1675
The Feasibility of Analyzing Systolic and Diastolic Myocardial Volume Ratio Based on CMR to Evaluate Myocardial Fibrosis in HCM Patients1The First Afliated Hospital of Harbin Medical University, Harbin, China, 2Philips Healthcare, Beijing, China
Synopsis
Keywords: Myocardium, Cardiomyopathy
Motivation: CMR, the gold standard for diagnosing myocardial diseases, is known for its ability to assess local myocardial fibrosis through LGE imaging. However, this imaging technique requires a contrast agent, limiting its use in patients with allergies or renal dysfunction.
Goal(s): The purpose of this study is to assess the ability of MVs/MVd as a new indicator to measure the extent of myocardial fibrosis.
Approach: Explore the correlation between MVs/MVd and LGE% in patients with hypertrophic cardiomyopathy.
Results: The results indicate that MVs/MVd may possess the ability to indicate myocardial fibrosis without the need for a contrast agent.
Impact: MVs/MVd, in contrast to traditional methods, directly measures the entire cardiac cycle, offering valuable insights into myocardial properties. Importantly, it can gauge myocardial fibrosis to some extent without requiring a contrast agent, making it clinically significant for diagnosis and treatment.
Introduction
Hypertrophic cardiomyopathy (HCM) demonstrates a substantial correlation between myocardial fibrosis and the incidence of malignant arrhythmias and sudden cardiac death[1].Late gadolinium enhancement(LGE) serves as widely recognized for its capability to assess regional myocardial fibrosis[2]. However, the procedure necessitates the use of a requires a contrast agent, and the demand for contrast agent injection restricts its applicability in patients with