1682
Application value of amide proton transfer imaging in differentiating benign, intermediate and malignant bone and soft tissue tumors1MRI Department, Honghui Hospital affiliated to Xi'an Jiaotong University, Xi'an, China, 2Department of Clinical and Technical Support, Philips Healthcare, Xi'an, China
Synopsis
Keywords: Bone, MSK, tumor; MRI; APT
Motivation: Current imaging methods for detecting tumor protein content are immature, thereby limiting early diagnosis, qualitative assessment, and post-treatment evaluation.
Goal(s): Magnetic resonance imaging (MRI) has contributed significantly to improvement in the management of bone and soft tissue tumors. However, the use of MRI based amide proton transfer (APT) technique to diagnose bone and soft tissue tumors remain less explored.
Approach: We use APT imaging to distinguish benign, intermediate and malignant bone and soft tissue tumors.
Results: APT value was different in benign, intermediate and malignant tumors. There is high sensitivity and specificity for the qualitative diagnosis of bone and soft tissue tumors.
Impact: APT imaging can provide diagnostic basis for the qualitative diagnosis of bone and soft tissue tumors. However, this imaging method is interfered by many factors. Whether tumors of different tissue sources have different APT characteristics needs further study.
Introduction
Bone and tissue tumors are pathologically based on the increase in the concentration and speed of intracellular protein synthesis by abnormal cell proliferation1. Amide proton transfer imaging (APT) technique is a novel MRI tool to detect amido-protons in free proteins and peptides in vivo2. It uses the presence of endogenous cellular proteins to produce an MR signal that directly correlates with cell proliferation, a marker of tumor activity. At present, the research of APT imaging in tumor mainly focuses on intracranial tumors3. In addition, APT imaging has also been studied in other tumor sites, such as rectal, cervical, and breast tumors4-7. However, there are few relevant reports on APT imaging in bone and soft tissue tumors. In this study, we investigated the application value of APT imaging in differentiating benign, intermediate and malignant tumors of bone and soft tissue in lower limb.Material and Methods
