1673
The value of left atrium in predicting reverse left ventricular remodeling in patients with ST-segment elevation myocardial infarction1Department of Radiology, the First Medical center, PLA General Hospital, Beijing, China, 2Department of Radiology, Beijing Jishuitan Hospital, Capital Medical University, Beijing, China, 3Philips Healthcare, Beijing, China
Synopsis
Keywords: Myocardium, Cardiovascular, Ventricular remodeling· Magnetic resonance imaging· ST elevation myocardial infarction· Left atrial reservoir strain rate
Motivation: Understanding reverse left ventricular remodeling (r-LVR) after ST-segment elevation myocardial infarction (STEMI) is important for patients. It is unknown whether left atrium (LA) volume and function can predict r-LVR.
Goal(s): The aim of study was to evaluate the changes in left heart structure and function by performing two cardiac magnetic resonance (CMR) scans and then to explore the value of LA in predicting r-LVR.
Approach: A total of 105 STEMI patients were studied. The predictors of r-LVR were analyzed by logistic regression method.
Results: LV end diastolic volume (LVEDV), total enhanced mass and LA reservoir strain rate were significantly predictors of r-LVR.
Impact: Our study described the natural course of the left heart over time in patients with STEMI, evaluated predictors of left heart for r-LVR, and found that LA reservoir strain rate and LV longitudinal displacement had similar value for predicting r-LVR.
Introduction
Reverse left ventricular remodeling (r-LVR) is associated with improved ST-segment elevation myocardial infarction (STEMI) patient prognosis[1]. Cardiac magnetic resonance (CMR) is a good tool for determining r-LVR and exploring the course of chronic changes in the LV after STEMI because it accurately measures changes in LV volume and function[2]. In recent years, the importance of left atrium (LA) has been introduced. LA function is closely related to changes in overall cardiac function, and the size of the LA is an independent prognostic indicator for various cardiac diseases[3]. However, it is still unknown whether LA volume and function can predict r-LVR after STEMI. The aim of study was to evaluate the changes in left heart structure and function by performing two cardiac magnetic resonance (CMR) scans in STEMI patients and then to explore the value of LA in predicting r-LVR.Methods