contrast agent allergies and those with renal dysfunction.The objective of this study is to employ the left ventricular myocardial volume ratio during systole to diastole (MVs/MVd), a contrast agent-free parameter[3]. This approach could directly observes myocardial compressibility throughout the cardiac cycle using CMR imaging technology. By investigating the correlation between MVs/MVd and LGE%, our goal is to ascertain whether MVs/MVd, as a novel indicator, can effectively reflect the extent of myocardial fibrosis.Methods
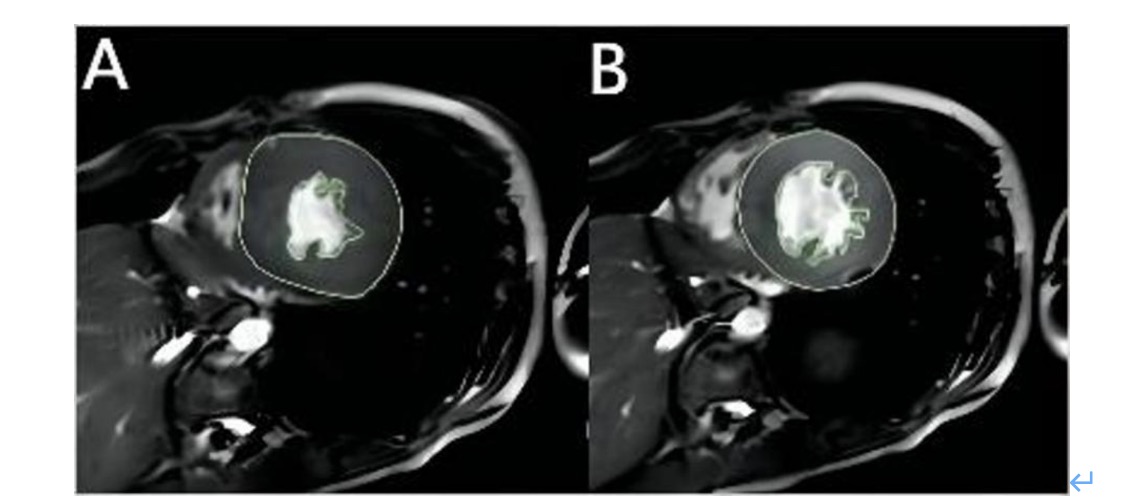
A retrospective analysis was performed for patients diagnosed with HCM from September 2018 to May 2021. Image acquisition was carried out using a 3.0-Tesla magnetic resonance scanner (Ingenia Elition; Philips Healthcare, Best, the Netherlands) with a ISP workstation (Intellispace Portal; Version 10.1) for post-processing. The scanning sequences included four-chamber, short-axis, and left ventricular long-axis planes. HCM patients were categorized into two groups: those with LVEF≥50% and those with LVEF<50%. Manual delineation of the endocardial and epicardial boundaries in the left ventricular short-axis cine sequences was executed (Fig.1). The area of each image slice was calculated by multiplying the slice thickness by the image gap, providing the volume of each slice, and summing the volumes of all slices determined the myocardial volume. Statistical analysis was conducted using SPSS 26.0 software, with the Mann-Whitney U test employed for non-normally distributed continuous variables. Categorical variables were evaluated using the chi-square test. Intra-observer and inter-observer consistency for quantitative data, measured by different observers on two occasions,was assessed using Spearman's correlation coefficient. Receiver Operating Characteristic (ROC) curve analysis was performed, with significance denoted by P<0.05.Results
