1680
FRACTURE-Angiography: simultaneous acquisition of bone imaging and angiography1Department of Radiology, Chiba University Hospital, Chiba city, Japan, 2Department of Diagnostic Radiology and Radiation Oncology, Graduate School of Medicine, Chiba University, Chiba city, Japan, 3Department of Orthopaedic Surgery, Graduate School of Medicine, Chiba University, Chiba city, Japan, 4Philips Japan, Tokyo, Japan
Synopsis
Keywords: Bone, Bone
Motivation: In preoperative cervical spine assessment, precise visualization of the vertebral artery (VA) course is of paramount importance. We present a new sequence called FRACTURE-Angiography.
Goal(s): The purpose is to evaluate the clinical applicability of FRACTURE-Angiography compared to FRACTURE and TOF-MRA.
Approach: Both quantitative and qualitative evaluations were performed. In the quantitative evaluations, we assessed the depiction ability of the VA and bone tissue based on the contrast ratio with background tissue. The qualitative evaluations for 3D-fusion images were conducted from the perspectives of bone morphology and VA course.
Results: FRACTURE-Angiography could image arterial signals and bone morphology simultaneously and satisfy clinical requirements.
Impact: FRACTURE-Angiography allows simultaneous acquisition of bone tissue and arterial images in a single imaging session. As a result, it has the advantage of shortening scan time and minimizing the gap between scans.
INTRODUCTION
In preoperative cervical spine assessment, precise visualization of the vertebral artery (VA) course is of paramount importance1,2. Typically, the evaluation for VA involves using computed tomography angiography (CTA) to assess especially high-riding VA3,4. In addition, some techniques use MRI for reasons of contrast administration limitations, such as iodine allergy or renal dysfunction. Specifically, the evaluation of VA involves time of flight magnetic resonance angiography (TOF-MRA)5,6, while the assessment of bone morphology is achieved through a CT-like imaging technique known as fast field echo resembling a CT using restricted echo-spacing (FRACTURE)7. FRACTURE can be observed in a 3D-images. Fusing both modalities makes it possible to three-dimensionally comprehend the relationship between the VA and bone morphology (FRACTURE-fused-TOF).In this study, we present a new sequence called FRACTURE-Angiography. The technique of FRACTURE-Angiography is shown in Figure 1. By combining TOF-MRA principles with FRACTURE, arterial signals and bone morphology can be imaged simultaneously. The purpose of this study is to evaluate the clinical applicability of FRACTURE-Angiography compared to FRACTURE-fused-TOF.
METHODS
Eight healthy volunteers (median age 27) were included in this study. We used a 3.0-Tesla MRI system (Philips Ingenia) to image from C1 Level to a proximal 15 cm. The scanning parameters are summarized in Figure 2. FRACTURE-Angiography collected 5 echoes. In-phase summed images were used for evaluating bone tissue, and out-of-phase summed images were used for assessing arteries. Both quantitative and qualitative evaluations were performed.In the quantitative evaluations, we assessed the depiction ability of the VA and bone tissue based on the contrast ratio (CR) with background tissue (muscle). CR was calculated from the signal intensity of the bone, muscle, and VA, as shown in Figure 3a.
Visual evaluations for 3D-fusion images were conducted from the perspectives of bone morphology and VA course. 3D-fusion images were created using Ziostation2 (Ziosoft, Japan). Three radiologists conducted the visual evaluations. The evaluation was divided into four categories, considering critical points for preoperative cervical spine evaluation in Figure 3b. Visual evaluation was performed on a four-grade scale with 4 being the highest score for each of the four categories. To evaluate the agreement in visual assessments, 3D-fusion images were created by two radiological technologists and evaluated with the same scale, since the assessment depends on WW/WL and individual skills of 3D-fusion. The agreement was evaluated using weighted Kappa coefficients8.
The statistical significance of the quantitative data was determined with the Wilcoxon Signed-Rank test and the Steel–Dwass test. Statistical significance was considered P<0.05.
RESULTS
The results of the quantitative evaluation are shown in Figure 4. CR of VA in FRACTURE-Angiography was significantly higher with FRACTURE, but lower than with TOF-MRA. (P<0.05). CR of bone tissue in FRACTURE-Angiography was significantly lower when compared to FRACTURE (P<0.05).The results of the qualitative evaluation are shown in Figure 5. Good evaluations were observed for all items, with no significant differences between FRACTURE-fused-TOF and FRACTURE-Angiography. The agreement of the evaluation grades by 3D-Fusion images creators was moderate to substantial in the Landis9 classification (Kappa coefficient 0.55-0.74).