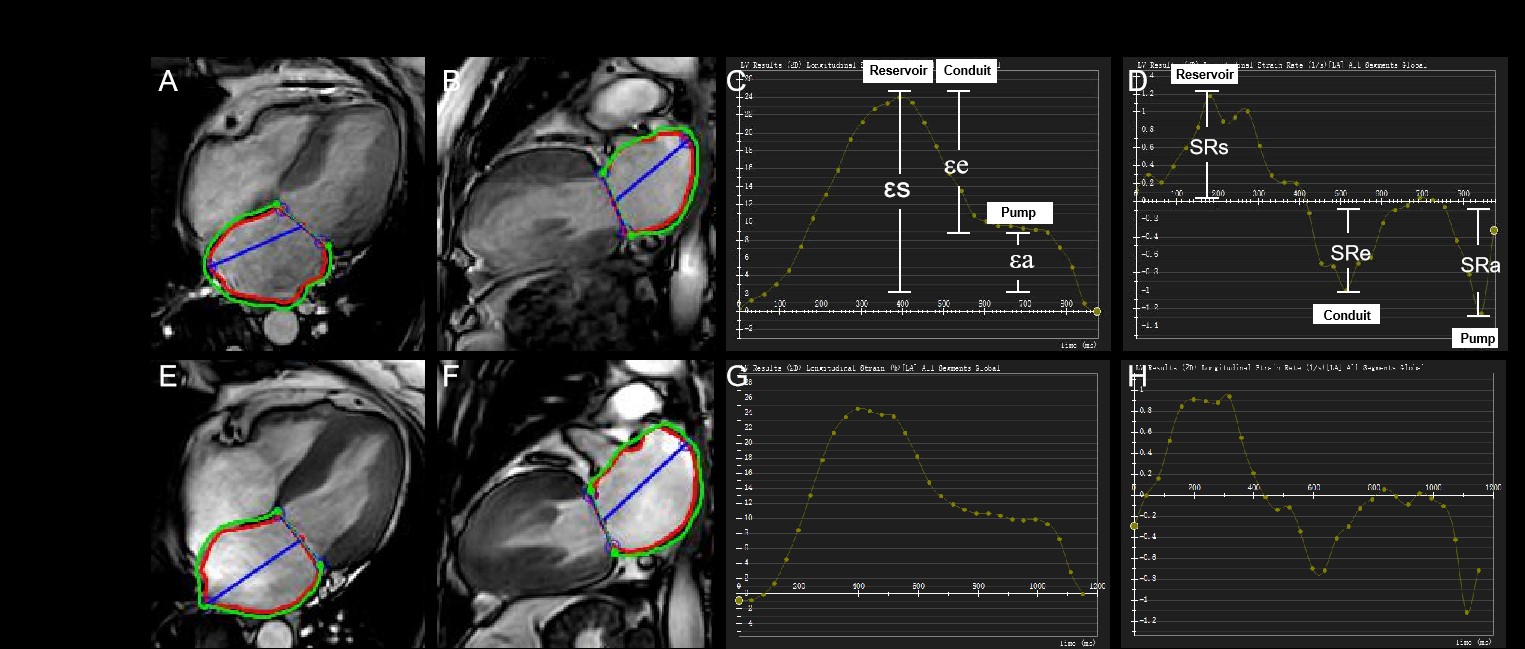
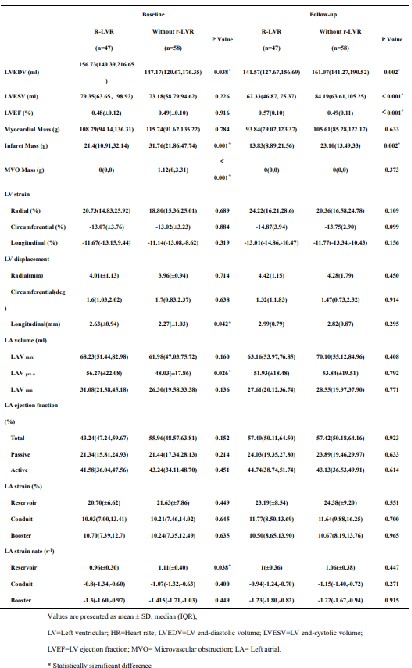
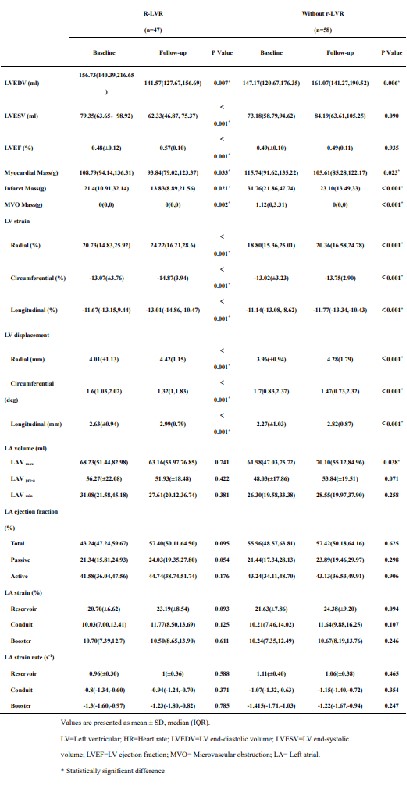
A total of 105 STEMI patients were retrospectively studied. There were 47 patients in r-LVR group and 58 patients in without r-LVR group. CMR analysis included left heart volume, infarct characteristics, myocardial function. The strain and strain rate were assessed by CMR feature tracking. R-LVR was defined as a reduction of 10% or more in the left ventricular end systolic volume (LVESV) at the second CMR compared with baseline CMR. The predictors of r-LVR were analyzed by logistic regression method.Results
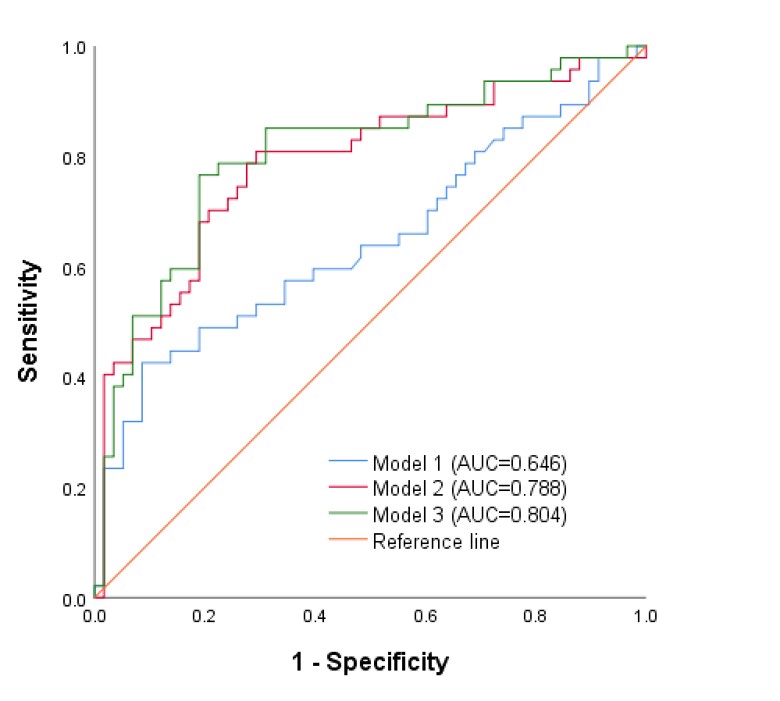
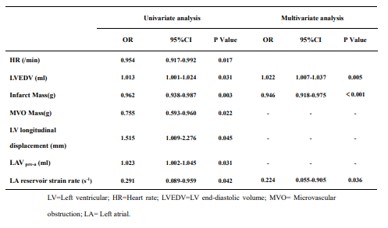
At first CMR, r-LVR group had higher left heart volume and LV longitudinal displacement as well as lower myocardial injury and LA reservoir strain rate (all P<0.05). At second CMR, r-LVR group had lower LV volume and infarct mass as well as greater left ventricular ejection fraction (LVEF) (all P<0.05). Of note, left ventricular end diastolic volume (LVEDV) [odds ratio: 1.022 (1.007–1.037), P=0.005], infarct mass [odds ratio: 0.946 (0.918–0.975), P<0.001] and LA reservoir strain rate [odds ratio: 0.224 (0.055–0.905), P=0.036] were independent predictors of r-LVR. In order to investigate the predictor value of CMR parameters in LV and LA, we built 3 different models to compare the predictive ability. The model 1 was baseline model, including age and HR. The AUC of model 1 was 0.646 (95% CI 0.537–0.755). The model 2 included model 1 plus LVEDV, infarct mass, MVO mass and LV longitudinal displacement. The AUC of model 2 was 0.788 (95% CI 0.697–0.878). The model 3 was to replace the LV longitudinal displacement of model 2 with the LA reservoir strain rate. The AUC of model 3 was 0.804 (95% CI 0.716–0.892). We observed that there was no significant difference of AUC between model 2 and model 3 (P=0.453), but AUC were significantly higher in model 2 and model 3 compared with model 1(P=0.009 and P=0.003, respectively).Discussion