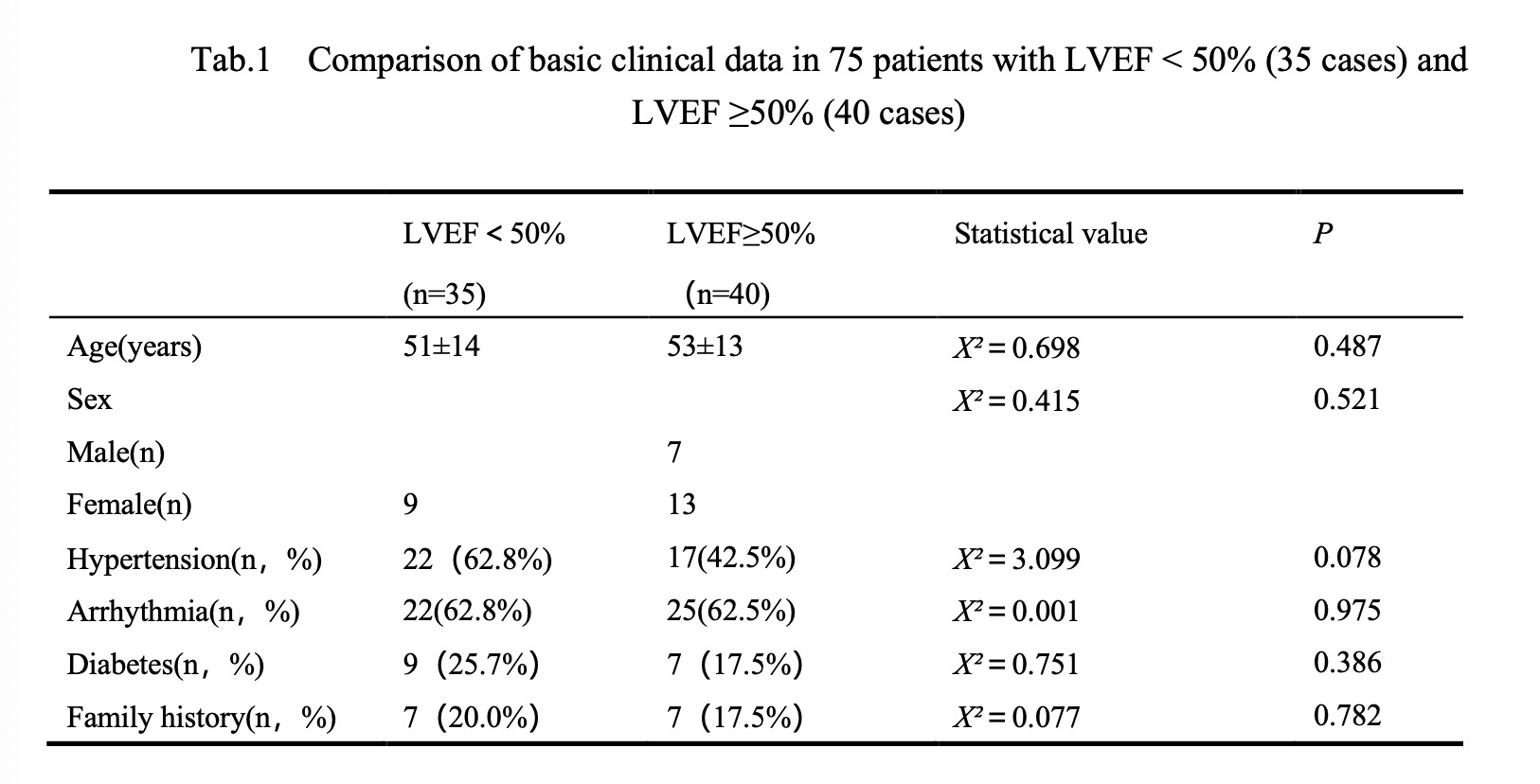
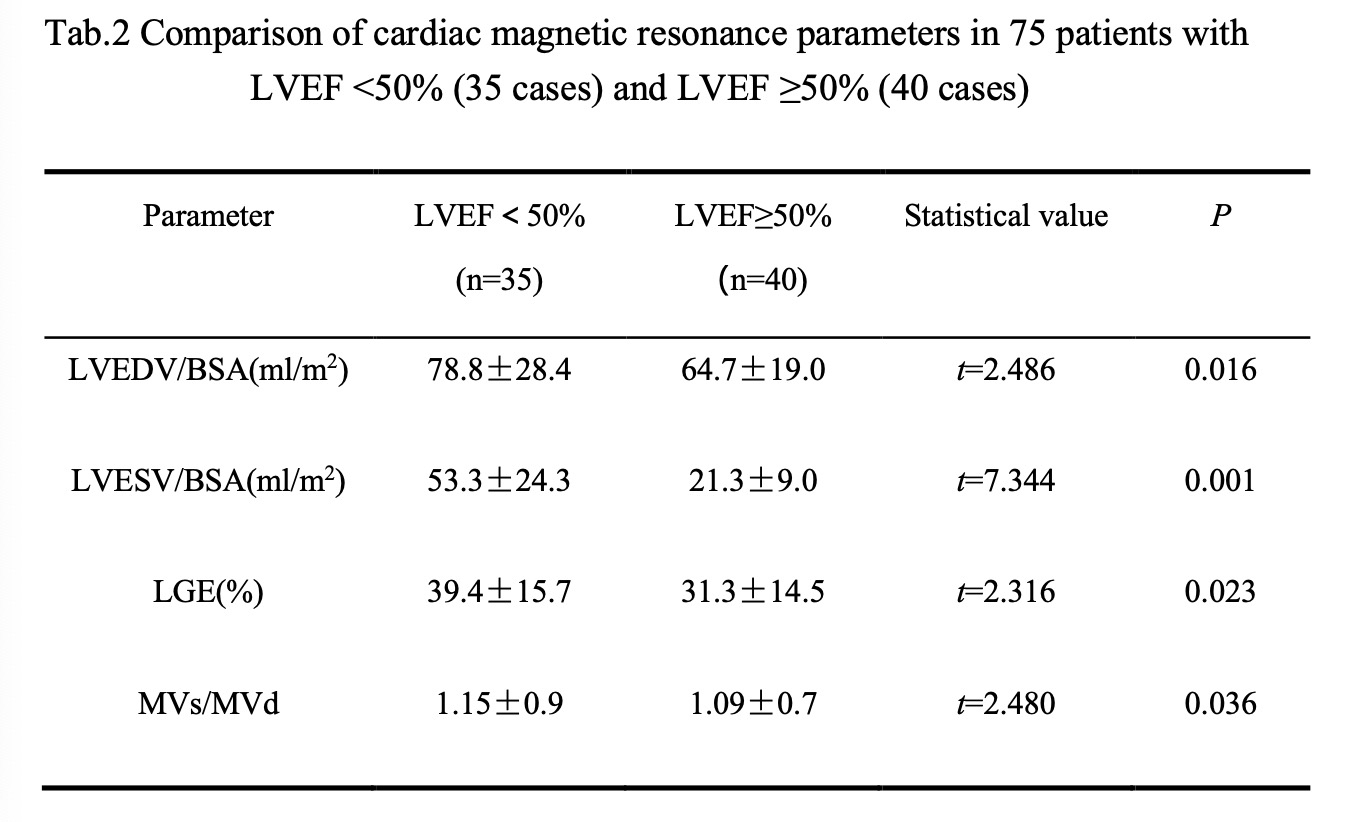
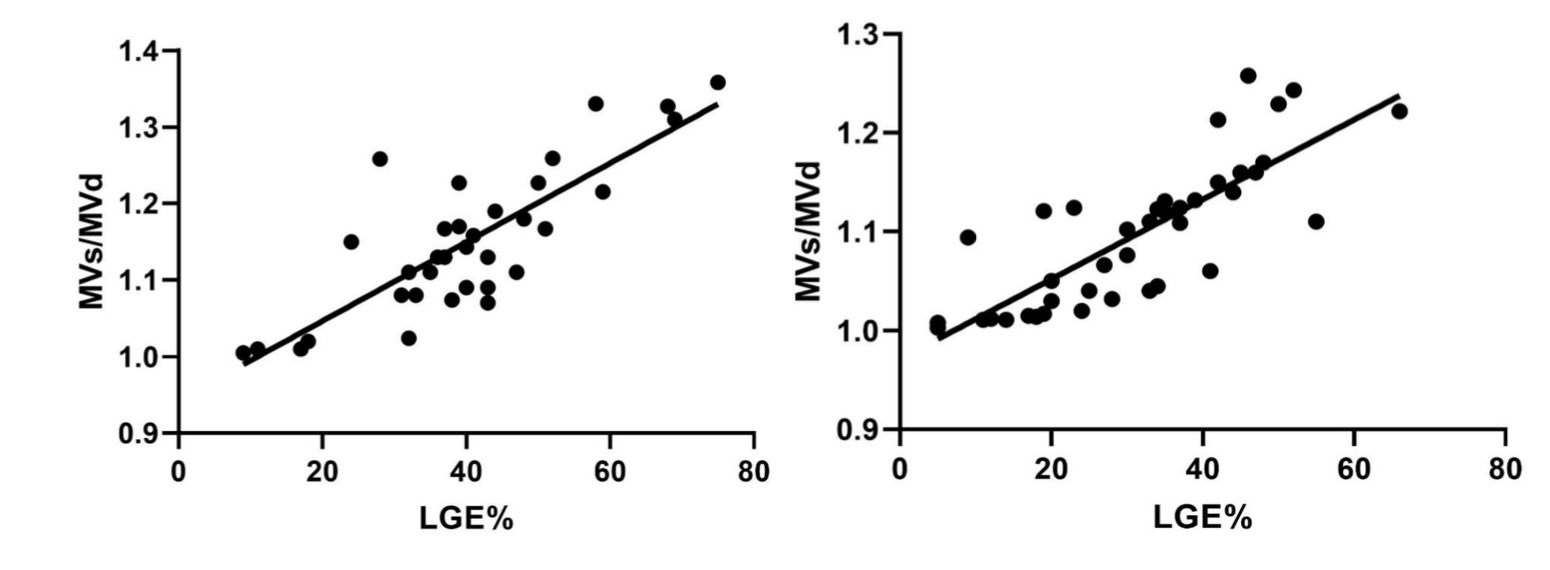
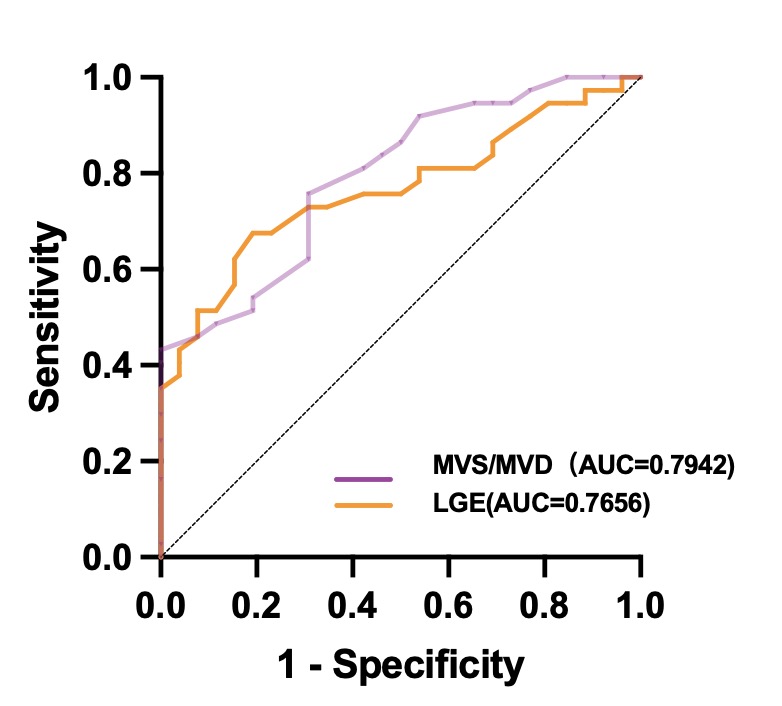
This study included a total of 75 patients diagnosed with HCM, and they were classified into two groups based on their left ventricular ejection fraction (LVEF) results.One group with reduced ejection fraction (LVEF<50%) consisting of 35 cases, and another with preserved ejection fraction (LVEF≥50%) comprising 40 cases. Clinical factors such as age, history of hypertension, history of arrhythmias, history of diabetes, and family history showed no significant correlation between the two groups (all P>0.05) (Tab.1).In the LVEF<50% group, left ventricular end-diastolic volume (78.8±28.4ml/m2vs 64.7±19.0 ml/m2, P=0.016), left ventricular end-systolic volume (53.3±24.3 ml/m2 vs 21.3±9.0 ml/m2, P=0.001), and late gadolinium enhancement percentage (39.4±15.7% vs 31.3±14.5%, P=0.023) were all higher than those in the LVEF≥50% group (P<0.05). The MVs/MVd value (1.15±0.9 vs 1.09±0.7, P=0.036) was also higher than in the preserved ejection fraction group(Tab. 2), and in both groups, LGE% and MVs/MVd were significantly positively correlated (Fig. 2)(with r values of 0.748 and 0.856, respectively, P<0.01). In the receiver operating characteristic (ROC) curve analysis, MVs/MVd and LGE displayed area under the curves of 0.794 and 0.766, respectively (Fig. 3).Discussion