DISCUSSION
FRACTURE-Angiography could observe VA course of the cervical spine without changing the visibility of 3D-images. In the cervical region, patient cooperation is important to reduce motion artifacts due to swallowing and breathing. The reduced imaging time with FRACTURE-Angiography can improve the success rate of the examination.In the quantitative evaluation, CR of VA in FRACTURE-Angiography was lower than that of TOF-MRA. This is because FRACTURE-Angiography uses a lower flip angle (FA), which results in a higher background signal10. It is very important for FRACTURE-Angiography to ensure signal-to-noise ratio (SNR) of the background signal and bone tissue when generating 3D-images. Increasing multi chunk decreases SNR. Therefore, a low FA was chosen to enhance the evenness of the arterial signal in the long-axis direction without sacrificing SNR.
Furthermore, CR of bone tissue in FRACTURE-Angiography was lower compared to FRACTURE. FRACTURE-Angiography uses fewer echoes for bone tissue imaging than FRACTURE. Longer TE images with particularly strong contrast between bone tissue and background signal were not acquired. This is the reason for the lower contrast. Decreased contrast makes it difficult to separate the target area from the background tissue when creating 3D-images.
However, the visual evaluations showed that the relationship between the cervical spine and VA was well evaluated. Moreover, the acquired images are independent of the image creator because the agreement of the evaluation scores by the image creator was moderate to substantial.
CONCLUSION
FRACTURE-Angiography could image arterial signals and bone morphology simultaneously and satisfy clinical requirements.Acknowledgements
No acknowledgement found.References
1. Hsu, W.K.; Kannan, A.; Mai, H.T.; et al. Epidemiology and Outcomes of Vertebral Artery Injury in 16 582 Cervical Spine Surgery Patients: An AOSpine North America Multicenter Study. Glob. Spine J. 2017, 7, 21S–27S.
2. Zhu, W.; Wang, Y.-F.; Dong, X.-F.; et al. Study on the correlation of vertebral artery dominance, basilar artery curvature and posterior circulation infarction. Acta Neurol. Belg. 2016, 116, 287–293.
3. Yamazaki M.; Okawa A.; Furuya T.; et al. Anomalous Vertebral Arteries in the Extra- and Intraosseous Regions of the Craniovertebral Junction Visualized by 3-Dimensional Computed Tomographic Angiography: Analysis of 100 Consecutive Surgical Cases and Review of the Literature. Spine 37(22):p E1389-E1397, October 15, 2012.
4. Wakao N.; Takeuchi M.; Kamiya M.; et al. Variance of cervical vertebral artery measured by CT angiography and its influence on C7 pedicle anatomy. Spine (Phila Pa 1976). 2014;39(3):228-232.
5. Mair G. Lack of flow on time-of-flight MR angiography does not always indicate occlusion. BJR Case Rep. 2015 Jun 10;2(1):20150187.
6. Li S.; Li Y.; Bai M.; et al. Three-dimensional time-of-flight magnetic resonance angiography detection of duplication of the vertebral artery in a large Chinese population. Med Sci Monit. . 2016 Oct 17;22:3771-3777.
7. Johnson B.; Alizai H.; Dempsey M.; Fast field echo resembling a CT using restricted echo-spacing (FRACTURE): a novel MRI technique with superior bone contrast. Skeletal Radiol. 2021;50(8):1705-1713.
8. Jacob, Cohen. A Coefficient of agreement for nominal Scales. Educational and Psychological Measurement, 20(1):37-46.
9. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977 Mar;33(1):159-74.
10. Runge, Val M; Johannes T Heverhagen; Flip Angle, TR, MT, and Field Strength (in 3D TOF MRA) BT - The Physics of Clinical MR Taught Through Images. 172–73. Cham: Springer International Publishing, 2022.
