1672
Biventricular intraventricular mechanical dyssynchrony and electronical dyssynchrony in pulmonary arterial hypertension1Fuwai Hospital, Chinese Academy of Medical Sciences, Beijing, China, 2MR Research Collaboration, Siemens Healthineers Ltd., Beijing, China, 3MR Application Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany, 4Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, China
Synopsis
Keywords: Myocardium, Myocardium, pulmonary hypertension; mechanical dyssynchrony;
Motivation: The ability of layer-specific intraventricular mechanical dyssynchrony (M-dys) to predict prognosis in pulmonary arterial hypertension (PAH) has not been investigated.
Goal(s): To illustrate the existence and prognostic values of layer-specific intraventricular M-dys and its associations with electronical dyssynchrony in PAH.
Approach: The biventricular volumetric and layer-specific intraventricular M-dys were analyzed by calculating strain and strain rate based on cine cardiac magnetic resonance images.
Results: The layer-specific intraventricular M-dys had varying impacts on biventricular functions in PAH.
Impact: This study was novel in reporting that the layer-specific intraventricular M-dys had various distribution patterns in both ventricles in patients with PAH.
Introduction
Pulmonary arterial hypertension (PAH) can lead to myocardial remodeling, manifesting as mechanical dyssynchrony (M-dys) and electronical dyssynchrony (E-dys) in both right (RV) and left ventricles (LV). However, the impacts of intraventricular M-dys and its direct associations with E-dys in PAH are not clear. The distribution patterns of layer-specific intraventricular M-dys measured by cardiac magnetic resonance (CMR), which reflects non-uniform contractile function within ventricles, and its ability to predict prognosis in PAH have not been reported. The purpose of this study is to illustrate the existence and prognostic values of layer-specific intraventricular M-dys and its associations with E-dys in PAH.Methods
Seventy-nine newly diagnosed PAH patients by right heart catherization (RHC) from a prospective registry1 and agreed to undergo CMR scanning were consecutively recruited between January 2011 and December 2017. All enrolled patients received RHC and CMR scanning within one week at the baseline. CMR was performed on a 1.5 T scanner (MAGNETOM Avanto, Siemens Healthcare, Erlangen, Germany). Breath-hold short-axis cine images encompassing the whole LV and RV from apex to base were acquired using balanced steady-state free-precession (bSSFP) sequence (repetition time/echo time, 3.2 ms/1.6 ms; temporal resolution, 34 ms; flip angle, 60 degrees; field of view, 280×340 mm2; matrix, 150×256; voxel size, 1.9mm×1.3mm; slice thickness, 8 mm). Acquired CMR images were analyzed using a research software (Trufi Strain V2.1, Siemens Healthineers AG, Erlangen, Germany). This software uses a deformation registration algorithm to calculate the myocardial strain on a pixel basis, which could be used to analyze the layer-specific strain and strain rate based on cine CMR (DRA-CMR). Comprehensive analysis of biventricular volumetric and intraventricular M-dys were also performed using Trufi Strain V2.1. Twelve-lead ECGs were collected a day before RHC with standard settings of 25 mm/s speed and 10-mm/mV amplitude. QRS duration was described as the widest interval in any of the 12 leads and was acquired digitally2. The QRS duration z-score were calculated adjusting by age and gender3, with E-dys defined as z-score ≥2.Results
77.22% of enrolled patients were female, with a mean age of 30.30 ± 9.79 years. The median follow-up was 2018 days (26 to 3990 days). 29 (36.71%) patients succumbed to all-cause mortality by the end of study. The baseline LV layer-specific intraventricular M-dys had obvious transmural gradients in the radial and circumferential directions from endocardial to epicardial layers compared to RV (Table 1). However, deceased PAH patients lost the transmural gradients of layer-specific intraventricular M-dys in LV (Table 2). LV longitudinal strain rate time to late diastolic peak in myocardial region (LVmyoLSRTTLDP) was predictive of long-term survival (AUC: 0.645, p = 0.038). The Kaplan-Meyer curve showed PAH patients with LVmyoLSRTTLDP < 20.01ms might have a worse prognosis (Figure 1, Log rank p = 0.018). Multivariate Cox regression analysis showed after adjusted by peak VO2 pred, RHC-cardiac index, diastolic pulmonary arterial pressure, or pulmonary vascular resistance, LVmyoLSRTTLDP < 20.01ms could independently predict mortality. Larger RV intraventricular M-dys resulted in worse CMR derived RV ejection fraction. However, larger LV intraventricular M-dys indicated good exercise capacity (larger 6-minute walk distance and peak VO2) and higher CMR-derived LV stoke volume index (LVSVI). No direct associations were found between E-dys and intraventricular M-dys in PAH. In addition, E-dys had no impact on the long-term prognosis of PAH.Discussion
This study was novel in reporting that the LV layer–specific intraventricular M-dys had noticeable transmural gradients in the radial and circumferential directions compared with RV in patients with PAH. Deceased patients with PAH lost the transmural gradients of LV layer–specific intraventricular M-dys. E-dys had no direct correlations with intraventricular M-dys, consistent with previous findings. Therefore, we speculated that the reorientations of myocytes in both ventricles caused a nonuniform contraction. Patients with PAH with LVmyoLSRTTLDP <20.01 milliseconds had a worse long-term prognosis. We speculated that the larger LV intraventricular M-dys in the late diastolic phase might result in longer time to filling, contributing to larger LVSVI. The intraventricular M-dys in the late diastolic phase in the LV needs more attention.Conclusion
The layer-specific intraventricular M-dys not only have different distribution patterns in LV and RV, but also might have different impacts on biventricular function in PAH. CMR derived LV intraventricular M-dys in the longitudinal direction might help to predict the long-term prognosis in PAH.Acknowledgements
This study was supported by grants from the National Key Research and Development Program of China (No. 2016YFC1304400) and Youth Foundation of Fuwai Hospital (Grant number: 2022-FWQN06).References
1. Quan R, Zhang G, Yu Z, et al. Characteristics, goal-oriented treatments and survival of pulmonary arterial hypertension in China : Insights from a national multicentre prospective registry. Respirology 2022;27:517-528. doi: 10.1111/resp.14247.
