1674
Highly accelerated CINE cardiac MR deep-learning image reconstruction in combination with compressed sensing: A quantitative evaluation.1Philips, Rochester, MN, United States, 2Department of Radiology, Mayo Clinic, Rochester, MN, United States
Synopsis
Keywords: Myocardium, Cardiovascular
Motivation: Deep-learning image reconstruction is promising for improving image quality and may enable higher acceleration for cardiac CINE MR.
Goal(s): To investigate deep-learning-based image reconstruction for accelerating cardiac CINE MRI over compressed sensing (CS) reconstructions without affecting quantitative measures of ejection fraction.
Approach: Cardiac CINE MR with CS factors 2-5 were acquired in 15 volunteers and reconstructed with one standard and two AI methods. Ejection fractions were calculated, and a subset of images were graded for image quality.
Results: CS-factors did not materially affect ejection fractions (left-ventricle p=0.969, right-ventricle p=0.998). Blurring (p<0.01) and perceived SNR (p<0.01) were improved by AI reconstruction at high acceleration.
Impact: Deep learning MR reconstruction reduces penalties from high acceleration in cardiac MRI CINE imaging, allowing for shorter breath-holds, shorter exams, non-compromised image quality, and preserved quantitative measurements.
Introduction
Cardiac MR CINE imaging is considered the standard for determination of cardiac chamber volumes and ejection fraction and is one of the most widely used MR techniques to visualize cardiac anatomy and function1. However, CINE acquisition takes several minutes and requires multiple breath-holds, which can be challenging for some patients. Reducing CINE acquisition time and improving patient comfort is of interest, methods include free-breathing2 and acquisition acceleration3. Acceleration incurs penalties including increased artifacts, requirement of accurate coil sensitivity maps, and reduced signal to noise ratio (SNR) and image sharpness. Deep-learning-based (DL) reconstruction methods are currently being investigated for improving image quality4,5, and may compensate for acceleration complications. We hypothesized that by applying DL reconstruction to CINE MRI, we could further accelerate acquisitions via compressive sensing without penalties to image quality or reliability of quantitative ejection fraction values, using standard reconstruction and two DL reconstruction methods.Methods