Figures
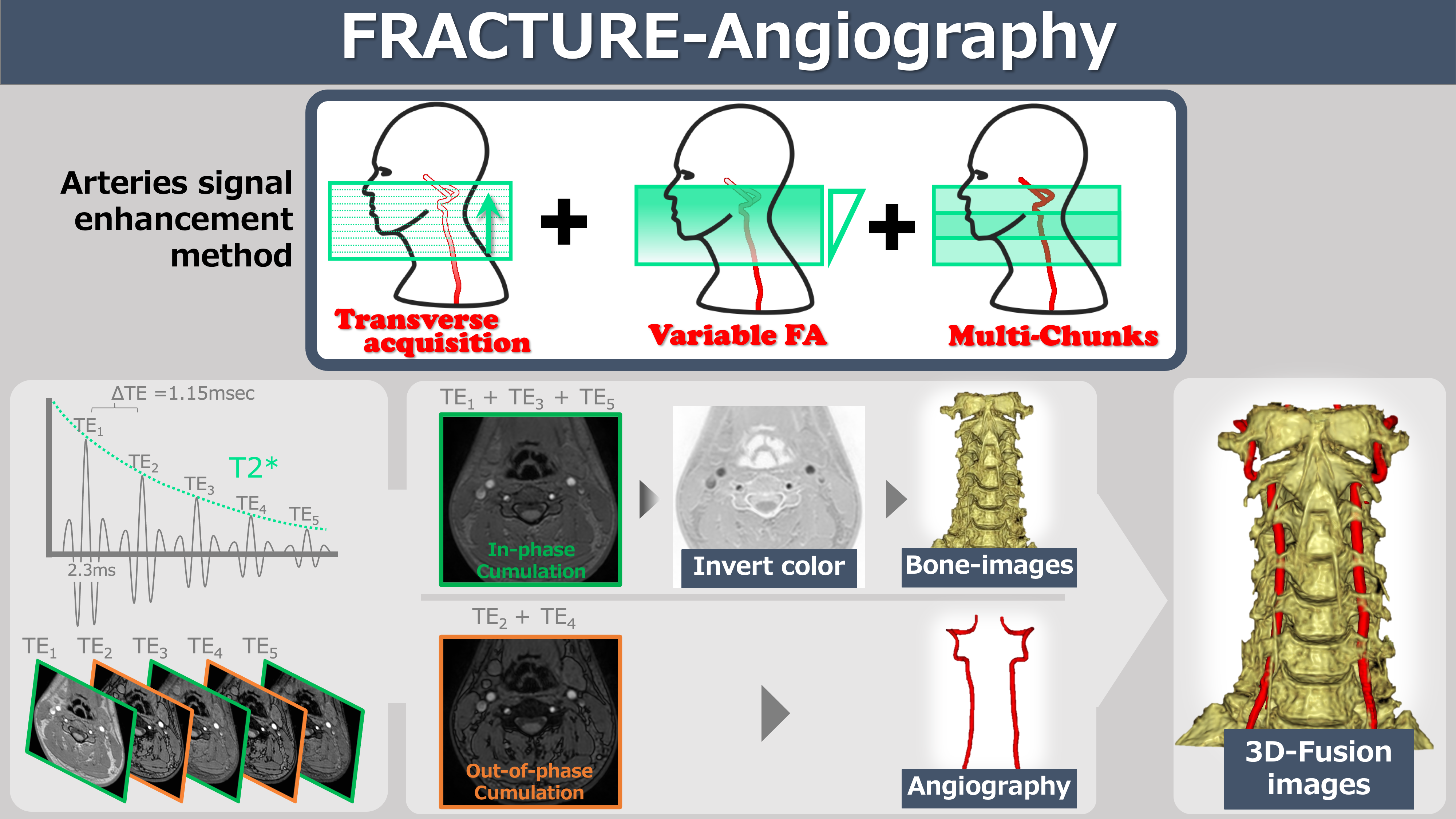
Figure 1.
