1683
Preliminary assessment of 3D-APTWI combined with DWI in differentiating benign and malignant bone and soft tissue tumors1The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China, 2Clinical & Technical Support, Philips Healthcare, Beijing, 100102, China, Beijing, China
Synopsis
Keywords: Bone, Tumor
Motivation: Clinical applications of APTWI for differentiating benign and malignant bone and soft tissue tumors are scarce.
Goal(s): This work investigated and evaluated the ability of APT and DWI parameters in distinguishing benign from malignant bone and soft tissue tumors.
Approach: MTRasym and ADC values of ninety-six patients in benign and malignant lesions were compared using either the independent samples t-test or Mann-Whitney U test. The ROC curve was used to assess the diagnostic performance in differentiation between benign and malignant tumors.
Results: APTWI combined with DWI showed a significantly improved differentiation between benign and malignant tumors.
Impact: The combination of APTWI and DWI offers valuable insights into changes in cellular proteins and peptides. When MTRasymmax is combined with ADCmin, it yields superior diagnostic performance for distinguishing between malignant and benign bone and soft tissue tumors.
Introduction
Although bone and soft-tissue tumors are uncommon, early diagnosis and prompt referral to a specialized unit offer the best prospects for successful outcomes, both in terms of survival and surgical resection. Previous studies have demonstrated the utility of amide proton transfer weighted imaging (APTWI) in evaluating glioma grading and distinguishing between benign and malignant pelvic tumors [1-3]. However, the clinical application of APTWI remains limited, and only a few analyses have been conducted to differentiate between benign and malignant bone and soft tissue tumors. This study aims to assess and compare the diagnostic effectiveness of APTWI and conventional diffusion weighted imaging (DWI) in discriminating between benign and malignant tumors.Methods
Ninety-six patients (55 males and 41 females, age ranged from 7 to 82 years) with soft tissue or bone tumors (diagnosed based on pathological biopsy) were included in this study. According to the WHO classification of tumors of soft tissue and bone (2020) criteria, the 96 patients were divided into two groups: 41 with benign tumors and 55 with malignancies. All the patients underwent scanning with APTWI and DWI using a 3T MR scanner (Ingenia CX, Philips Healthcare, Best, the Netherlands). APTWI was acquired using