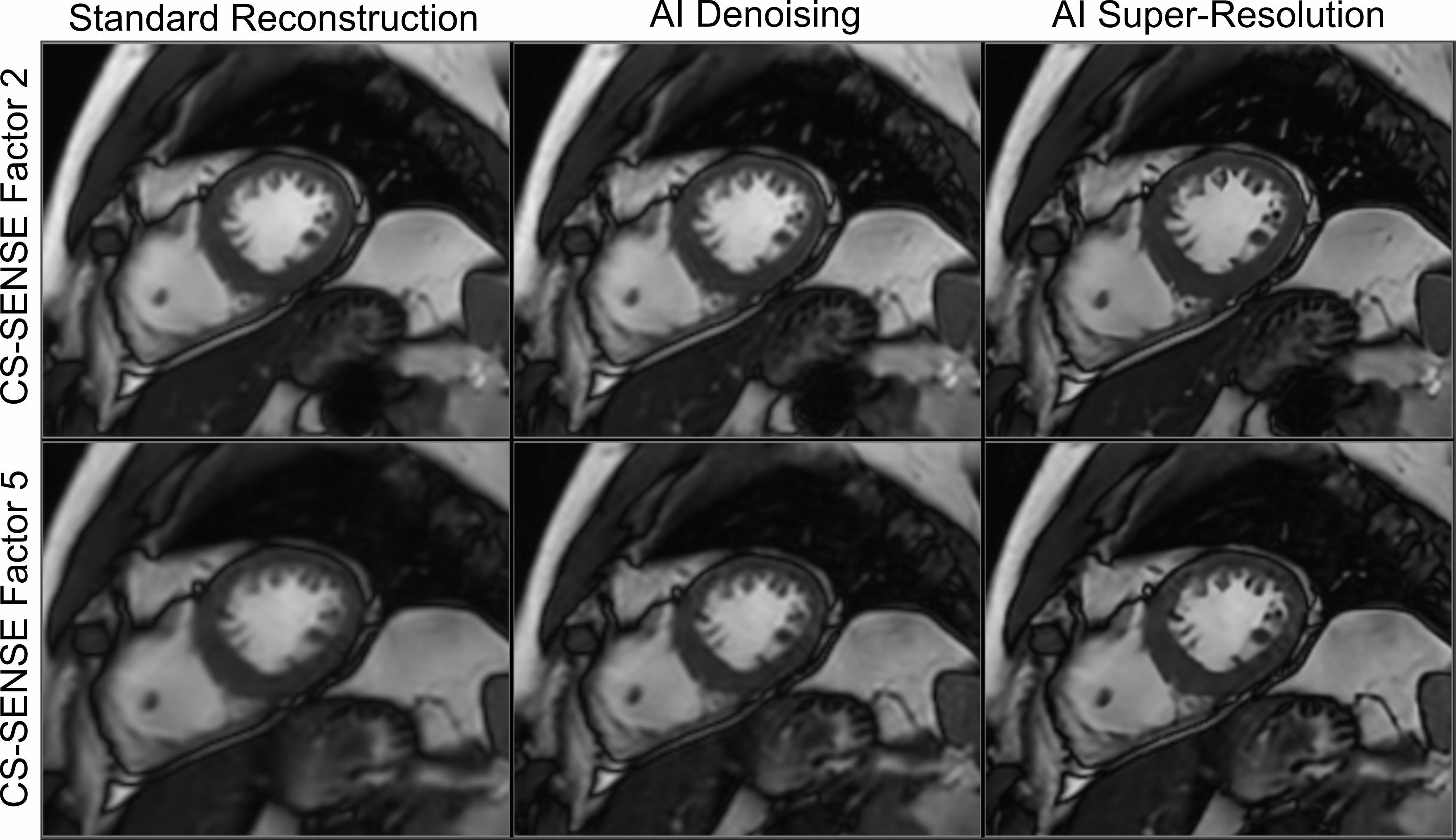
In this prospective study, 15 healthy subjects gave informed consent and underwent a cardiac MRI protocol on a 3.0T Philips (Best, The Netherlands) Elition X scanner with a 28-channel torso coil (16 anterior, 12 posterior). Age was 41.4±10.8 years, weight was 77.5±13 kg, and 9 participants were male. Reference images were acquired for 2-, 3-, and 4-chamber views in addition to four short axis (ShAx) multi-slice CINE acquisitions with variable Compressed Sensing (CS). ShAx CINE acquisitions had CS factors 2, 3, 4, and 5. Spatial resolution was kept constant at 2.1x1.9x8.0 mm, 15 slices. Other parameters were: balanced SSFP, echo-train length=8, and TR/TE=2.7/1.4 ms. The CS=2 acquisition had 12 second breath-holds with 1 slice/breath (Nominal acquisition duration 180s for full heart coverage), CS3 had 15s breath-holds with 2 slices/breath (113s nominal acquisition time), CS4 had 12s breath-holds with 2 slices/breath (90s nominal acquisition time), and CS5 had 15s breath-holds with 3 slices/breath (75s nominal acquisition time). Images were reconstructed with a standard nonlinear conjugate gradient reconstruction without DL, a DL-based denoised reconstruction, and DL-based reconstruction with AI super-resolution. For all ShAx CINE series, left- and right-ventricular end-systolic and end-diastolic volume as well as ejection fraction were recorded using deep-learning based contouring software (AI4CMR, Braga, Portugal).A cardiac radiologist with 20 years of experience, provided image quality gradings on a 4-point scale where 1 is best for overall-IQ, artifacts, blurring, and perceived signal-to-noise ratio (pSNR) for all CS factors and reconstruction techniques in a subset of subjects (n=5). The evaluator was blinded to acceleration factors and image reconstruction techniques.