FRACTURE-Angiography enhances the arteries signal by using transverse acquisition, variable flip angle (FA), and Multi-chunk techniques. While regular FRACTURE acquires In-phase images, FRACTURE-Angiography adds Out-of-phase images to achieve fat suppression effects, further improving artery depiction. (First echo time was 2.3 ms in in-phase and echo space-time was 1.15 ms in out-of-phase)
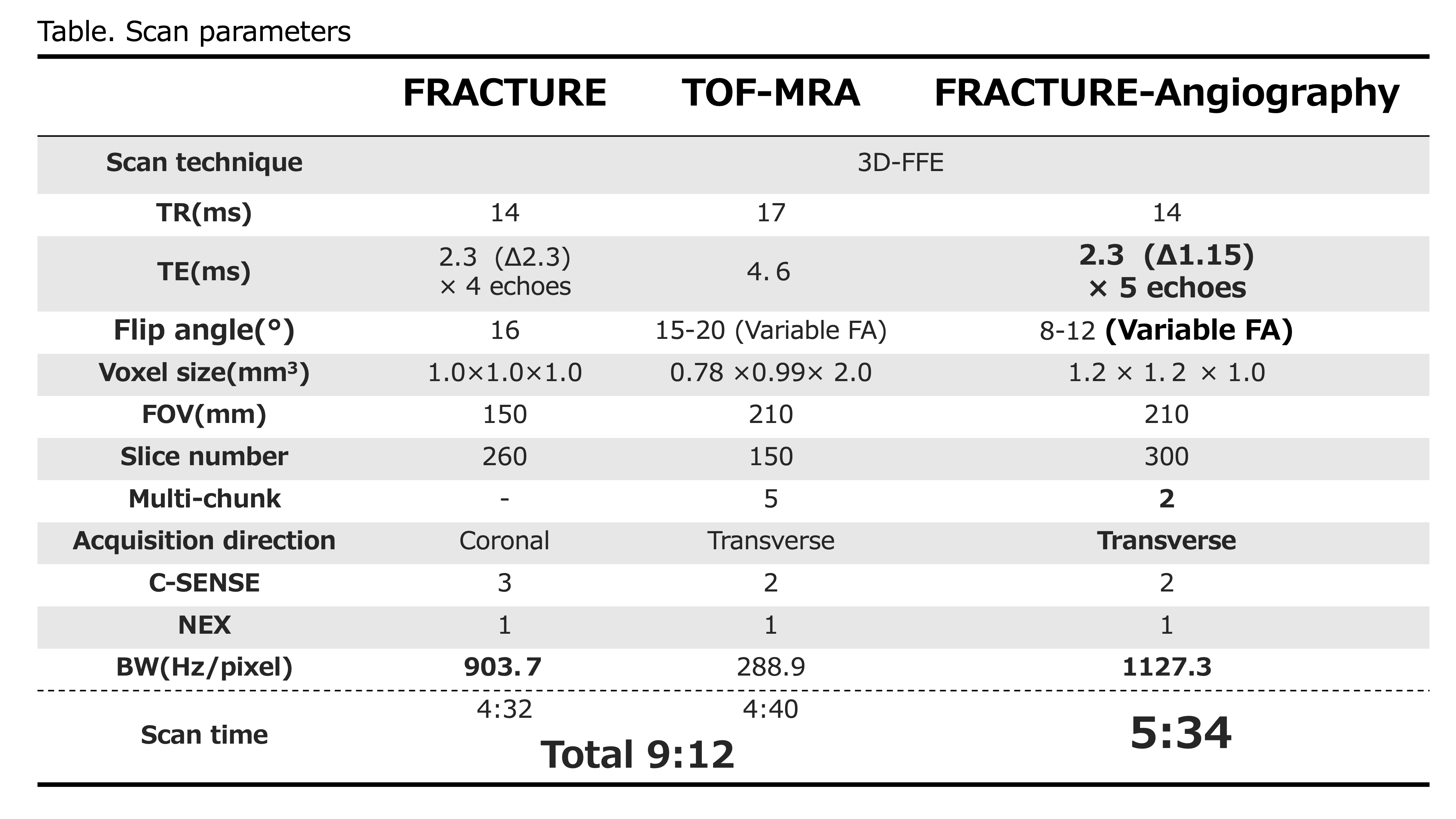
Figure 2.
The following were the scan parameters. The boldface values shown for FRACTURE-Angiography are the modified values of FRACTURE. It is important to point that the scan time for FRACTURE-Angiography is about half less than the total time for FRACTURE and TOF-MRA.