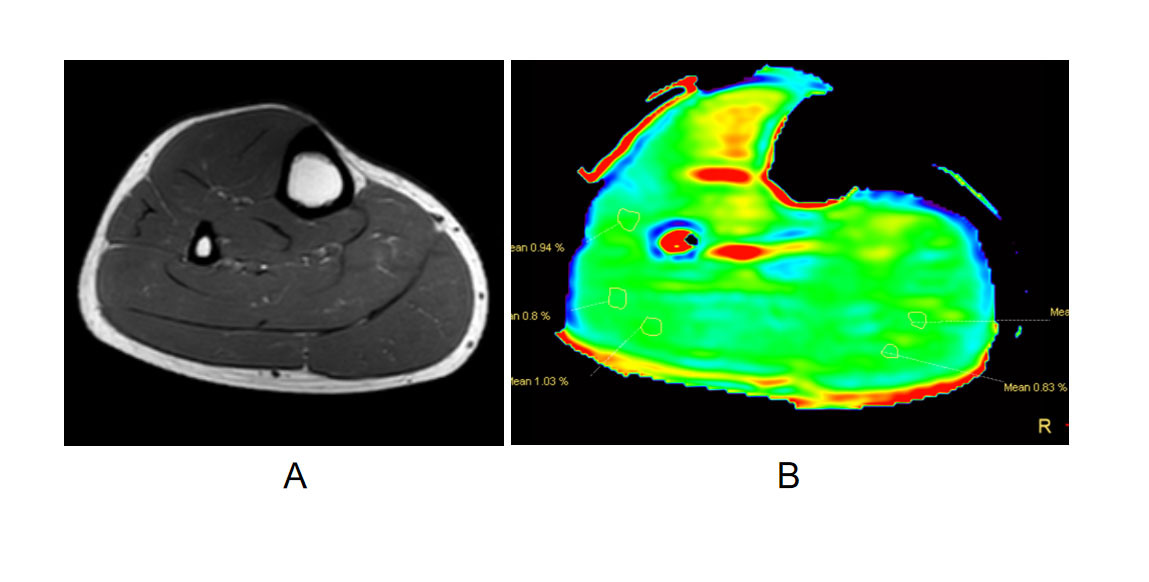
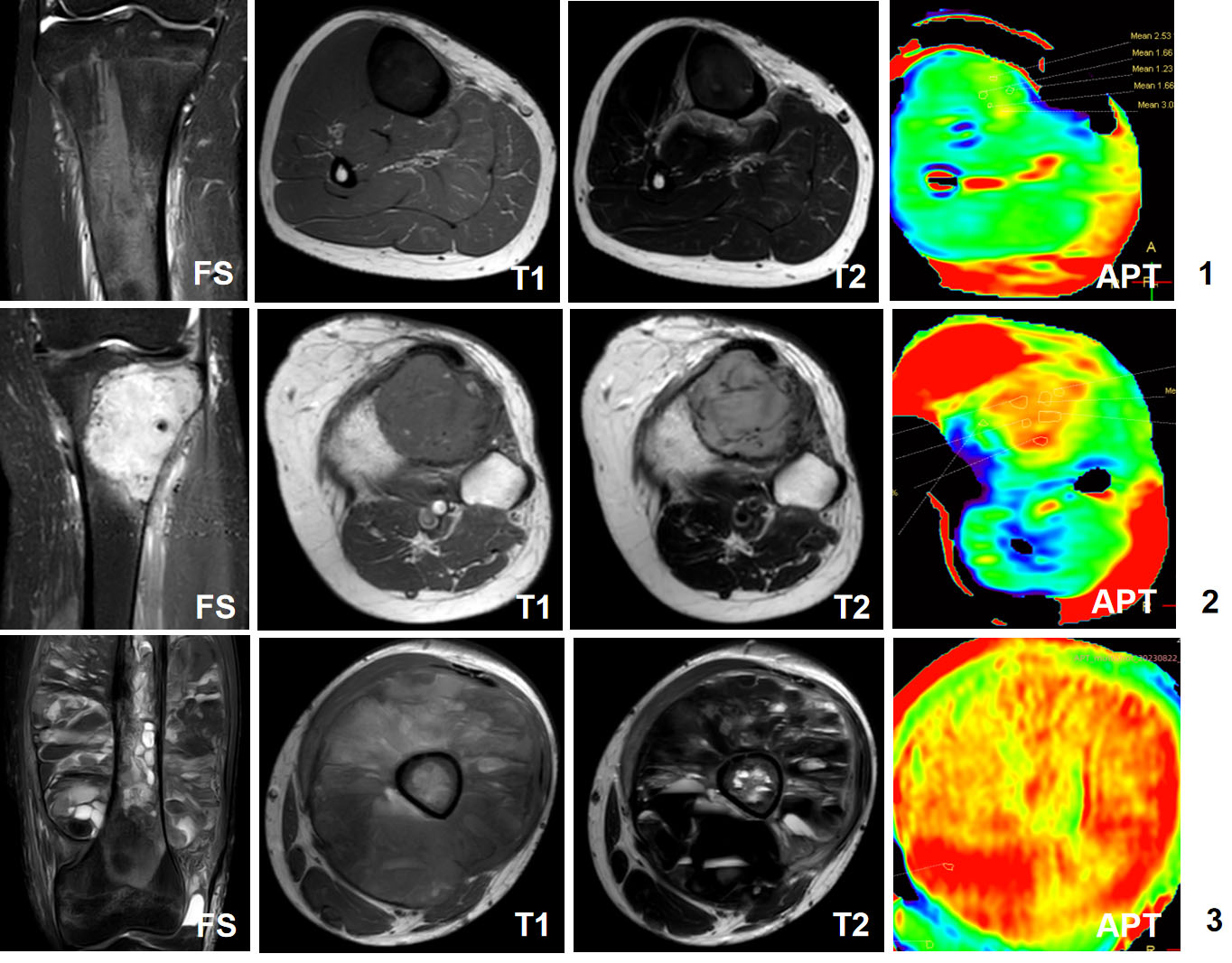
Fifteen healthy controls (HCs) and thirty-one patients with bone or soft tissue tumors were enrolled. The data was conducted in 3.0T Ingenia CX System (Philips Healthcare, The Netherlands). All subjects had MR scanning two weeks before surgery. The pathological results were obtained by surgical treatment. Scanning sequences include coronal fat saturation T2WI (FS-T2WI), transverse T1WI and T2WI, and transverse APT imaging. We compare the statistical differences in APT values among control subject, benign tumor, intermediate-locally aggressive tumor, malignant tumor. Statistical analysis was accomplished with the MedCalc 13.0 and SPSS 19.0 software. A two-way model average measure intraclass correlation coefficient (ICC) was used to test the interobserver agreement. The independent sample T test was applied to the data following normal distribution. The non-parametric analysis independent sample Mann-Whitney U test was applied to the data which didn’t follow the normal distribution. The diagnostic efficiency of APT value was evaluated by drawing Receiver Operator Characteristic (ROC) curve. P<0.05 was considered statistically significant.Results
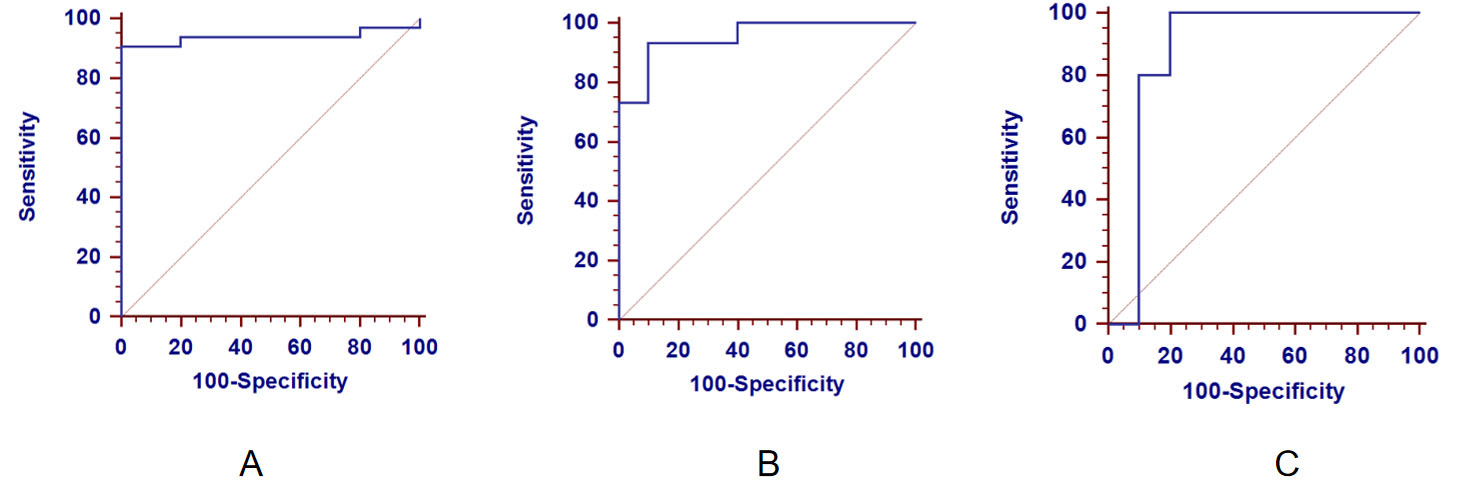
Table 1 showed the demographic features of the enrolled subjects. Figure 1 and 2 showed a representative example of HC and bone or soft tissue tumor patients, respectively. The intraclass correlation coefficient (ICC) of APT in the interobserver agreement was 0.848, P<0.001. APT value was 1.09±0.23% in control subjects, 3.62±1.66% in all the tumors, 1.11±0.35% in benign tumor, 1.26±0.52 in intermediate-locally aggressive tumor, 4.62±1.33 in malignant tumor, respectively. For the APT value in the area of ROC curve, there was statistical difference between control subject and bone/soft tissue tumor (P<0.001), control subject and benign tumor (P=0.0002), benign and malignant tumor (P<0.0001), intermediate-locally aggressive and malignant tumor (P<0.0001), whereas no statistical difference in benign and intermediate-locally aggressive tumor (P=0.085). ROC curve analysis showed that (1) when APT value ≥1.46, the sensitivity and specificity of the diagnosis in bone/soft tissue tumor was 90.6% and 100%, respectively; (2) when APT value ≤3.01, the sensitivity and specificity of the diagnosis in benign tumor was 83.33% and 90%; (3) when APT value ≥4.69, the sensitivity of the diagnosis in malignant tumor was 83.33%, and the specificity was 90% (Figure 3).Discussion