A Kruskal-Wallis test comparing ejection fractions from all techniques was computed to test the stability of this metric for different acquisition and reconstruction protocols. A Wilcoxon rank-sum test was utilized for group-wise comparison of image quality metrics.
Results
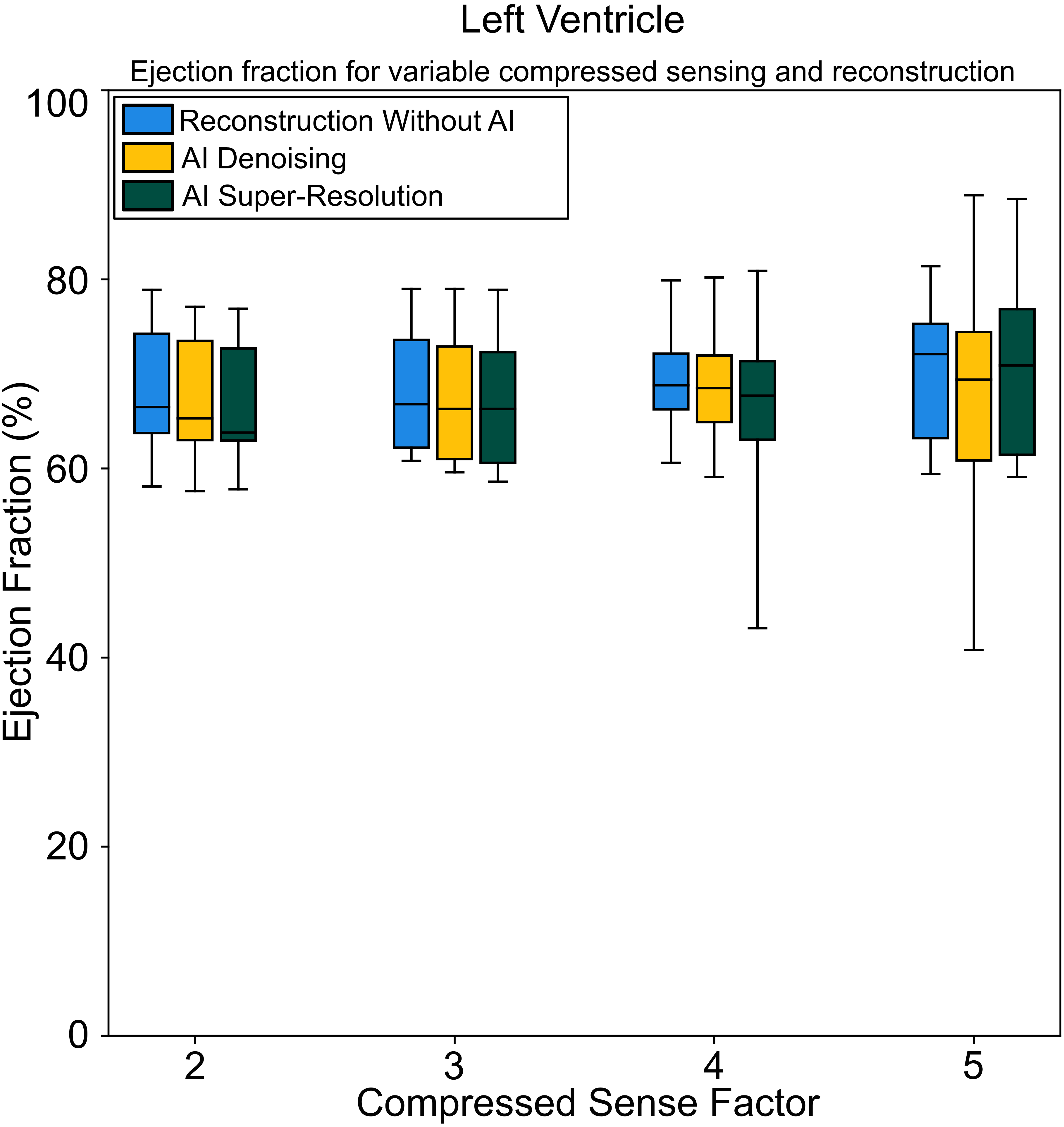
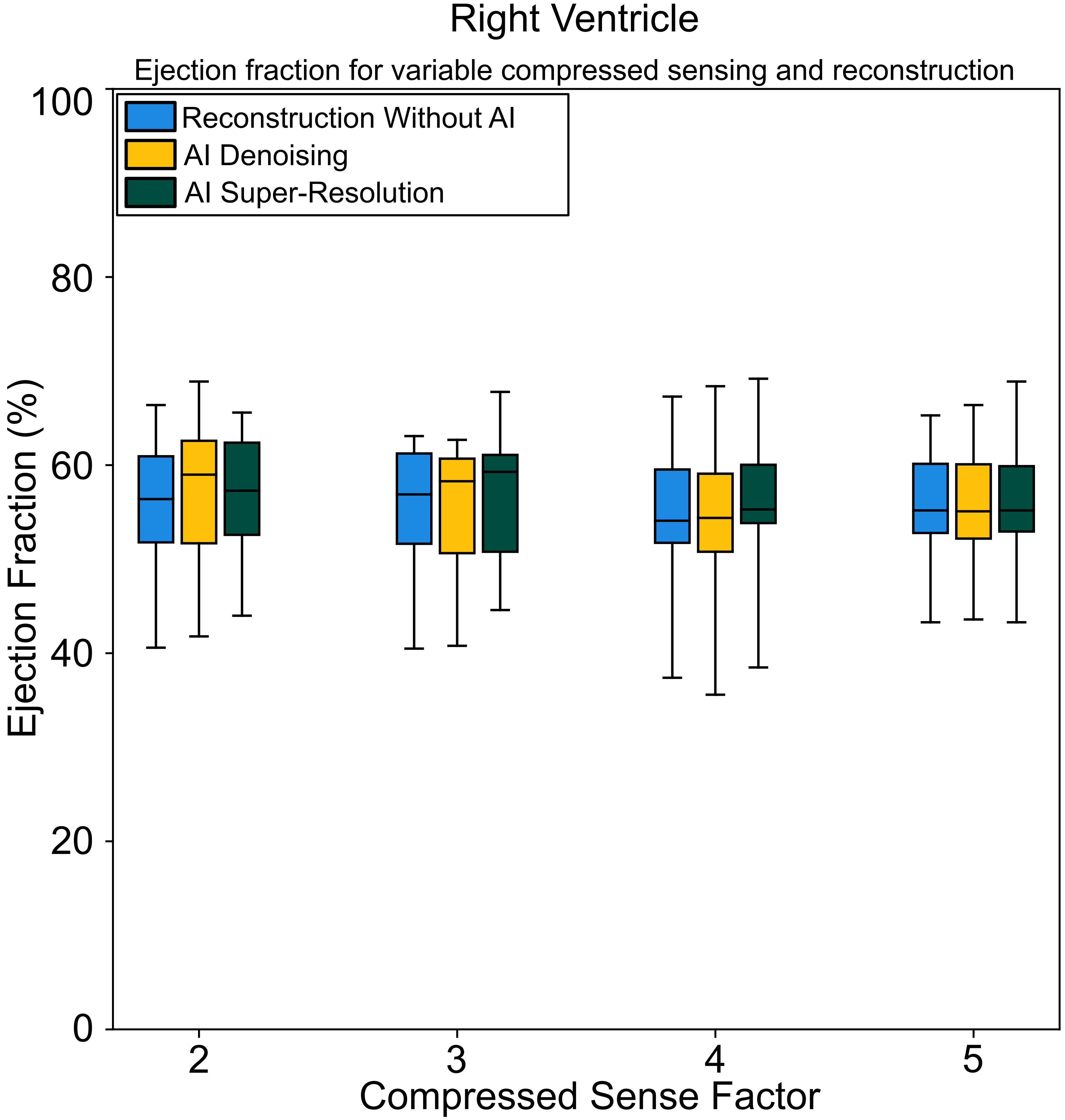
Figure 1 shows representative images, which demonstrate expected increased image noise with increasing CS factor, which is compensated for after DL reconstruction. Boxplots showing ejection fractions for the left ventricle are shown in Figure 2, and for the right ventricle in Figure 3. No difference in ejection fraction was detected between CS factor and acquisition method for either left (p=0.969) or right (p=0.998) ventricle.Image quality metrics indicated that all ShAx CINE acquisitions were diagnostic, and DL reconstruction methods resulted in improved IQ scores, lower artefacts, higher pSNR, and lower blurring. For all subjects, CS factor 5 resulted in reduced image quality without AI reconstruction; overall IQ was 2.0±0.0, blurring 2.4±0.5, pSNR 2.0±0.0, and aliasing 1.4±0.5. The same acquisitions reconstructed with DL super-resolution resulted in overall IQ scores of 1.4±0.5, blurring 1.0±0.0, pSNR 1.0±0.0, and aliasing 1.6±0.5. Blurring (p<0.01) and pSNR (p<0.01) were statistically improved.