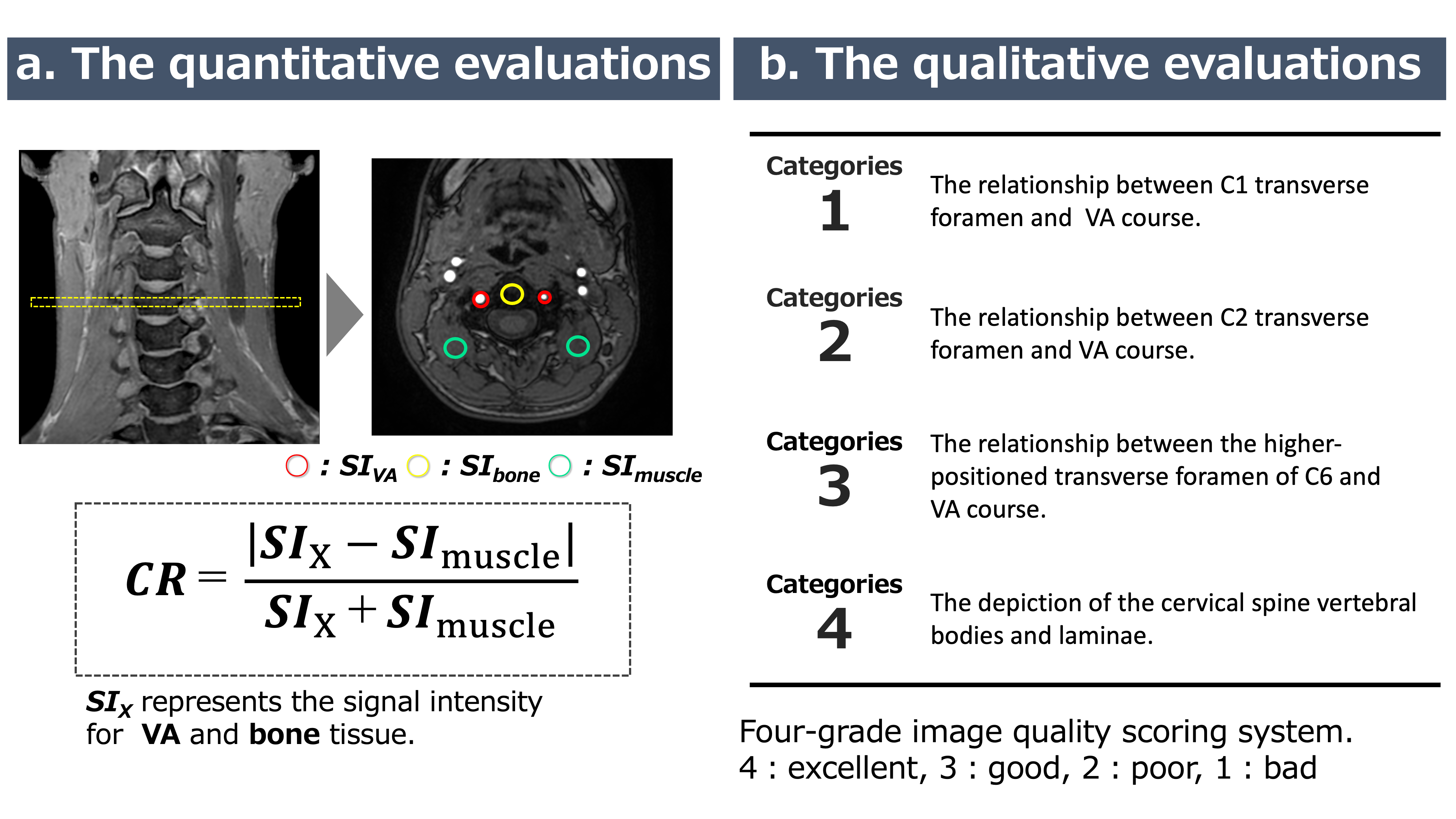
Figure 3.
a. The quantitative evaluations: We defined a region of interest (ROI) with a 5 mm2 diameter in the central slice for bone, muscle, and VA and measured the signal intensity (SI). Contrast ratio was calculated using the following figure, where SIX represents SI for VA and bone tissue. Individual SI values were represented as the average within the ROI.
b. The qualitative evaluations: The evaluation was divided into four categories and scored on a four-grade scale (4: excellent, 3: good, 2: poor, 1: bad), considering key points in the preoperative cervical spine evaluation.