2. Yang X wei, Hua W, Wang J, et al. Native QRS narrowing reflects electrical reversal and associates with anatomical reversal in cardiac resynchronization therapy. J Interv Card Electrophysiol. 2014;41:161-168. doi: 10.1007/s10840-014-9936-5.
3. Chubb H, Ceresnak SR, Motonaga KS, Dubin AM. A proposed method for the calculation of age-dependent QRS duration z-scores. J Electrocardiol 2020;58:132-134. doi: 10.1016/j.jelectrocard.2019.12.004.
Figures
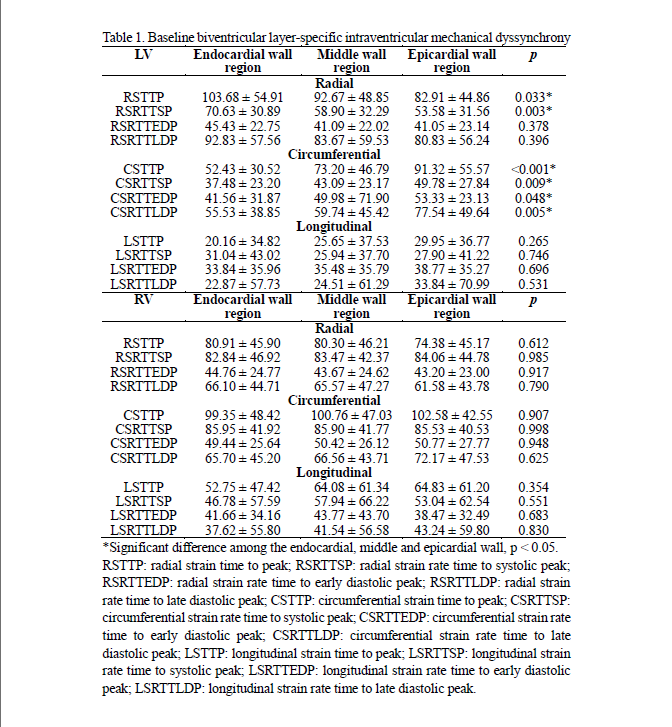
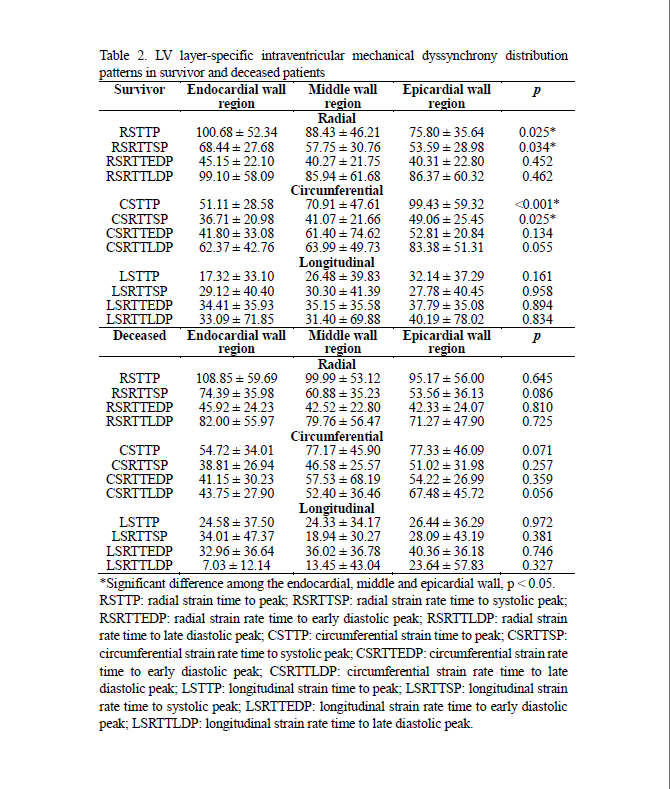
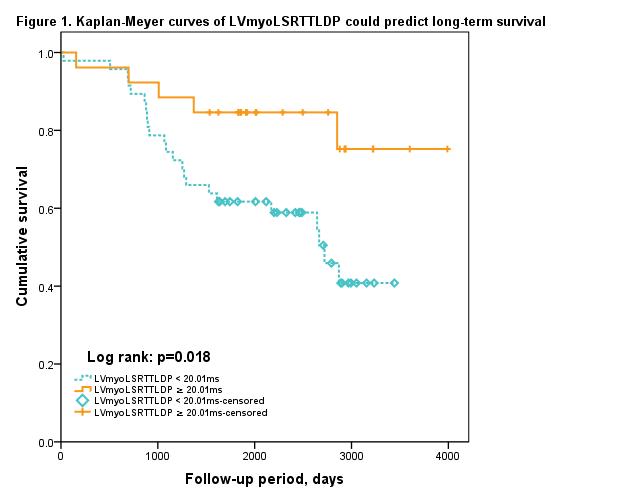
Figure 1.Kaplan-Meyer curve of LVmyoLSRTTLDP could predict long-term survival