This study illustrated that MVs/MVd may serve as a novel indicator with the capability to reveal myocardial fibrosis without the need for a contrast agent. Furthermore, MVs/MVd values were higher in the LVEF<50% group compared to the LVEF≥50% group.The variation in myocardial volume variation is likely to originate from the periodic inflow and outflow of blood. Hao et al. have demonstrated in an animal model that the myocardial compressible model aligns better with myocardial tissue dynamics[4,5]. An LVEF<50% is considered a threshold for classifying hypertrophic cardiomyopathy with systolic dysfunction, and systolic dysfunction (left ventricular ejection fraction <50%) is a strong predictor of sudden cardiac death (SCD) in patients[6,7]. Patients in the LVEF<50% group had higher left ventricular end-diastolic volume (LVEDV), left ventricular end-systolic volume (LVESV), and LGE% compared to the LVEF≥50% group. This could be attributed to the reduced contractility of the left ventricular myocardium, aligning with prior research[8]. A study by T. Konno indicated that in patients with hypertrophic cardiomyopathy, a higher collagen content in biopsy samples was associated with higher LGE% values. This implies that LGE can depict the presence and extent of myocardial scarring in HCM biopsy samples[9]. It also clarifies that higher LGE% values correspond to reduced myocardial compressibility, leading to an increased MVs/MVd ratio.Conclusions
Left ventricular MVs/MVd in HCM is positively correlated with LGE%, suggesting that MVs/MVd may serve as a novel indicator of myocardial function with the potential to assess the degree of myocardial fibrosis. It also indicates that MVs/MVd may detect myocardial functional decline earlier than changes in ejection fraction.Acknowledgements
NoneReferences