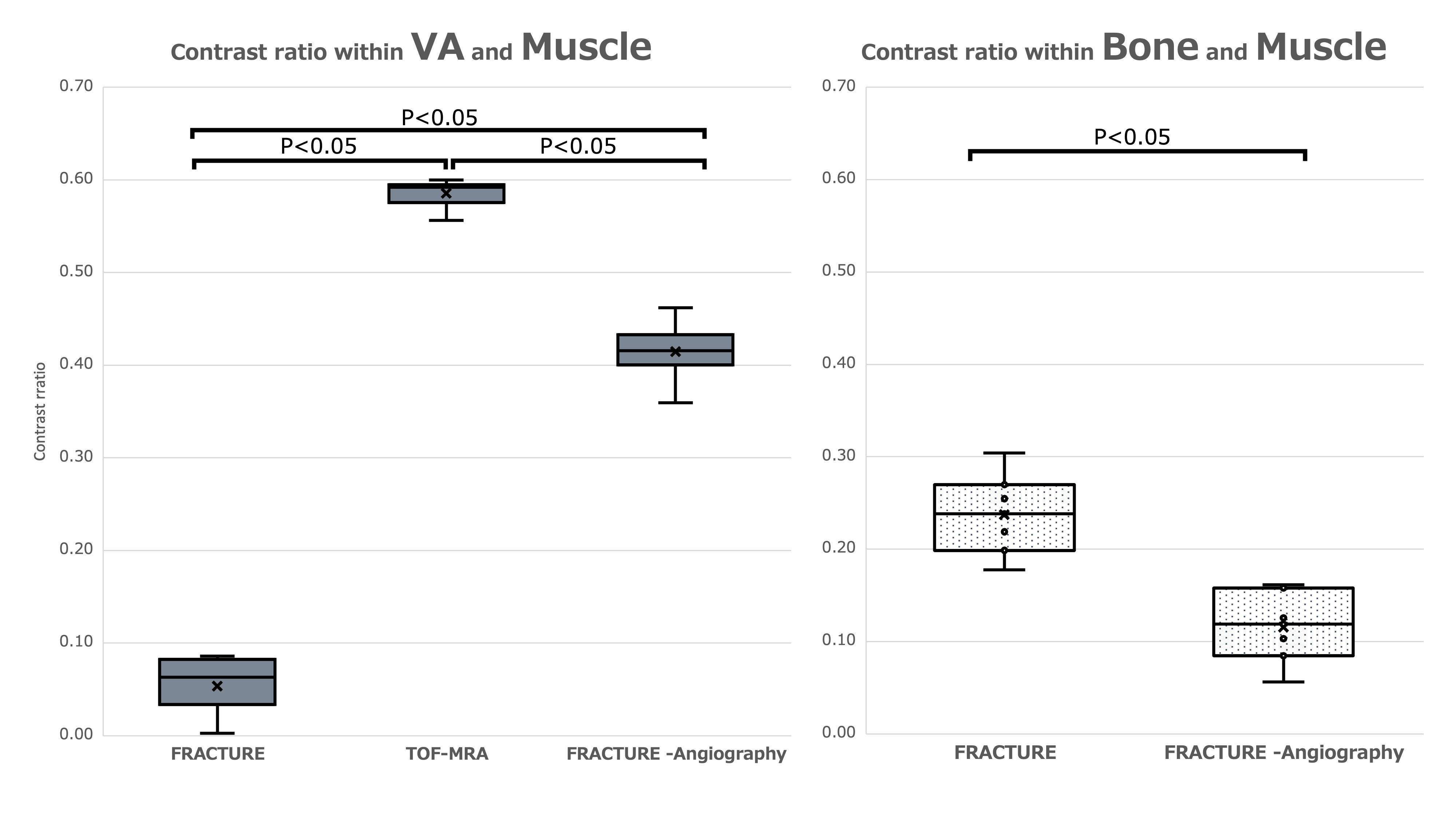
Figure 4.
Box plot showing contrast ratio (CR) of the vertebral artery (VA) and bone tissue. Contrast ratio of the vertebral artery in FRACTURE-Angiography was predominantly higher with FRACTURE, but lower than with TOF-MRA. (FRACTURE vs. TOF-MRA vs. FRACTURE-Angiography, median 0.06 [IQR 0.03-0.08] vs. median 0.59 [IQR 0.58-0.59] vs. median 0.42 [IQR 0.41-0.43], P<0.05). CR of bone tissue in FRACTURE-Angiography was predominantly lower when compared to FRACTURE (median 0.24 [IQR 0.20-0.27] vs. median 0.12 [IQR 0.08-0.16], P<0.05).
