Saeter, G., et al. Systemic relapse of patients with osteogenic sarcoma. Prognostic factors for long term survival. Cancer 75, 1084-1093 (1995).
[3] Bielack, S.S., et al. Osteosarcoma and causes of death: A report of 1520 deceased patients from the Cooperative Osteosarcoma Study Group (COSS). Eur J Cancer 176, 50-57 (2022).
[4] Ferrari, S., et al. Neoadjuvant chemotherapy with methotrexate, cisplatin, and doxorubicin with or without ifosfamide in nonmetastatic osteosarcoma of the extremity: an Italian sarcoma group trial ISG/OS-1. J Clin Oncol 30, 2112-2118 (2012).
[5] Bielack, S.S., et al. Methotrexate, Doxorubicin, and Cisplatin (MAP) Plus Maintenance Pegylated Interferon Alfa-2b Versus MAP Alone in Patients With Resectable High-Grade Osteosarcoma and Good Histologic Response to Preoperative MAP: First Results of the EURAMOS-1 Good Response Randomized Controlled Trial. J Clin Oncol 33, 2279-2287 (2015).
[6] Fritz, B., Yi, P.H., Kijowski, R. & Fritz, J. Radiomics and Deep Learning for Disease Detection in Musculoskeletal Radiology: An Overview of Novel MRI- and CT-Based Approaches. Invest Radiol 58, 3-13 (2023).
[7] Beam, A.L., et al. Artificial Intelligence in Medicine. N Engl J Med 388, 1220-1221 (2023).
[8] Zhang, L., et al. Machine Learning-Based Radiomics Nomogram With Dynamic Contrast-Enhanced MRI of the Osteosarcoma for Evaluation of Efficacy of Neoadjuvant Chemotherapy. Front Oncol 11, 758921 (2021).
[9] Zhong, J., et al. Automated prediction of the neoadjuvant chemotherapy response in osteosarcoma with deep learning and an MRI-based radiomics nomogram. Eur Radiol 32, 6196-6206 (2022).
Figures