In this study, APT values in normal muscle tissue, bone and soft tissue tumors in the lower limb had a good repeatability. There were differences in the APT value among benign, intermediate and malignant bone and tissue tumors. The cutoff values of ATP were 1.46, 3.01, and 4.69 in the diagnosis of benign, intermediate and malignant bone and tissue tumor, respectively. APT is geared towards detecting the exchangeable amide protons in the backbone of mobile proteins8-10. There have been several studies demonstrating the relationship between the APT signal and protein expression11-12 .The high signal intensity of APT may represent the active metabolism of tumors and the production of large amounts of proteins. The proliferation rate of malignant tumors increased rapidly, the content of protein and polypeptide in tumor cells increased, the chemical exchange saturation transfer effect was enhanced13. The proliferation rate of benign tumor cells is slow, the content of protein and polypeptide is relatively less than that of malignant tumor, the effect of chemical exchange saturation metastasis is weaker than that of malignant tumor, and the APT value is lower than that of malignant tumor. Our results shows that the APT imaging can be used for differentiation of benign, intermediate and malignant bone and soft tissue tumors of lower limbs.Conclusion
APT imaging holds diagnostic value in distinguishing between benign, intermediate, and malignant tumors, with high sensitivity and specificity for qualitative diagnosis of bone and soft tissue tumors. This has significant implications for clinicians when formulating preoperative surgical plans.Acknowledgements
No acknowledgement found.References
1. Sagiyama K, Mashimo T, Togao O, Vemireddy V, Hatanpaa KJ, Maher EA, et al. In vivo chemical exchange saturation transfer imaging allows early detection of a therapeutic response in glioblastoma. Proc Natl Acad Sci USA 2014;111(12):4542-7.