The LA strain was better predictor of r-LVR than LAV (LA volume) for the following reasons. First, LA function can predict hemodynamics more effectively. Bergstra et al. [4] found that many STEMI patients exhibited increased left-sided cardiac filling pressures, LAV max didn’t seem to be influenced by changes in LV filling or acute ischemia[5], while LA strain was associated with LV filling pressure[6]. Secondly, atrial fibrillation is the most common arrhythmia after MI[7], and LA strain predicts new-onset atrial fibrillation in MI patients, leading to LV dysfunction. In our study, we found the reservoir strain rate was the only parameter among LA strain rates that was able to predict r-LVR. The reasons were as followed. First, the atrioventricular plane shift is a major contributor to passive LA reservoir function, so changes in LVESV in STEMI patients causing atrioventricular plane shift may affect LA reservoir function[8]. Second, the LA reservoir occurs before LV diastole, whereas the conduit and pump phases occur during LV diastole[9], so the LA reservoir was first impaired when there was a significant change in LV volume, which may be the earliest detectable LA parameter of predicting r-LVR in patients with STEMI. In addition, Antoni et al.[10] investigated the importance of LA strain in STEMI prognosis and found that LA reservoir strain was an independent predictor of MACE. In addition to LA reservoir strain rate, our analysis showed that LVEDV and total enhanced mass were also significant independent predictors of r-LVR , which was consistent with previous finding[11, 12].Conclusions
LVEDV, total enhanced mass and LA reservoir strain rate were significantly predictors of r-LVR in STEMI patients. LA reservoir strain rate and LV longitudinal displacement had similar values for predicting r-LVR.Acknowledgements
No acknowledgement found.References