1. Makavos G, Κairis C, Tselegkidi M, et al: Hypertrophic cardiomyopathy: an updated review on diagnosis, prognosis, and treatment. Heart failure reviews 24:439-459, 2019.
2. Holtackers R, Emrich T, Botnar R, et al: Late Gadolinium Enhancement Cardiac Magnetic Resonance Imaging: From Basic Concepts to Emerging Methods. RoFo : Fortschritte auf dem Gebiete der Rontgenstrahlen und der Nuklearmedizin 194:491-504, 2022.
3. Ryu AJ, Kumar V, Borlaug BA, et al: Systolic-to-diastolic myocardial volume ratio as a novel imaging marker of cardiomyopathy. International Journal of Cardiology 322:272-277, 2021.
4. Soares JS, Li DS, Lai E, et al: Modeling of Myocardium Compressibility and its Impact in Computational Simulations of the Healthy and Infarcted Heart. Funct Imaging Model Heart 10263:493-501, 2017.
5. Kumar V, Manduca A, Rao C, et al: An under-recognized phenomenon: Myocardial volume change during the cardiac cycle. Echocardiography 38:1235-1244, 2021.
6. Rowin EJ, Maron BJ, Carrick RT, et al: Outcomes in Patients With Hypertrophic Cardiomyopathy and Left Ventricular Systolic Dysfunction. J Am Coll Cardiol 75:3033-3043, 2020.
7. Triposkiadis F, Giamouzis G, Boudoulas KD, et al: Left ventricular geometry as a major determinant of left ventricular ejection fraction: physiological considerations and clinical implications. Eur J Heart Fail 20:436-444, 2018.
8. Zhang Y, Wu KH, Li Q, et al: [Analysis on related factors of myocardial fibrosis in patients with hypertrophic cardiomyopathy]. Zhonghua Xin Xue Guan Bing Za Zhi 49:31-36, 2021.
9. Konno T, Hayashi K, Fujino N, et al: High sensitivity of late gadolinium enhancement for predicting microscopic myocardial scarring in biopsied specimens in hypertrophic cardiomyopathy. PLoS One 9:e101465, 2014.
Figures