Discussion
Deep-learning-based reconstruction techniques are novel methods anticipated to improve image quality and allow further increase in acquisition efficiency over existing acceleration techniques such as compressed sensing. However, the effect of DL reconstruction on interpretation of MRI is still being investigated. In this study, we enrolled 15 volunteers to evaluate three reconstruction methods for compressed sensing factors 2-5, and performed image quality gradings in a subset of images. We found that quantitative ejection fraction measurements were similar for all compressed sensing and reconstruction methods. Image quality was found to be improved for high compressed sensing factors when using DL reconstruction. These findings are promising for DL reconstruction in cardiac imaging. Future directions are to evaluate DL based image reconstruction in various cardiovascular pathologies and investigate additional methods of image acceleration, such as k-t acceleration.Conclusion
DL-based image reconstruction methods are promising for acquisition acceleration with reduced penalties to image quality and preserved quantitative measures of ejection fraction on cardiac MRI CINE exams.Acknowledgements
No acknowledgement found.References
1. Sakuma H, Fujita N, Foo TK, et al. Evaluation of left ventricular volume and mass with breath-hold CINE MR imaging. Radiology. 1993;188:377-380.
2. Leung AO, Paterson I, Thompson RB. Free-breathing CINE MRI. Magn Reson Med. 2008 Sep;60(3):709-17. doi: 10.1002/mrm.21711. PMID: 18727100.
3. Axel L, Otazo R. Accelerated MRI for the assessment of cardiac function. Br J Radiol. 2016 Jul;89(1063):20150655. doi: 10.1259/bjr.20150655. Epub 2016 Apr 21. PMID: 27033471; PMCID: PMC5257298.
4. Sandino CM, Lai P, Vasanawala SS, Cheng JY. Accelerating cardiac CINE MRI using a deep learning-based ESPIRiT reconstruction. Magn Reson Med. 2021 Jan;85(1):152-167. doi: 10.1002/mrm.28420. Epub 2020 Jul 22. PMID: 32697891; PMCID: PMC7722220.
5. Pednekar A, Kocaoglu M, Wang H, Tanimoto A, Tkach JA, Lang S, Taylor MD. Accelerated CINE Cardiac MRI Using Deep Learning-Based Reconstruction: A Systematic Evaluation. J Magn Reson Imaging. 2023 Oct 19. doi: 10.1002/jmri.29081. Epub ahead of print. PMID: 37855257.
Figures