2. Kogan F, Hariharan H, Reddy R. Chemical exchange saturation transfer (CEST) imaging: description of technique and potential clinical applications. Curr Radiol Rep 2013;1(2):102-14.
3. Bai Y, Lin Y, Zhang W, Kong L, Wang L, Zuo P, et al. Noninvasive amide proton transfer magnetic resonance imaging in evaluating the grading and cellularity of gliomas. Oncotarget 2017;8(4):5834-42.
4. Ohno Y, Yui M, Koyama H, Yoshikawa T, Seki S, Ueno Y, et al. Chemical exchange saturation transfer MR imaging: preliminary results for differentiation of malignant and benign thoracic lesions. Radiology 2016;279(2): 578-89.
5. Law BKH, King AD, Ai QY, Poon DMC, Chen W, Bhatia KS, et al. Head and neck tumors: amide proton transfer MRI. Radiology 2018;288(3):782-90.
6. Nishie A, Takayama Y, Asayama Y, Ishigami K, Ushijima Y, Okamoto D, et al. Amide proton transfer imaging can predict tumor grade in rectal cancer. Magn Reson Imaging 2018;51:96-103.
7. Meng N, Wang Xi, Sun J, et al. Comparative Study of Amide Proton Transfer-Weighted Imaging and Intravoxel Incoherent Motion Imaging in Breast Cancer Diagnosis and Evaluation. J Magn Reson Imaging, 2020, 52(4):1175-1186.
8. Kogan F, Hariharan H, Reddy R. Chemical exchange saturation transfer (CEST) imaging: Description of technique and potential clinical applications. Curr Radiol Reports 2013;1(2):102-14.
9. Vinogradov E, Sherry AD, Lenkinski RE. CEST: From basic principles to applications, challenges and opportunities. J Magn Reson 2013;229:155-72.
10. Jones KM, Pollard AC, Pagel MD. Clinical applications of chemical exchange saturation transfer (CEST) MRI. J Magn Reson Imaging 2018;47:11-27.
11. Togao O, Yoshiura T, Keupp J, Hiwatashi A, Yamashita K, Kikuchi K, et al. Amide proton transfer imaging of adult diffuse gliomas: correlation with histopathological grades. Neuro-oncology 2014;16(3):441-8.
12. Zhou J, Zhu H, Lim M, Blair L, Quinones-Hinojosa A, Messina SA, et al. Threedimensional amide proton transfer MR imaging of gliomas: initial experience and comparison with gadolinium enhancement. J Magn Reson Imaging 2013;38(5):1119-28.
13.Hobbs SK, Shi G, Homer R, Harsh G, Atlas SW, Bednarski MD. Magnetic resonance image-guided proteomics of human glioblastoma multiforme. J Magn Reson Imaging 2003;18(5):530-6.
Figures