the 3D turbo spin echo sequence. The other parameters were: TR/TE = 6540/8.3 ms; FOV = 230×181 mm2; scan matrix = 116×90; voxel size = 2×2×5 mm3; 9 slices; TSE factor = 174; acquisition time = 6 min. The axial DWI sequence (TR/TE=3700/85ms, NSA=4) was performed with b values of 0 and 800 s/mm², and the corresponding apparent diffusion coefficient (ADC) map was calculated. The magnetization transfer ratio asymmetry at 3.5 ppm [MTRasym (3.5 ppm)] and ADC values for tumors were measured, with the maximum, mean, and minimum values recorded, respectively. MTRasym and ADC values in benign and malignant lesions were compared using either the independent samples t-test or Mann-Whitney U test by SPSS software (version 20.0). A P value < 0.05 was considered statistically significant. Furtherly, the receiver operating characteristic (ROC) curve was used to assess the diagnostic performance of MTRasym and ADC values in differentiation between benign and malignant tumors.Results
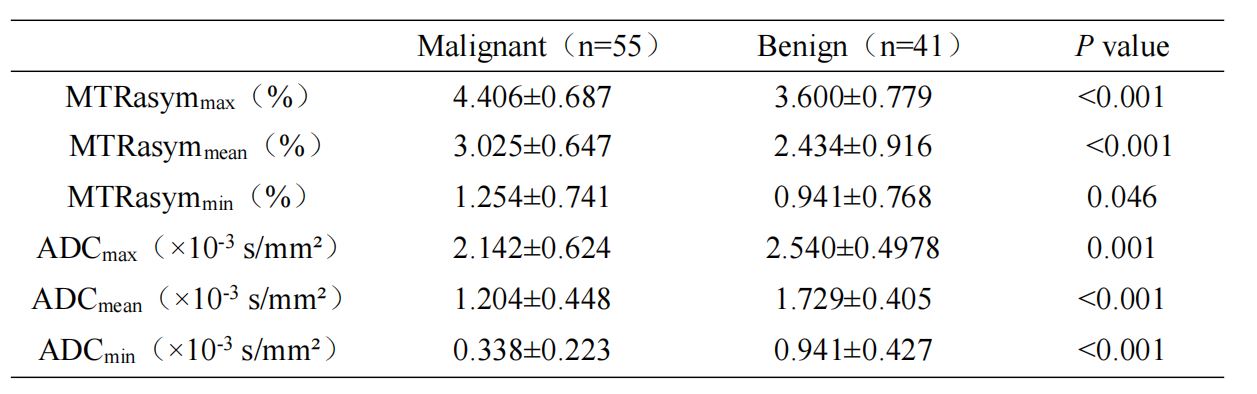
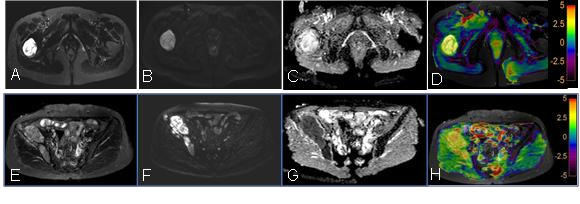
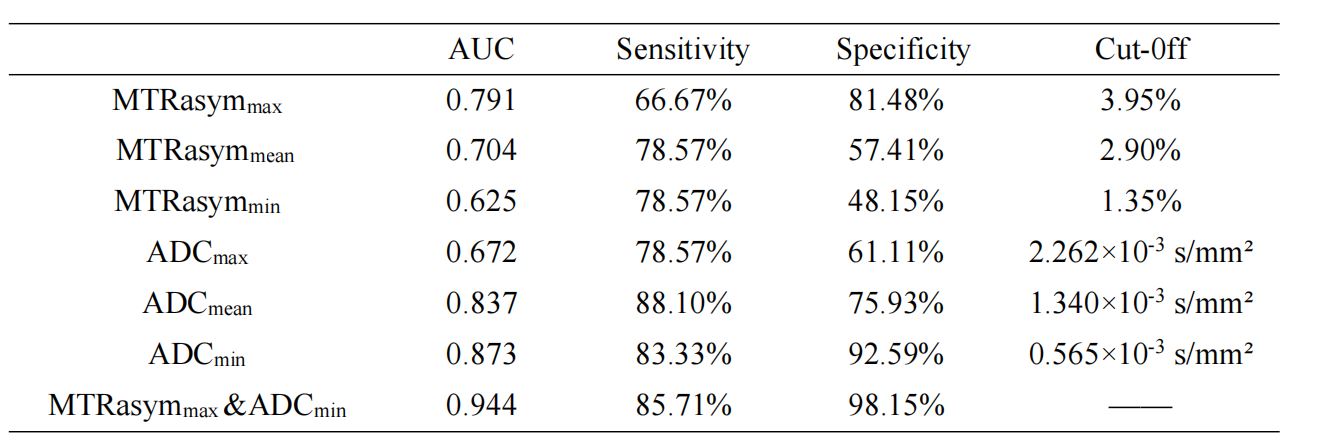
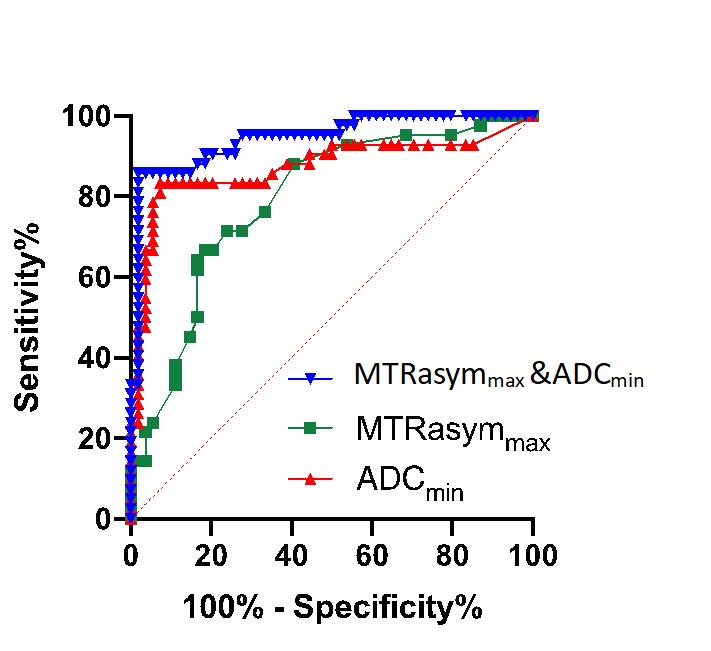
MTRasym(3.5 ppm) values, including MTRasymmax, MTRasymmean and MTRasymmin, exhibited a significant elevation in malignant tumors, while ADC values, including ADCmax, ADCmean and ADCmin, demonstrated a marked decrease (Table 1, Figure 1, Figure 2). ROC analyses revealed that MTRasymmax and ADCmin exhibited the highest diagnostic performance within the APTWI and DWI parameters, respectively, for distinguishing between benign and malignant tumors. Their corresponding Area Under the ROC Curves (AUCs) were 0.791 and 0.873, respectively (Table 2).The combination of MTRasymmax and ADCmin yielded an enhanced diagnostic performance with an AUC of 0.944. There was no significant difference in the AUC between MTRasymmax and ADCmin. When using a cut-off value of 3.95% for MTRasymmax, the sensitivity and specificity for distinguishing benign from malignant bone and soft tissue tumors were 66.67% and 81.48%, respectively. Similarly, employing a cut-off value of 0.565×10-3 mm²/s for ADCmin resulted in a sensitivity and specificity of 83.33% and 92.59%, respectively. Furthermore, the combination of MTRasymmax and ADCmin yielded a sensitivity and specificity of 85.71% and 98.15%, respectively (Figure 3).Discussion