References [1] Cheng S, Vasan RS. Advances in the epidemiology of heart failure and left ventricular remodeling. Circulation. 2011. 124(20): e516-9. [2] Groot HE, Al Ali L, van der Horst I, et al. Plasma interleukin 6 levels are associated with cardiac function after ST-elevation myocardial infarction. Clin Res Cardiol. 2019. 108(6): 612-621. [3] Abhayaratna WP, Seward JB, Appleton CP, et al. Left atrial size: physiologic determinants and clinical applications. J Am Coll Cardiol. 2006. 47(12): 2357-63. [4] Bergstra A, Svilaas T, van Veldhuisen DJ, van den Heuvel AF, van der Horst IC, Zijlstra F. Haemodynamic patterns in ST-elevation myocardial infarction: incidence and correlates of elevated filling pressures. Neth Heart J. 2007. 15(3): 95-9. [5] Barbier P, Solomon SB, Schiller NB, Glantz SA. Left atrial relaxation and left ventricular systolic function determine left atrial reservoir function. Circulation. 1999. 100(4): 427-36. [6] Singh A, Addetia K, Maffessanti F, Mor-Avi V, Lang RM. LA Strain for Categorization of LV Diastolic Dysfunction. JACC Cardiovasc Imaging. 2017. 10(7): 735-743. [7] Reinstadler SJ, Stiermaier T, Eitel C, et al. Impact of Atrial Fibrillation During ST-Segment-Elevation Myocardial Infarction on Infarct Characteristics and Prognosis. Circ Cardiovasc Imaging. 2018. 11(2): e006955. [8] Cau R, Bassareo P, Suri JS, Pontone G, Saba L. The emerging role of atrial strain assessed by cardiac MRI in different cardiovascular settings: an up-to-date review. Eur Radiol. 2022. 32(7): 4384-4394. [9] Rossi A, Gheorghiade M, Triposkiadis F, Solomon SD, Pieske B, Butler J. Left atrium in heart failure with preserved ejection fraction: structure, function, and significance. Circ Heart Fail. 2014. 7(6): 1042-9. [10] Leng S, Ge H, He J, et al. Long-term Prognostic Value of Cardiac MRI Left Atrial Strain in ST-Segment Elevation Myocardial Infarction. Radiology. 2020. 296(2): 299-309. [11] D'Elia N, D'hooge J, Marwick TH. Association Between Myocardial Mechanics and Ischemic LV Remodeling. JACC Cardiovasc Imaging. 2015. 8(12): 1430-1443. [12] Galloo X, Stassen J, Hirasawa K, et al. Impact of baseline left ventricular volume on left ventricular reverse remodeling after cardiac resynchronization therapy. Heart Rhythm. 2022. 19(6): 927-936.Figures