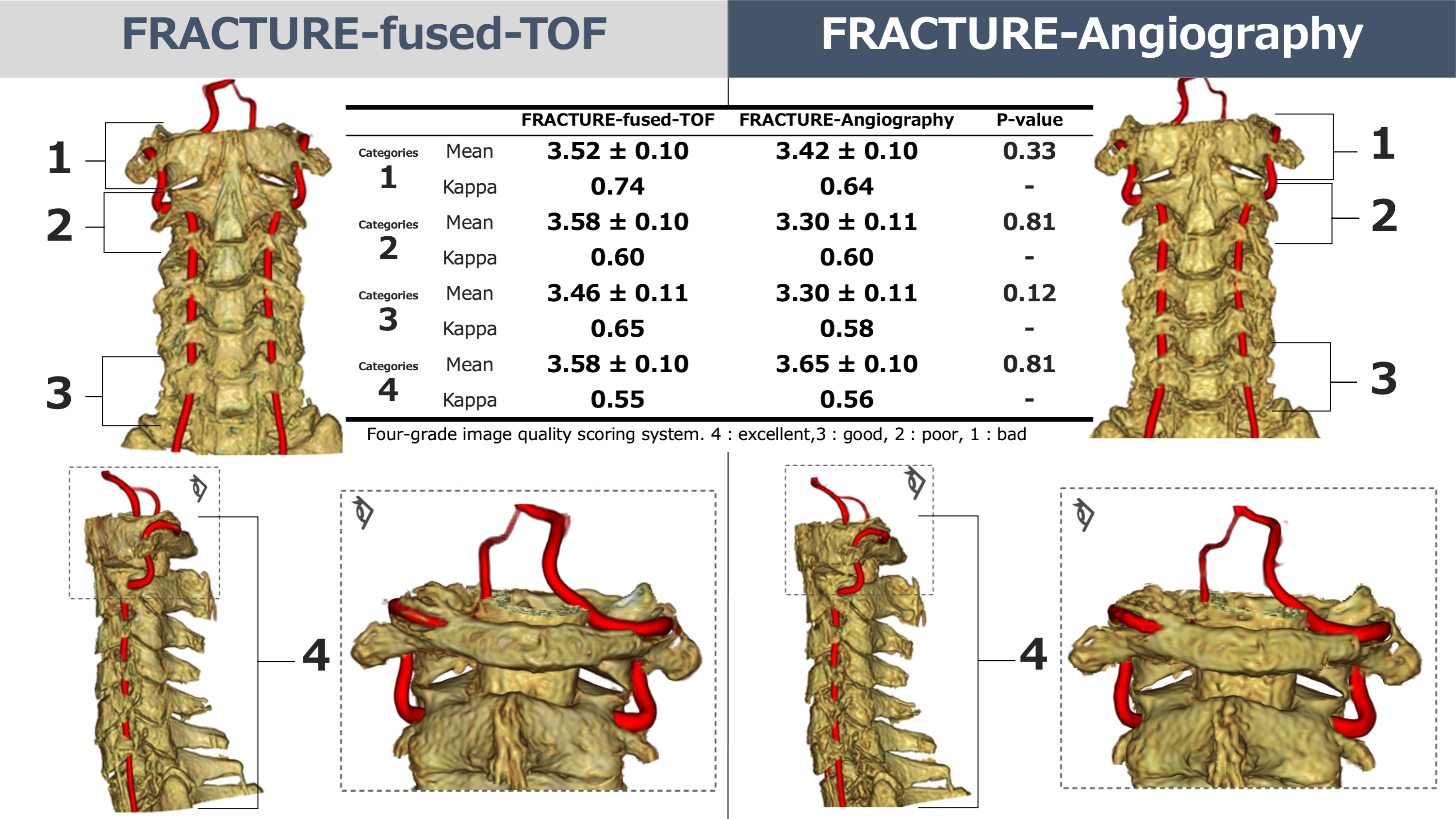
Figure 5.
Diagram of the results of visual evaluation with 3D-fusion images of FRACTURE-fused-TOF and FRACTURE-Angiography.Good evaluations were observed for all items, with no significant differences between FRACTURE-fused-TOF and FRACTURE-Angiography. The agreement of the evaluation grades by the 3D-Fusion images creators was moderate to substantial in the Landisclassification (Kappa coefficient 0.55-0.74).