In this study, we initially observed a significant overlap in APT values between benign and malignant lesions. Our findings revealed higher APT signal intensity in malignant tumors compared to benign ones, implying varying concentrations of mobile proteins and peptides within tumors, correlating with their malignancy grade. Additionally, MTRasymmax was found to serve as an indicator of regions within the tumor characterized by the highest local cell density or most active metabolic activity. Conversely, we also noted lower ADC intensities in malignant tumors compared to benign tumors. This observation aligns with findings from previous studies, which have established a correlation between ADC values and tumor grade, indicating their capacity to reflect tumor cellularity and water content within the interstitial space [4]. And the diagnostic potential of DWI in distinguishing between benign and malignant musculoskeletal tumors was explored[5]. Their research identified a statistically significant difference in ADCmin values between benign and malignant tumors. Combining APT and ADC values offers a more comprehensive characterization of tumor tissues. Furthermore, the combination of MTRasymmax and ADCmin demonstrates an enhanced diagnostic performance.Conclusions
The combination of APTWI and DWI offers valuable insights into changes in cellular proteins and peptides, alongside water diffusion properties within tumors. When MTRasymmax is combined with ADCmin, it yields superior diagnostic performance for distinguishing between malignant and benign bone and soft tissue tumors.Acknowledgements
No acknowledgement found.References
1.Togao O, Hiwatashi A, Yamashita K, Kikuchi K, Keupp J, Yoshimoto K, et al. Grading diffuse gliomas without intense contrast enhancement by amide proton transfer MR imaging: comparisons with diffusion- and perfusion- weighted imaging. Eur Radiol. 2017;27(2):578–88.
2. Zhizheng Zhuo, Liying Qu, Peng Zhang, et al. Prediction of H3K27M-mutant brainstem glioma by amide proton transfer-weighted imaging and its derived radiomics[J].Eur J Nucl Med Mol Imaging,2021 ,48(13):4426-4436.
3.Meng N, Wang J, Sun J, et al. Using amide proton transfer to identify cervical squamous carcinoma/adenocarcinoma and evaluate its diferentiation grade[J]. Magn Reson Imaging. 2019,61:9-15.
4.Dallaudière B, Lecouvet F, Vande Berg B, Omoumi P, Perlepe V, Cerny M, et al. Diffusion-weighted MR imaging in musculoskeletal diseases: current concepts. Diagn Interv Imaging. 2015;96(4):327-40.
5.Sevtap Arslan, Fatma Bilge Ergen, Güzide Burça Aydın, et al. Different Attenuation Models of Diffusion-Weighted MR Imaging for the Differentiation of Benign and Malignant Musculoskeletal Tumors[J].J Magn Reson Imaging,2022,55(2):594-607.
Figures